Page 6 of 23
PA29.{2-3,9} | Endometrial Hyperplasia, Carcinoma & Uterine Smooth Muscle Tumors — SDL Guide (Part 2)
Endometrial Carcinoma — Type II Serous (Non-Estrogen-Driven)
Type II endometrial carcinoma — predominantly the serous (papillary serous) subtype — accounts for only ~10% of endometrial carcinomas but causes a disproportionate share of deaths because of its aggressive biology.
Contrast with Type I:
| Feature | Type I Endometrioid | Type II Serous |
|---|---|---|
| Age at presentation | Perimenopausal (55–65 yr) | Older postmenopausal (65–75 yr) |
| Estrogen dependence | Yes | No |
| Precursor lesion | Atypical hyperplasia / EIN | Serous Endometrial Intraepithelial Carcinoma (SEIC) |
| Key mutation | PTEN, MSI, KRAS | TP53 (> 90%) |
| Grade | Low (Grade 1–2) | High (Grade 3 by default) |
| Background endometrium | Hyperplastic / thick | Atrophic |
| Prognosis | Good | Poor |
TP53 mutation is the driver event in serous carcinoma, arising in an atrophic endometrium through SEIC (non-invasive serous carcinoma in surface epithelium or glands).
Histology: Complex papillary architecture with fibrovascular cores, lined by cells with marked nuclear pleomorphism, hyperchromatic nuclei, prominent nucleoli, and numerous atypical mitoses. Characteristically, cells with bulging apical cytoplasm appear to be falling into gland lumens ("hobnail" cells in some variants).
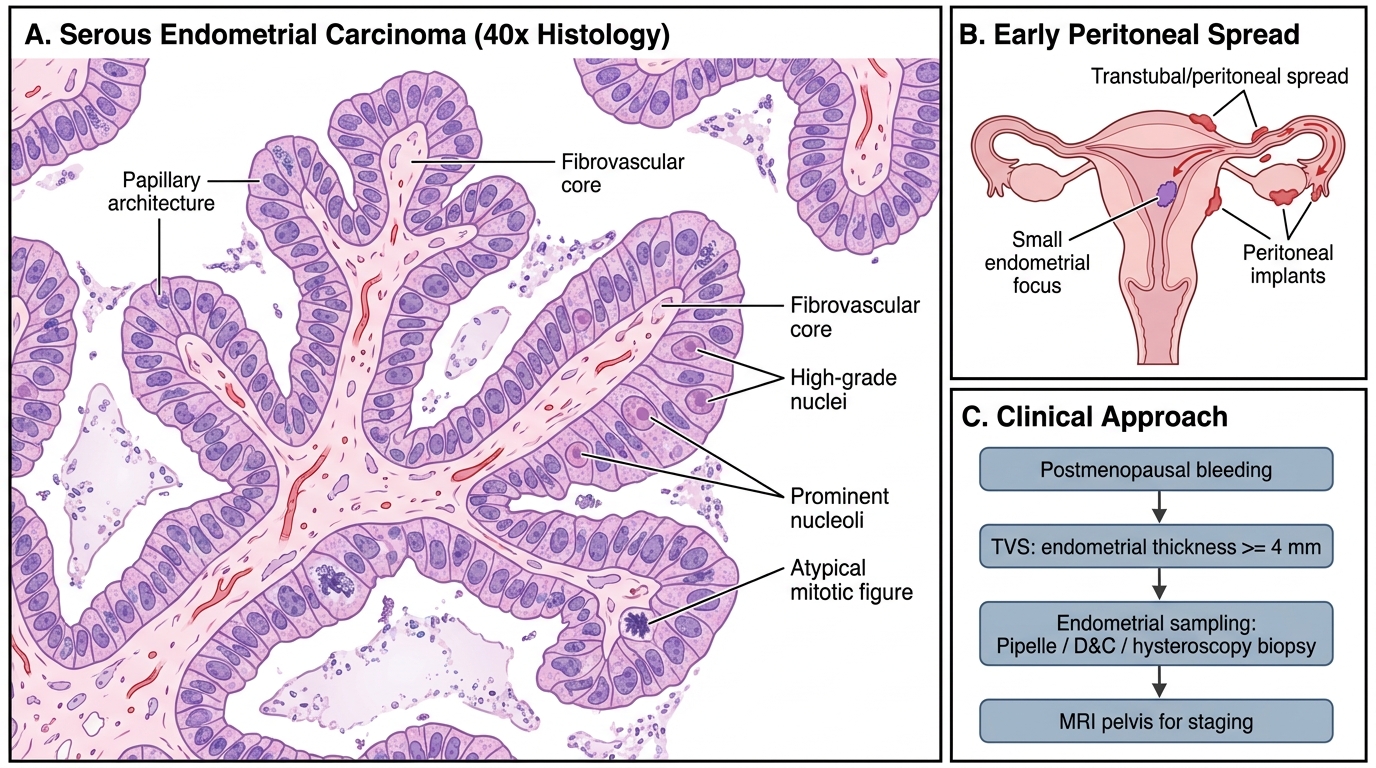
Serous Endometrial Carcinoma: High-Power Histology and Clinical Significance
Why serous kills: Despite arising in small foci (even SEIC), serous carcinoma spreads early to peritoneal surfaces (analogous to ovarian serous carcinoma) — stage for stage, it carries a far worse prognosis than endometrioid.
