Page 3 of 23
PA29.6-8 | Cervicitis, Endometriosis & Adenomyosis — SDL Guide (Part 3)
Endometriosis: Clinical Features and Complications
Classic triad of clinical features:
- Dysmenorrhea (cyclical pelvic pain beginning 2–3 days before menstruation) — this is secondary dysmenorrhea (a structural cause exists), distinguishing it from primary dysmenorrhea (no structural pathology).
- Dyspareunia (pain during intercourse) — from fibrosis and adhesions in the pouch of Douglas and uterosacral ligaments.
- Infertility — multifactorial: (a) peritubal adhesions obstruct sperm/egg transport; (b) altered peritoneal fluid environment (prostaglandins, macrophages) impairs fertilization; (c) ovarian endometriomas distort folliculogenesis.
Additional features:
• Cyclical rectal bleeding or haematuria (if bowel/bladder involved).
• Catamenial pneumothorax (right-sided, coincides with menstruation — diaphragmatic implants).
• Pelvic examination findings: retroverted fixed uterus, tender nodules in the pouch of Douglas, fixed adnexal masses.
Complications:
| Complication | Mechanism |
|---|---|
| Infertility | Adhesions, toxic peritoneal environment, ovarian dysfunction |
| Ectopic pregnancy | Tubal distortion from peritubal adhesions |
| Malignant transformation | Rare (~1%); endometrioid adenocarcinoma or clear cell carcinoma of ovary arising in endometrioma |
| Bowel obstruction | Fibrosis encasing sigmoid colon |
| Catamenial pneumothorax | Diaphragmatic/pleural implants |
CLINICAL PEARL
Pearl: 'Retroversion alone means nothing; fixed retroversion means everything.'
A retroverted uterus is a normal anatomical variant in 20–30% of women and is clinically insignificant in isolation. What matters is mobility. In endometriosis, fibrosis and adhesions in the posterior cul-de-sac anchor the uterus posteriorly — it becomes fixed and immobile on bimanual examination, and any movement elicits exquisite pain. When you combine a fixed retroverted uterus with secondary dysmenorrhea and a history of infertility in a young woman, your first diagnosis until proven otherwise is endometriosis.
SELF-CHECK
A 26-year-old woman undergoes laparoscopy for infertility workup. The surgeon describes 'dark brown punctate deposits on the posterior leaf of the broad ligament and uterosacral ligaments, plus a 5 cm left ovarian cyst with chocolate-colored contents.' Biopsy of the ovarian cyst wall is sent to histopathology. Which of the following microscopic findings would CONFIRM the diagnosis?
A. Glands lined by tall columnar epithelium, endometrial-type stroma, and hemosiderin-laden macrophages
B. Simple cuboidal glands within a smooth muscle wall with stromal edema
C. Granulomatous inflammation with Langhans giant cells and central caseous necrosis
D. Fibrous wall with flattened epithelium and serous fluid content
Reveal Answer
Answer: A. Glands lined by tall columnar epithelium, endometrial-type stroma, and hemosiderin-laden macrophages
Option A describes the diagnostic triad of endometriosis: endometrial-type glands, stroma, and evidence of prior haemorrhage (hemosiderin-laden macrophages). Option B describes adenomyosis (glands within myometrium). Option C is a granulomatous lesion (e.g., tuberculous salpingo-oophoritis). Option D is a simple serous cyst. At least two of the three triad components are required for histological diagnosis.
Adenomyosis: Definition, Etiology, and Morphology
Adenomyosis is defined as the presence of endometrial glands and stroma within the myometrium (uterine smooth muscle wall), at a depth of more than 2.5 mm below the endomyometrial junction. It is sometimes called 'internal endometriosis,' but this term is misleading and should be avoided because the pathogenesis and clinical associations differ substantially from true (external) endometriosis.
Etiology and pathogenesis:
Adenomyosis is thought to arise by direct downgrowth (invagination) of the basal endometrium into the myometrium — not by the implantation or metaplastic mechanisms proposed for endometriosis. Risk factors:
• Multiparity — repeated pregnancy-related remodeling of the endomyometrial junction weakens the barrier.
• Prior uterine instrumentation (dilatation and curettage, caesarean section, myomectomy) — disrupts the endomyometrial interface.
• Elevated estrogen — adenomyosis is an estrogen-responsive condition (though less dramatically so than endometriosis).
