Page 2 of 23
PA29.6-8 | Cervicitis, Endometriosis & Adenomyosis — SDL Guide (Part 2)
Endometriosis: Definition, Theories of Origin
Endometriosis is defined as the presence of endometrial glands and stroma outside the uterine cavity. It is a benign but hormonally driven, often progressive condition.
Epidemiology: Affects ~10% of women of reproductive age; up to 30–40% of women with infertility; peak incidence 25–35 years.
Hormonal dependence:
Endometriotic foci are estrogen-dependent — they undergo cyclic proliferation and bleeding under the influence of estrogens, just like eutopic endometrium. This explains:
• Why symptoms are worst perimenstrually.
• Why the disease remits during pregnancy (progesterone dominance) and after menopause (estrogen withdrawal).
• Why medical treatment targets estrogen suppression (combined OCP, GnRH agonists, progestogens).
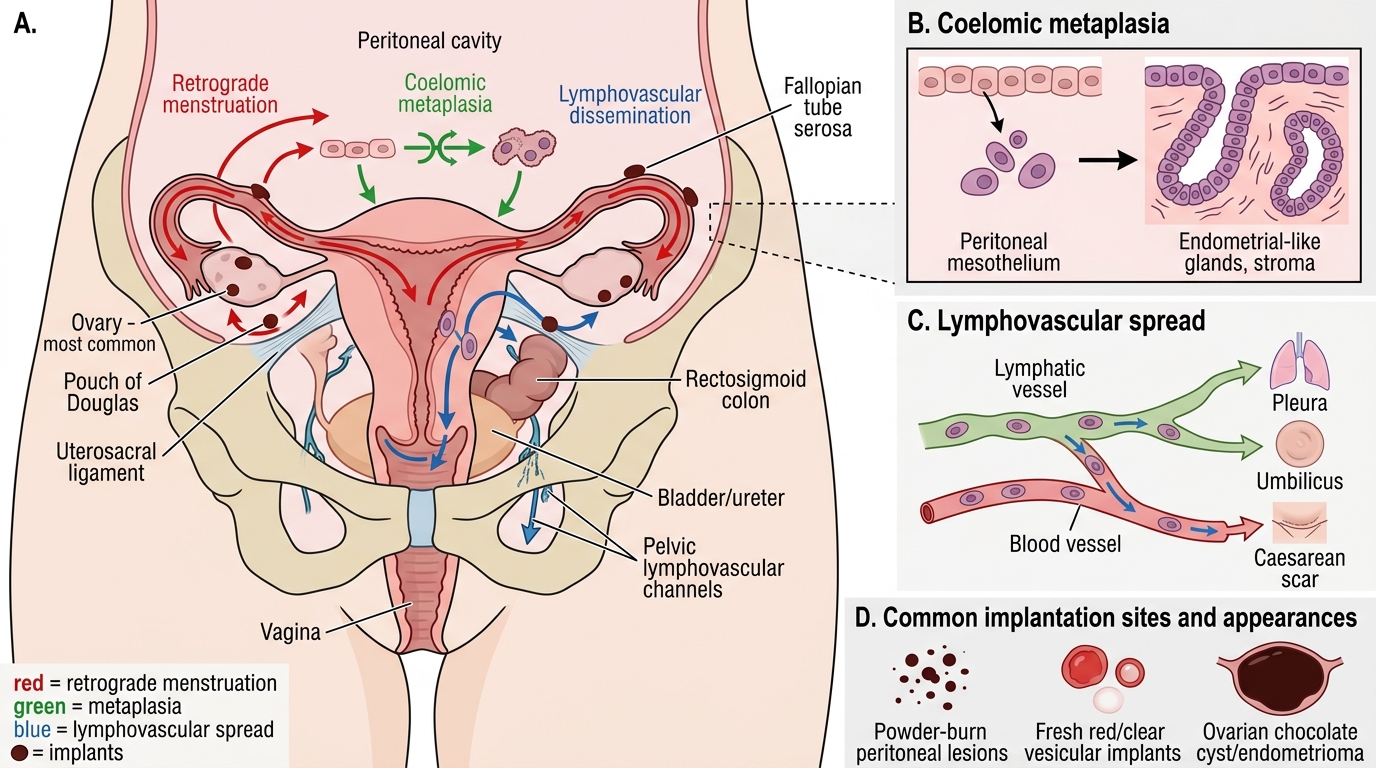
Theories of origin — the 'where did these cells come from?' debate:
- Retrograde menstruation theory (Sampson, 1927) — Most widely accepted. Menstrual debris flows backward through the fallopian tubes into the peritoneal cavity. Viable endometrial cells implant on peritoneal surfaces and proliferate. Supported by: (a) retrograde menstruation occurs in 90% of menstruating women; (b) endometriosis is most common in the dependent peritoneal recesses (pouch of Douglas, ovaries, uterosacral ligaments).
- Coelomic metaplasia theory (Meyer) — Totipotent coelomic mesothelial cells lining the peritoneum undergo metaplastic transformation into endometrial-type cells under hormonal or inflammatory stimuli. Explains rare cases in males (on estrogen therapy) and in sites inaccessible to retrograde flow (e.g., pleura, pericardium).
