Page 5 of 23
PA29.{2-3,9} | Endometrial Hyperplasia, Carcinoma & Uterine Smooth Muscle Tumors — SDL Guide
Learning Objectives
- Describe the etiology and hormonal dependence of endometrial hyperplasia and classify it as non-atypical versus atypical/EIN, with associated progression risk.
- Explain the pathogenesis and molecular alterations of Type I endometrioid and Type II serous endometrial carcinoma, and contrast their risk profiles and prognosis.
- Describe the clinical presentation, FIGO staging, routes of spread, and diagnostic approach for endometrial carcinoma.
- Outline the gross and microscopic features of uterine leiomyoma, its hormonal dependence, and key clinical consequences.
- Distinguish leiomyosarcoma from leiomyoma using the Stanford histological criteria, and describe its clinical behaviour.
INSTRUCTIONS
Uterine corpus disease is one of the commonest causes of abnormal uterine bleeding in women across the reproductive and postmenopausal spectrum. Endometrial carcinoma is the most frequent gynaecological malignancy in high-income countries, and leiomyomas affect up to 70% of women by the age of 50. As a Year-2 student, understanding the hormonal and molecular underpinnings of these entities will directly inform your clinical reasoning in any posting where a woman presents with vaginal bleeding or a pelvic mass — Obstetrics, Surgery, and Medicine alike. This SDL walks you from the hyperplastic continuum through to frank malignancy, and from the benign intramural nodule to its malignant counterpart.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 22 — Female Genital Tract (textbook)
- Harsh Mohan — Textbook of Pathology, 8th ed., Ch. 24 — Female Reproductive System (textbook)
- WHO Classification of Tumours of Female Reproductive Organs, 5th ed. (2020) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old woman visits her general practitioner with a three-week history of painless vaginal bleeding. She had her last period twelve years ago. She has hypertension, type 2 diabetes, and a BMI of 34. Her uterus is slightly enlarged on pelvic examination.
She says: "Doctor, surely it's just hormones — I've heard bleeding can come back after menopause sometimes?"
She is wrong. Any vaginal bleeding occurring more than one year after the last menstrual period is postmenopausal bleeding and must be investigated as endometrial carcinoma until histology proves otherwise. Transvaginal ultrasound shows an endometrial thickness of 9 mm. The gynaecologist recommends endometrial sampling.
By the end of this session you will know exactly why her risk profile made this outcome predictable — and how the pathology at the cellular level connects to every symptom and sign you have just read.
WHY THIS MATTERS
Why this matters for your clinical career:
- Endometrial carcinoma is the most common gynaecological malignancy in developed countries and is rising in India with changing dietary and metabolic patterns.
- Leiomyomas affect up to 70% of women by age 50 and are the leading indication for hysterectomy worldwide.
- The hormonal axis linking obesity, insulin resistance, and unopposed estrogen ties together topics from Physiology, Biochemistry, and Pharmacology — making this a favourite integrated question in university examinations.
- FIGO staging of endometrial carcinoma is a standard long-answer question in final MBBS and post-graduate entrance examinations.
- Distinguishing leiomyoma from leiomyosarcoma on histology is a high-yield practical exercise in surgical pathology postings.
RECALL
Before you proceed, anchor the following from Phase-1 and Physiology:
- The menstrual cycle has two phases: The proliferative (follicular) phase, driven by estrogen, causes endometrial gland proliferation and stromal thickening. The secretory (luteal) phase, driven by progesterone, induces glandular secretion and stromal decidualization.
- Progesterone is the physiological anti-estrogen for the endometrium — it down-regulates estrogen receptors and triggers glandular maturation. Absence of progesterone leaves estrogen's proliferative effect unopposed.
- PTEN is a tumour suppressor phosphatase that antagonises the PI3K/AKT proliferation pathway. Loss of PTEN → unchecked cell proliferation.
- TP53 encodes a guardian protein that arrests the cell cycle at G1 on DNA damage. Loss of TP53 → accumulation of mutations.