• Most common in perimenopausal multiparous women (35–50 years), contrasting with endometriosis (younger nulliparous/low-parity women).
Macroscopic morphology:
• Uterus is diffusely enlarged, globular, and boggy (bulky uterus); typically 200–300 g (normal uterine weight: ~70 g).
• On cut section: trabeculated myometrium with small, poorly defined hemorrhagic foci (old blood within ectopic glands).
• No capsule — this distinguishes adenomyosis from leiomyoma (which has a fibrous pseudocapsule and 'whorled' cut surface).
Microscopic morphology:
• Endometrial glands and stroma are present within the myometrium, surrounded by hypertrophic smooth muscle bundles (reactive myometrial hypertrophy).
• The glands are predominantly basalis-type (non-functioning, non-secretory — recall: the basalis does not respond to hormones in the same way as the functionalis).
• Hemosiderin may be present but is less conspicuous than in endometriosis.
• Distance from the endomyometrial junction must exceed 2.5 mm (one high-power field at 40× from the junction) to distinguish from normal basal endometrium dipping slightly into the superficial myometrium.
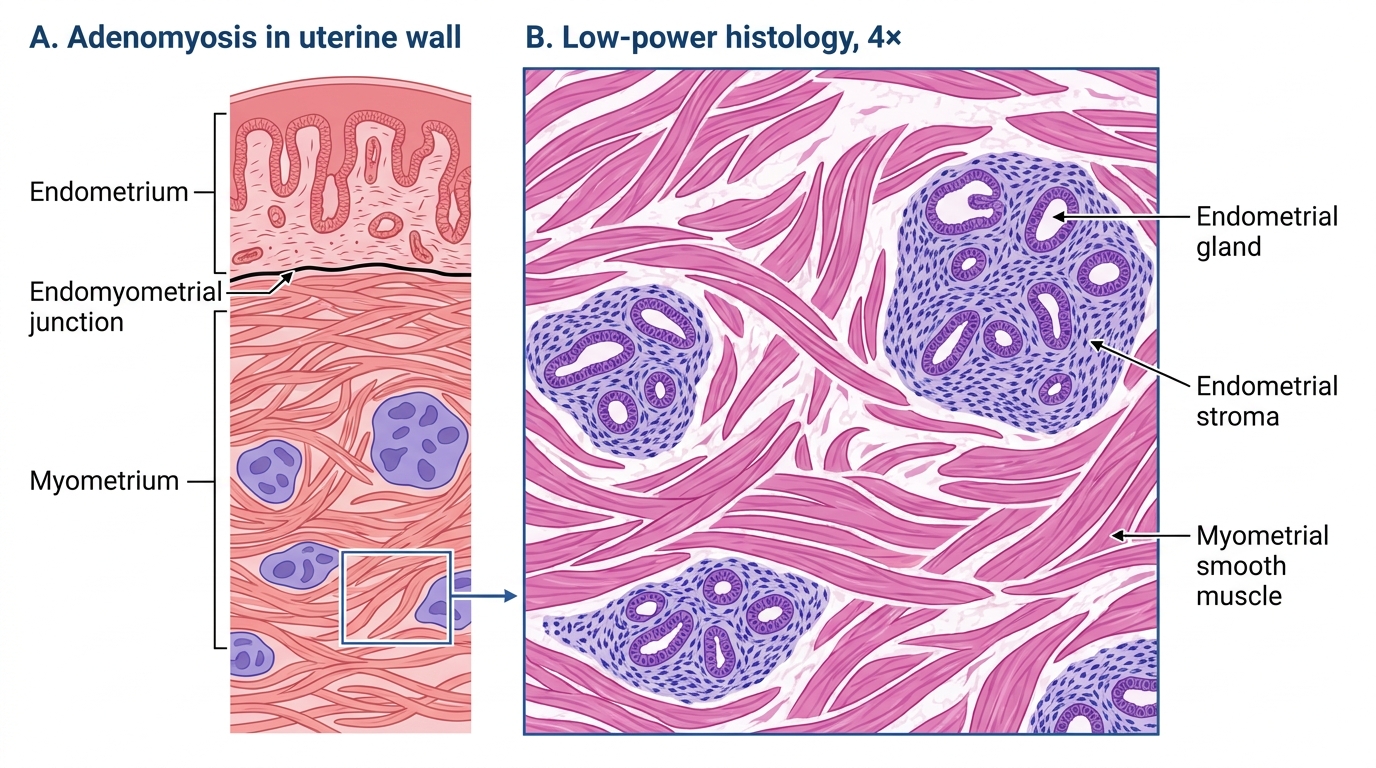
Low-Power Histology of Adenomyosis
Adenomyosis: Clinical Features and Distinction from Endometriosis and Leiomyoma
Clinical features of adenomyosis:
- Abnormal uterine bleeding (AUB) — specifically menorrhagia (heavy menstrual bleeding) ± dysmenorrhea (usually secondary, begins with onset of flow, not pre-menstrually as in endometriosis).