- Induction/vascular-lymphatic theory (Halban) — Endometrial fragments are transported hematogenously or via lymphatics to distant sites (lung, skin, lymph nodes, even the brain — very rare).
In practice, multiple mechanisms likely operate simultaneously in different patients and sites.
Theories of Endometriosis Origin and Implantation Sites
Endometriosis: Sites and Macroscopic Appearances
Common sites of endometriosis (in descending frequency):
- Ovaries — most common (60–80% of cases); bilateral in 30%.
- Pouch of Douglas (rectouterine pouch) and uterosacral ligaments.
- Fallopian tubes — peritoneal surface and serosa.
- Rectosigmoid colon — can cause cyclical rectal bleeding or obstruction.
- Urinary bladder and ureters — cyclical haematuria.
- Cervix, vagina, vulva — less common.
- Distant sites — pleura (catamenial pneumothorax), umbilicus (Villar's nodule), surgical scars (caesarean section scar endometriosis).
Macroscopic appearances:
- Powder-burn lesions (peritoneal implants): Small, punctate, dark brown or red-black deposits on peritoneal surfaces — the color comes from old haemorrhage (hemosiderin and haematin). Also called 'gunshot lesions' at laparoscopy. Fresh implants may be red or vesicular (clear/yellow) — these are more active and easily overlooked.
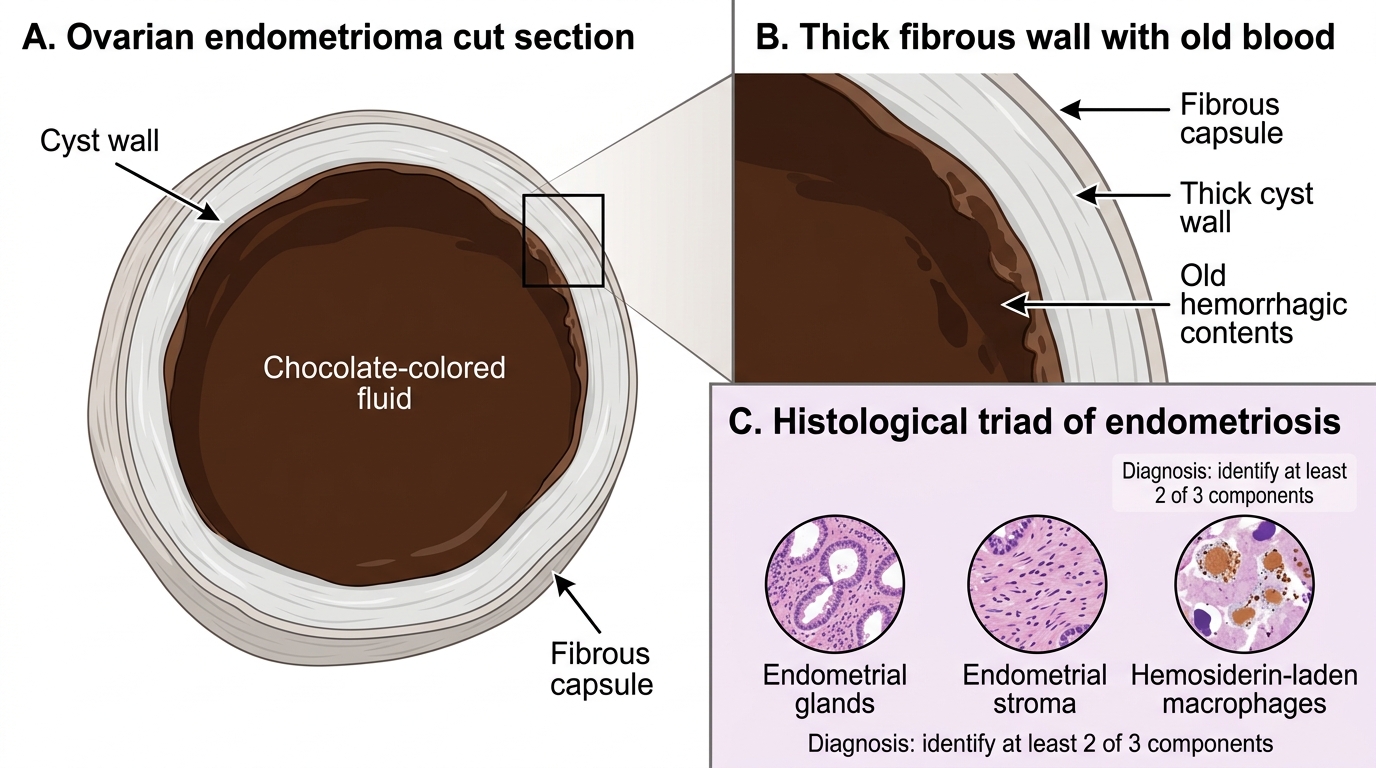
- Chocolate cyst (endometrioma): Endometriosis within the ovary forms a cyst lined by endometrial-like tissue that bleeds cyclically. The accumulated dark, tarry, old blood resembles melted chocolate — hence the name. These cysts are typically 1–10 cm; wall is thick and fibrous; cyst contents = dark viscous fluid.