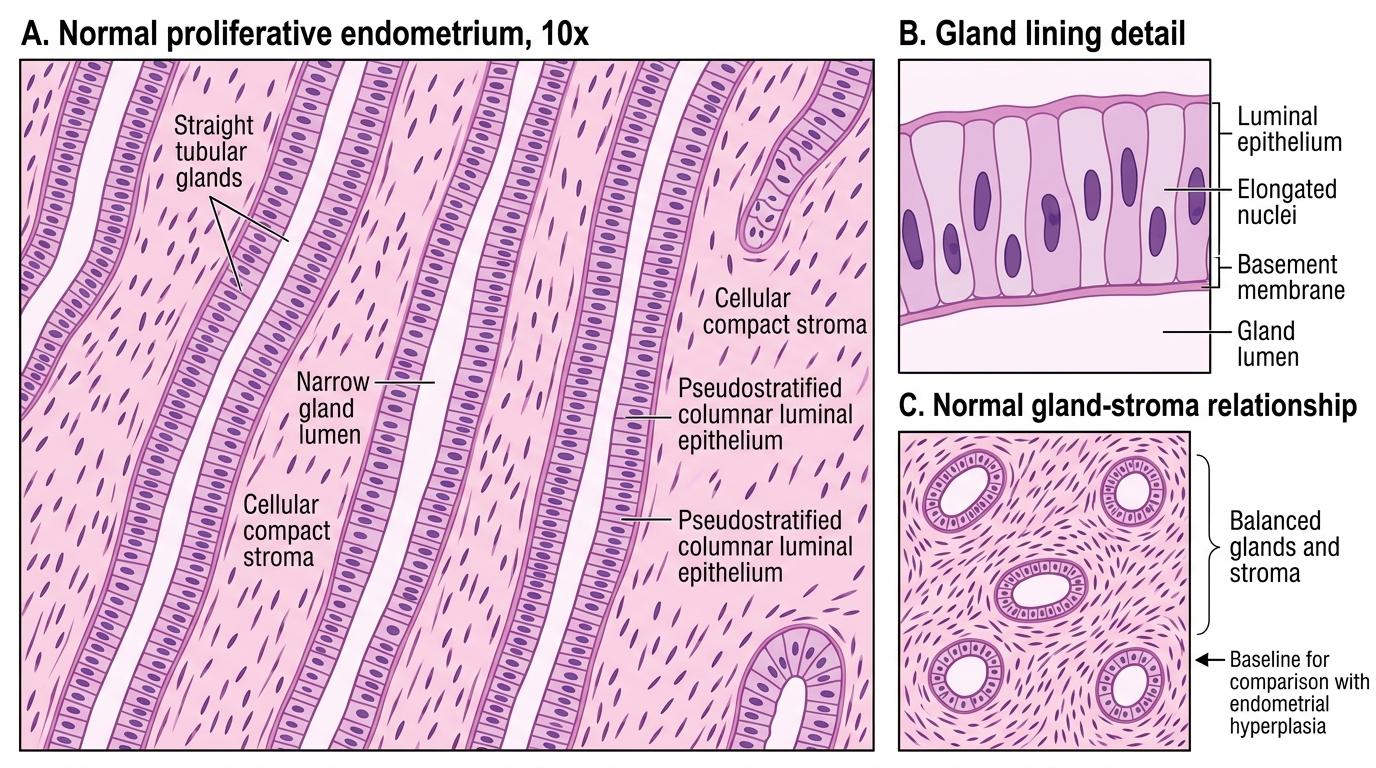
Normal Proliferative Endometrium at 10x
Hold these in mind — every entity in this SDL is a perturbation of one or more of these baseline facts.
Endometrial Hyperplasia — Hormonal Dependence and Etiology
Endometrial hyperplasia is an abnormal proliferation of endometrial glands relative to stroma, driven by unopposed estrogen (estrogen without balancing progesterone).
Mechanism of unopposed estrogen:
Estrogen continuously stimulates gland proliferation. In the absence of progesterone, glands keep dividing. Over months to years this produces increasingly crowded architecture with accumulating genetic errors.