- Diffusely enlarged, tender uterus on bimanual examination — the uterus feels boggy and may be 2× normal size; tenderness is greatest just before and during menstruation.
- No adnexal masses — unlike endometriosis (which produces ovarian endometriomas and tubal adhesions).
- Infertility — less consistently associated than in endometriosis; there is an association with implantation failure in IVF.
- Definitive diagnosis is made histologically — on hysterectomy specimen (the gold standard). Imaging (MRI > ultrasound) can suggest the diagnosis but cannot confirm it.
Comparison table — Adenomyosis vs Endometriosis vs Leiomyoma:
| Feature | Adenomyosis | Endometriosis | Leiomyoma |
|---|---|---|---|
| Location of endometrium | Within myometrium | Outside uterus | Absent |
| Uterine size | Diffusely enlarged | Normal or mildly enlarged | Irregular enlargement |
| Cut surface | Trabeculated, hemorrhagic foci, no capsule | N/A | Whorled, firm, pseudocapsule |
| Key symptom | Menorrhagia + dysmenorrhea | Dysmenorrhea + infertility | Menorrhagia ± pressure symptoms |
| Age group | Perimenopausal multiparous | Reproductive age nulliparous | Reproductive age |
| Infertility | Mild/moderate | Major cause | Minor (if submucosal) |
| Malignant potential | Very rare | ~1% (ovarian) | Very rare (leiomyosarcoma, separate entity) |
| Hormone response | Estrogen-responsive | Strongly estrogen-responsive | Estrogen-responsive |
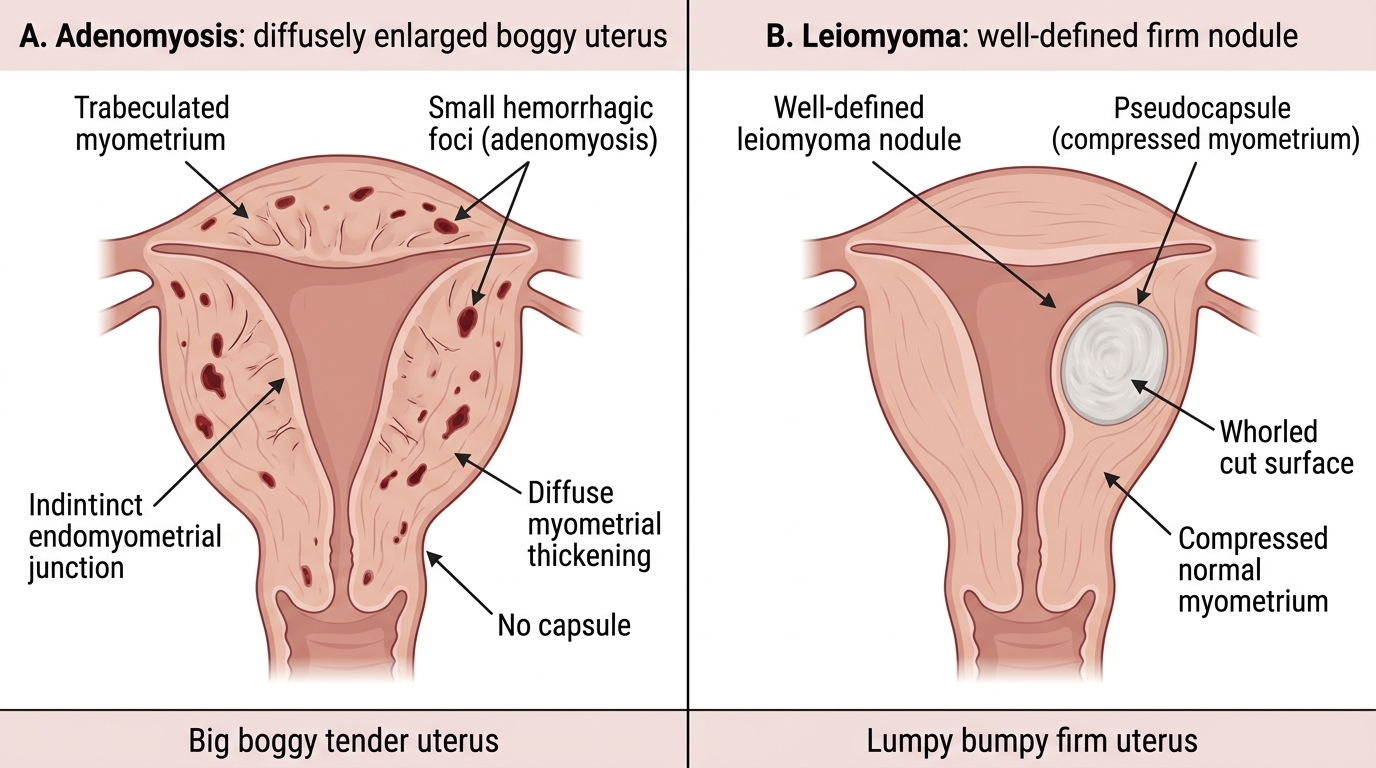
Adenomyosis vs Leiomyoma: Gross Cut Surface
CLINICAL PEARL
Pearl: 'Big boggy tender uterus = adenomyosis; lumpy bumpy firm uterus = leiomyoma.'
In clinical practice, these two conditions are the commonest causes of a symmetrically or asymmetrically enlarged uterus in a perimenopausal woman presenting with heavy menstrual bleeding. The key differentiating examination finding is texture and tenderness: adenomyosis gives a uniformly enlarged, soft/boggy, tender uterus — most tender premenstrually. Leiomyoma gives an irregular, firm, non-tender uterus with discrete nodules. Pelvic MRI is the investigation of choice to differentiate them pre-operatively when the clinical picture is ambiguous. Remember: adenomyosis has no capsule on histology; leiomyoma does.