Endometrial Carcinoma — Presentation, Diagnosis, and Clinical Approach
Clinical presentation:
- Postmenopausal bleeding (PMB) — the cardinal symptom. Occurs in 90% of symptomatic cases. Any PMB (bleeding > 12 months after last period) mandates investigation.
- Premenopausal: abnormal uterine bleeding, menorrhagia, or intermenstrual bleeding — often misattributed to fibroids or dysfunction.
- Pelvic pain is a late feature, suggesting parametrial or nodal involvement.
- Rarely: pyometra (distension of the uterine cavity with pus) in elderly women with cervical stenosis.
Diagnostic pathway:
1. Transvaginal ultrasound (TVS) — endometrial thickness ≥ 4 mm in a postmenopausal woman is abnormal and warrants sampling (sensitivity ~96% for carcinoma).
2. Endometrial sampling:
• Pipelle biopsy (outpatient, 90% sensitivity for carcinoma)
• Dilatation and curettage (D&C) — more complete, used if Pipelle is inadequate
• Hysteroscopy + directed biopsy — best for focal lesions
3. MRI pelvis — most accurate for assessing depth of myometrial invasion and cervical involvement (critical for staging and surgical planning).
4. CT chest/abdomen/pelvis or PET-CT — distant staging, especially for high-grade histology.
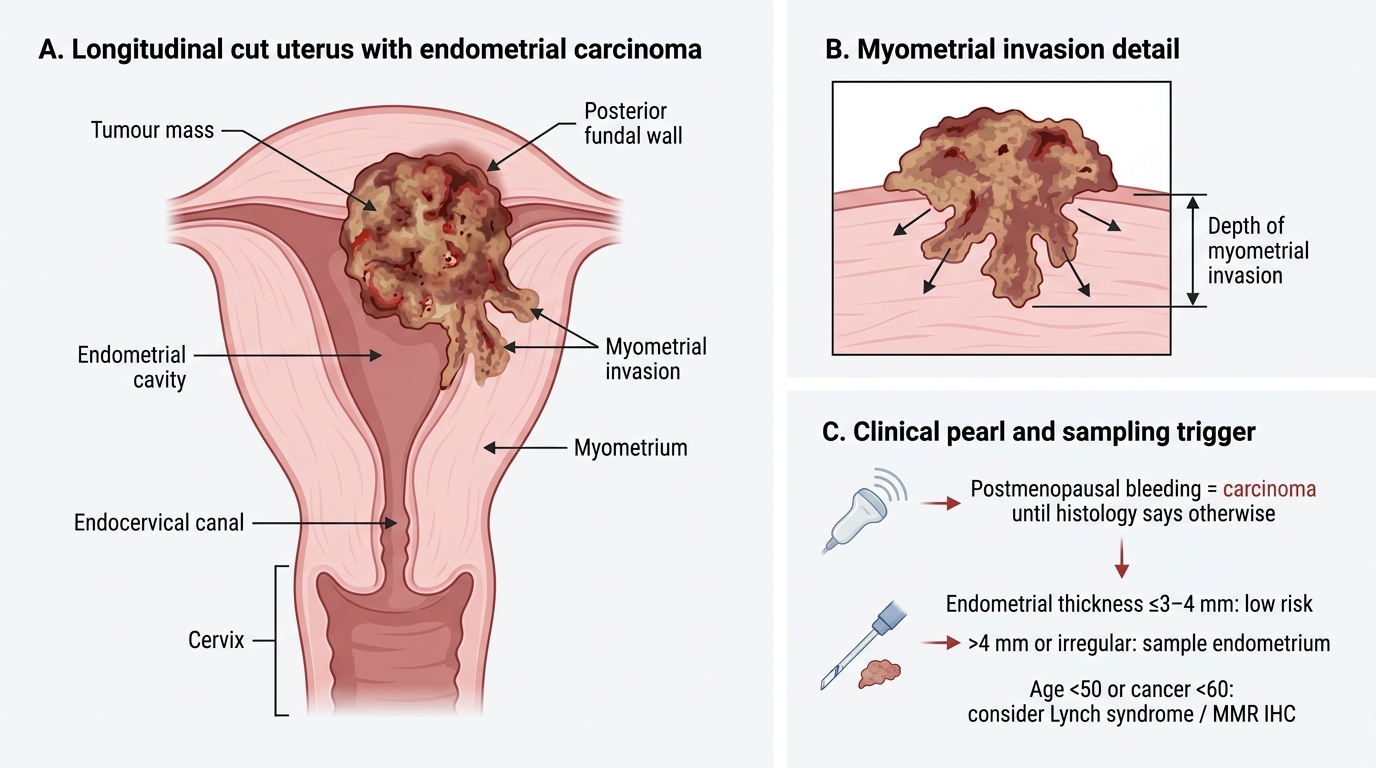
Gross Endometrial Carcinoma With Myometrial Invasion
CLINICAL PEARL
Postmenopausal bleeding = carcinoma until histology says otherwise.
Only 10% of women with PMB have endometrial carcinoma — but 90% of women with endometrial carcinoma present with vaginal bleeding. The asymmetry is everything: you cannot reassure without tissue.