Common causes of unopposed estrogen (etiology):
| Source | Mechanism |
|---|---|
| Anovulatory cycles (PCOS, perimenopause) | No corpus luteum → no progesterone |
| Obesity | Peripheral aromatization of androgens → estrone in adipose tissue |
| Exogenous estrogen (ERT without progestogen) | Pharmacological unopposed estrogen |
| Tamoxifen (for breast cancer) | Partial estrogen agonist at endometrium |
| Granulosa cell tumour of ovary | Autonomously secretes estrogen |
| Polycystic ovary syndrome (PCOS) | Chronic anovulation → persistent estrogen |
Note: Insulin resistance (diabetes, metabolic syndrome) amplifies hyperplasia risk by reducing sex-hormone-binding globulin, increasing free estrogen, and directly stimulating endometrial insulin-like growth factor receptors — which is why diabetic-obese women like the patient in the hook have compounded risk.
Non-atypical Endometrial Hyperplasia
Classification of Endometrial Hyperplasia: Non-Atypical vs Atypical/EIN
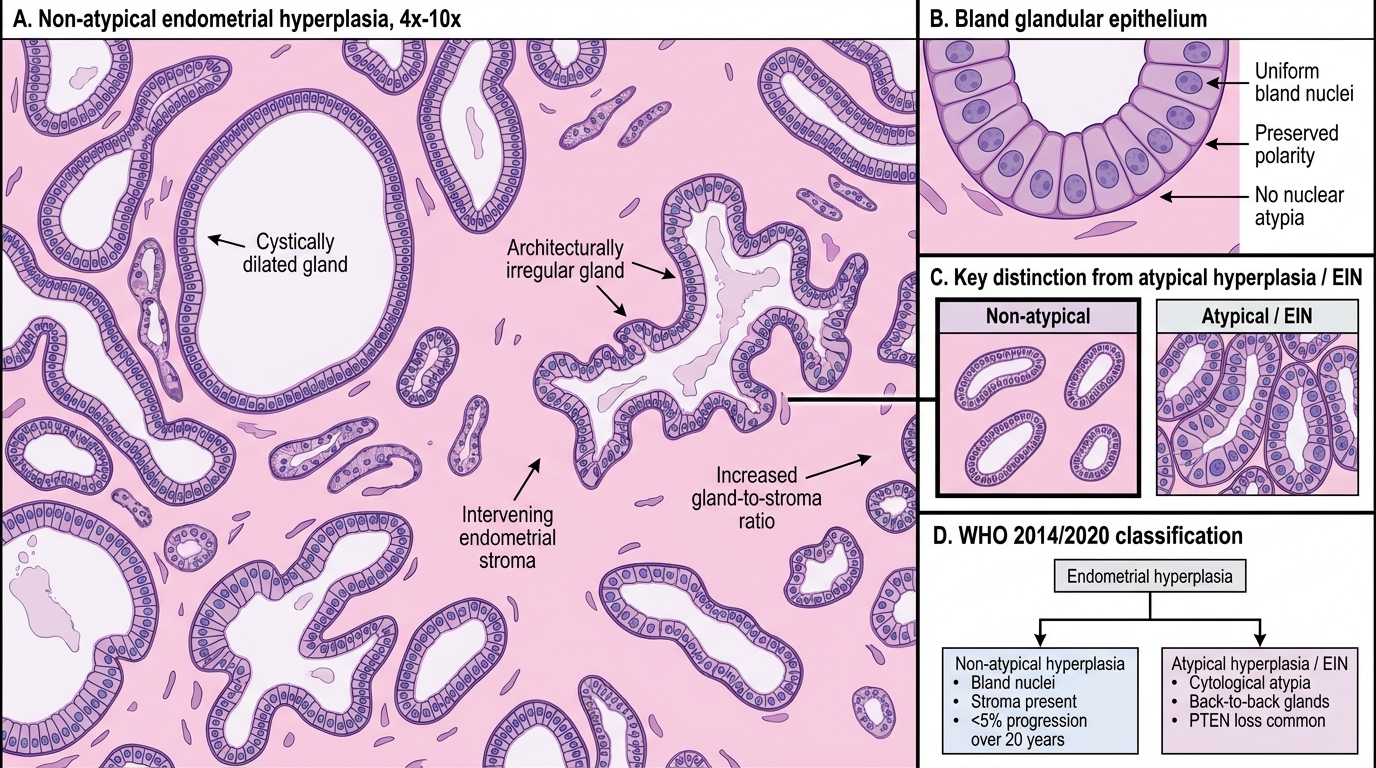
The WHO 2014/2020 classification uses a two-tier system replacing the older four-tier scheme (simple/complex with and without atypia):
1. Non-atypical hyperplasia (formerly simple or complex hyperplasia without atypia)
• Glands are increased in number and may be architecturally irregular or cystically dilated.