SELF-CHECK
A 42-year-old multiparous woman (P4L4) presents with 3 years of progressively heavy and painful periods. Examination shows a diffusely enlarged, boggy, tender uterus of 12-week size with no discrete nodules. MRI shows diffuse junctional zone thickening (>12 mm) with small myometrial cysts. She undergoes hysterectomy. Which histological finding is MOST diagnostic of the underlying condition?
A. Whorled bundles of smooth muscle cells arranged in interlacing fascicles, with a fibrous pseudocapsule
B. Endometrial glands and stroma embedded >2.5 mm within the myometrium, surrounded by hypertrophic smooth muscle
C. Endometrial glands with atypia and stromal invasion through the endomyometrial junction
D. Peritoneal implants of endometrial glands and stroma with hemosiderin-laden macrophages
Reveal Answer
Answer: B. Endometrial glands and stroma embedded >2.5 mm within the myometrium, surrounded by hypertrophic smooth muscle
Option B describes adenomyosis: the defining histological criterion is endometrial glands and stroma within the myometrium at a depth >2.5 mm below the endomyometrial junction. The surrounding smooth muscle hypertrophy is a characteristic reactive change. Option A describes leiomyoma. Option C would suggest endometrial carcinoma. Option D describes peritoneal endometriosis (external) — adenomyosis is by definition intramural (internal).
SELF-CHECK
A pathology slide shows a cervical biopsy with prominent lymphoid follicles with germinal centres in the subepithelial stroma, with overlying intact but mildly disrupted squamous epithelium. This pattern of cervicitis is MOST commonly associated with which organism?
A. Neisseria gonorrhoeae
B. Herpes simplex virus type 2
C. Chlamydia trachomatis
D. Trichomonas vaginalis
Reveal Answer
Answer: C. Chlamydia trachomatis
Follicular cervicitis — defined by reactive lymphoid follicles with germinal centres in the cervical stroma — is the histological hallmark of Chlamydia trachomatis cervicitis. Gonorrhoea causes a predominantly neutrophilic/purulent exudate. HSV produces vesicles, ulceration, and Tzanck-positive multinucleated giant cells. Trichomonas is a protozoan that produces a strawberry cervix but not lymphoid follicles.