- Fibrosis and adhesions: Repeated cycles of bleeding → inflammation → fibrosis → dense fibrous adhesions that bind the uterus, tubes, ovaries, bowel, and bladder together ('frozen pelvis' in severe disease).
Ovarian Endometrioma: Chocolate Cyst Cut Section
Endometriosis: Microscopy and Histological Diagnosis
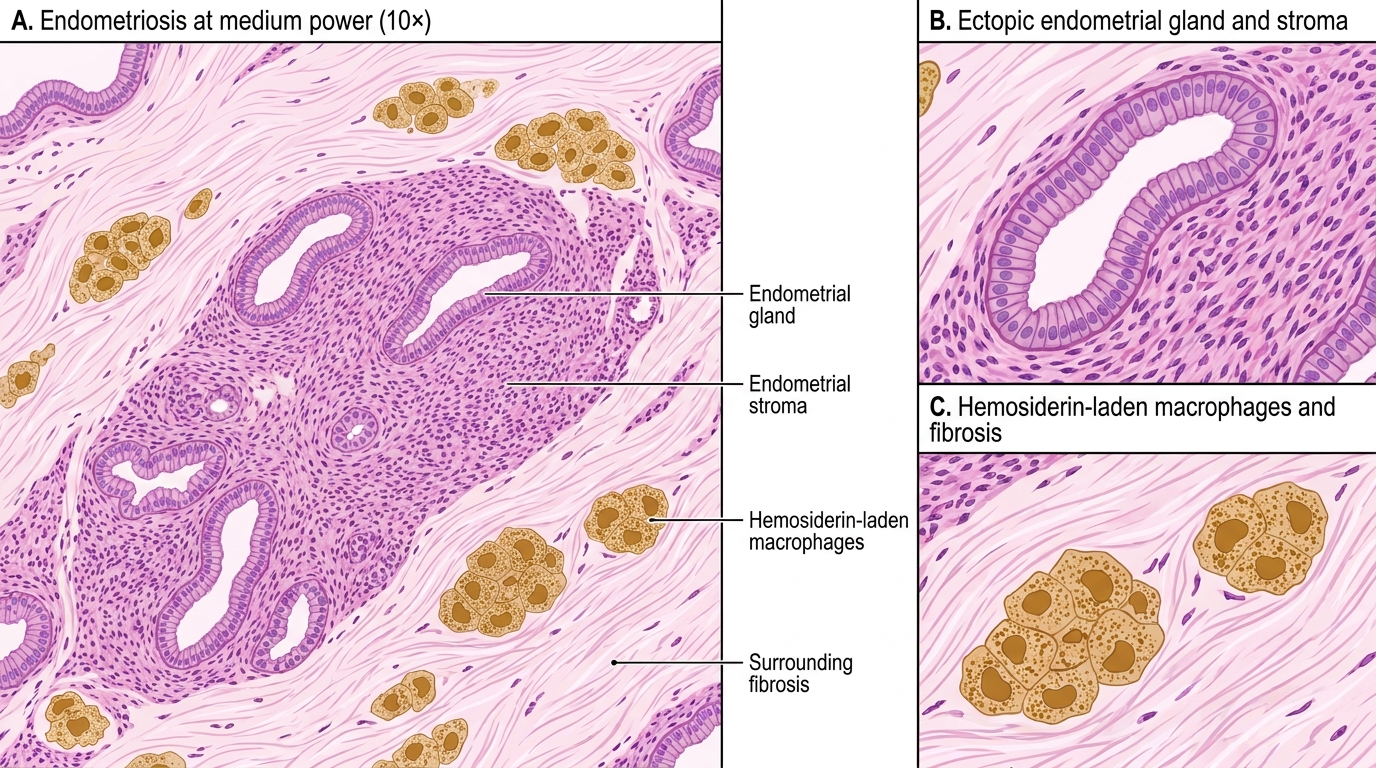
The histological diagnosis of endometriosis requires identification of at least TWO of the following three components (the classic triad):
- Endometrial glands — lined by columnar epithelium identical to eutopic endometrial glands; may show proliferative or secretory changes under hormonal influence.
- Endometrial stroma — spindle-shaped stromal cells (CD10 positive immunohistochemically) surrounding the glands.
- Hemosiderin-laden macrophages (siderophages) — brown, granular, iron-positive pigment within macrophages; evidence of prior haemorrhage; stain golden-brown on H&E, positive on Perls' Prussian blue stain.
Why is the triad important? In older or regressed lesions, the epithelium may be lost or attenuated due to repeated bleeding and fibrosis. In such cases, stroma alone with hemosiderin may be the only clue — and immunohistochemistry (CD10 for stroma, ER/PR for glands) can confirm the diagnosis.
The 'burnt-out' endometriosis trap: Fibrotic nodules on the peritoneum or bowel may lack glands entirely after years of disease. A clinician who biopsies a firm nodule suspicious for endometriosis but sees only fibrosis and hemosiderin should not dismiss the diagnosis — this is regressed endometriosis.
Histology of Endometriosis