• Epithelial nuclei are bland — round to oval, uniform, without nucleoli.
• Stroma is present between glands.
• Progression to carcinoma: < 5% over 20 years.
• Management: progestogen therapy (medroxyprogesterone acetate), address underlying cause.
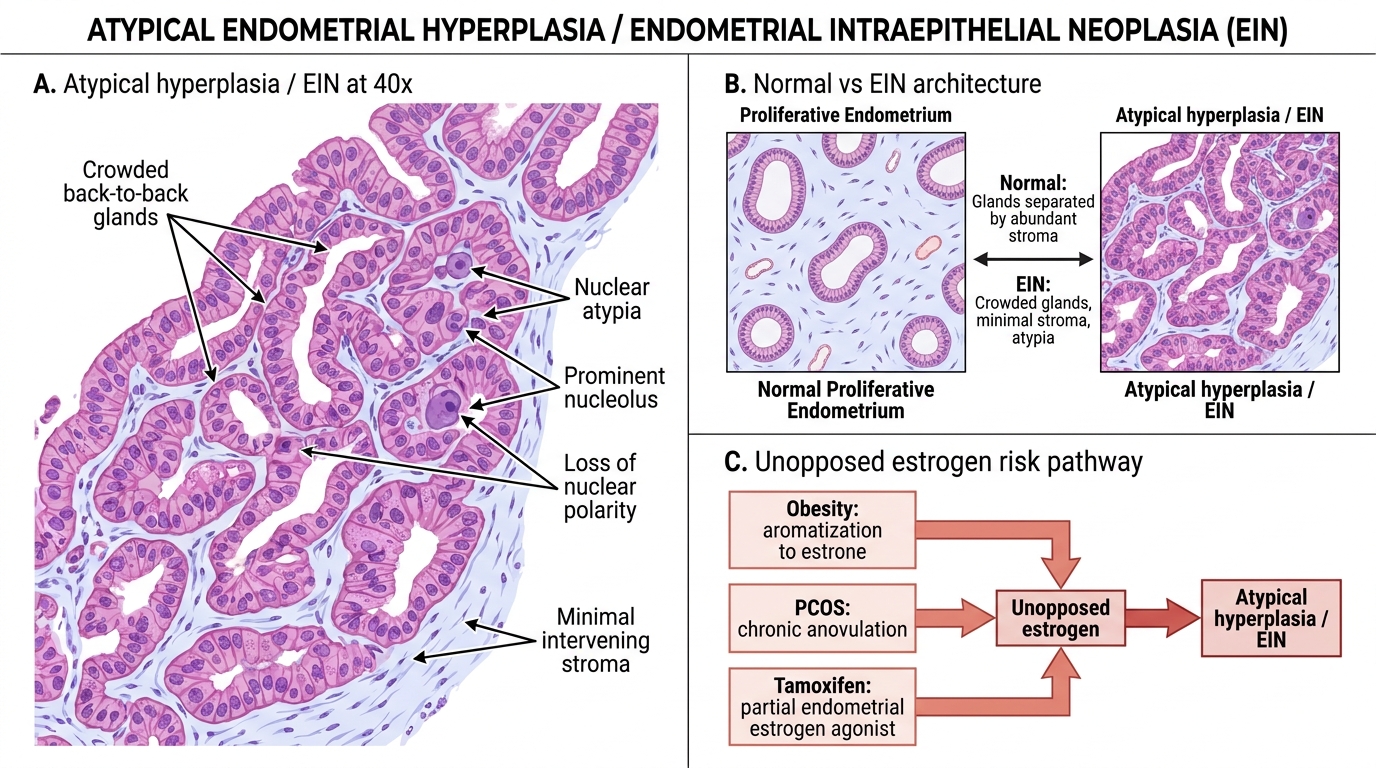
2. Atypical hyperplasia / Endometrial Intraepithelial Neoplasia (EIN)
• The WHO 2020 edition equates atypical hyperplasia (clinical gynecology terminology) with EIN (endometrial intraepithelial neoplasia — molecular pathology terminology).
• Key feature: cytological atypia — enlarged, rounded vesicular nuclei with prominent nucleoli, loss of polarity.
• Architecture: glands are crowded or back-to-back with minimal intervening stroma (the gland area exceeds the stroma area).
• PTEN loss is the earliest and most consistent molecular event: found in > 80% of EIN lesions. Loss of PTEN → hyperactivated PI3K/AKT → unchecked gland proliferation.
• Microsatellite instability (MSI) and KRAS mutations also occur.
• Progression to endometrioid carcinoma: 25–40% risk. Up to 40% of women diagnosed with atypical hyperplasia on curettage have concurrent carcinoma in the hysterectomy specimen.
• Management: hysterectomy (preferred) or high-dose progestogen for women wishing to preserve fertility.
Atypical Endometrial Hyperplasia / EIN
CLINICAL PEARL
The obesity–PCOS–tamoxifen triad of unopposed estrogen:
- A woman with PCOS has chronic anovulation → persistent estrogen without progesterone surges. Even young (20–30-year-old) PCOS patients can develop atypical hyperplasia and should have periodic endometrial surveillance.
- Obesity is independently the single strongest modifiable risk factor. Fat tissue aromatises androstenedione to estrone. A woman with BMI > 30 has 2–3× the endometrial carcinoma risk of a normal-weight woman; BMI > 40 confers a 6× risk.
- Tamoxifen used for breast cancer prevention or treatment acts as a partial estrogen agonist at the endometrium (while being an antagonist at the breast). Patients on tamoxifen require annual endometrial surveillance and should promptly report any vaginal bleeding.
Endometrial Carcinoma — Type I Endometrioid (Estrogen-Driven)
Type I endometrial carcinoma is the endometrioid subtype and accounts for ~80% of all endometrial carcinomas.
Risk factors: Obesity, anovulation, PCOS, late menopause, nulliparity, diabetes, exogenous estrogen, tamoxifen, Lynch syndrome (hereditary mismatch repair deficiency → MSI).
Molecular pathogenesis:
| Alteration | Frequency | Significance |
|---|---|---|
| PTEN loss | 80% | Earliest change, shared with EIN precursor |
| Microsatellite instability (MSI) | 20–30% | Lynch syndrome cases; hypermutation |
| KRAS mutation | 15–30% | RAS/MAPK proliferation pathway |
| CTNNB1 (β-catenin) mutation | 15–20% | Wnt pathway; squamous metaplasia |
| PIK3CA mutation | 35% | Downstream of PTEN in PI3K pathway |
Gross appearance: Exophytic, polypoid, friable tan-grey mass arising from the endometrium, often in the fundus or posterior wall. The depth of myometrial invasion is critical for staging.
Histology: Back-to-back malignant glands with confluent cribriform architecture, loss of intervening stroma, and glands lined by atypical columnar cells with prominent nucleoli. Squamous differentiation (morules) is common.
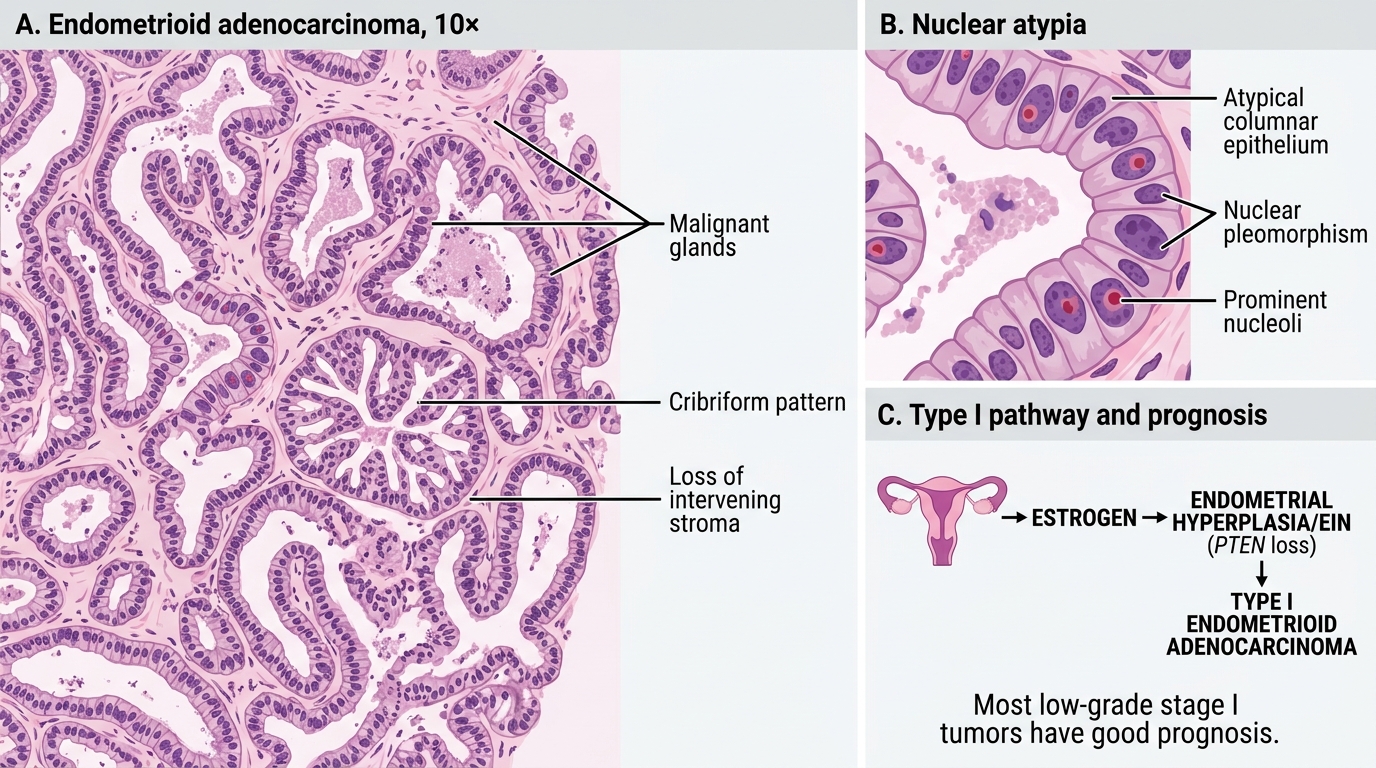
Endometrioid Adenocarcinoma at 10×
Prognosis: Generally good — most present at stage I (confined to uterine corpus) and have > 85% five-year survival when low-grade.
SELF-CHECK
A 52-year-old obese woman with PCOS undergoes endometrial biopsy for irregular bleeding. Histology shows crowded back-to-back glands with nuclear atypia and prominent nucleoli. Molecular analysis reveals PTEN loss. What is the MOST appropriate diagnosis?
A. Non-atypical endometrial hyperplasia
B. Atypical hyperplasia / Endometrial Intraepithelial Neoplasia (EIN)
C. Type II serous endometrial carcinoma
D. Endometrial polyp with reactive atypia
Reveal Answer
Answer: B. Atypical hyperplasia / Endometrial Intraepithelial Neoplasia (EIN)
The combination of crowded back-to-back glands, nuclear atypia with prominent nucleoli, and PTEN loss is diagnostic of atypical hyperplasia / EIN — the direct precursor to Type I endometrioid carcinoma. Non-atypical hyperplasia lacks cytological atypia. Type II serous carcinoma is TP53-driven and not associated with PTEN or the estrogen-hyperplasia pathway. An endometrial polyp lacks these architectural and molecular features.