TVS threshold: In a postmenopausal woman NOT on hormone replacement, an endometrial thickness of ≤ 3–4 mm has a negative predictive value of ~99% for carcinoma and may avoid biopsy. Any thickness > 4 mm, irregular echo texture, or inhomogeneity mandates endometrial sampling regardless of symptom severity.
Lynch syndrome alert: In a woman < 50 presenting with endometrial carcinoma, always consider Lynch syndrome (hereditary non-polyposis colorectal cancer — HNPCC). Reflex immunohistochemistry for mismatch repair proteins (MLH1, MSH2, MSH6, PMS2) should be performed on all endometrial carcinoma specimens under 60 — this has direct implications for colorectal cancer screening of the patient and her family.
Grading, FIGO Staging, Myometrial Invasion, and Routes of Spread
Histological grading (FIGO/WHO for endometrioid carcinoma):
| Grade | Architecture | Nuclear Atypia |
|---|---|---|
| Grade 1 | ≤ 5% solid non-squamous growth | Mild |
| Grade 2 | 6–50% solid growth | Moderate |
| Grade 3 | > 50% solid growth | Severe (upgrades G1 → G2 if severe atypia) |
Serous and clear cell carcinomas are Grade 3 by definition.
FIGO Staging (2023 revised):
| Stage | Definition |
|---|---|
| IA | Tumour confined to endometrium or invades < ½ myometrium |
| IB | Invades ≥ ½ myometrium |
| II | Invades cervical stroma (not just surface epithelium) |
| IIIA | Serosa or adnexal involvement |
| IIIB | Vaginal or parametrial involvement |
| IIIC1 | Pelvic lymph node metastasis |
| IIIC2 | Para-aortic lymph node metastasis |
| IVA | Bladder or bowel mucosa invasion |
| IVB | Distant metastasis (lung, liver, bone) |
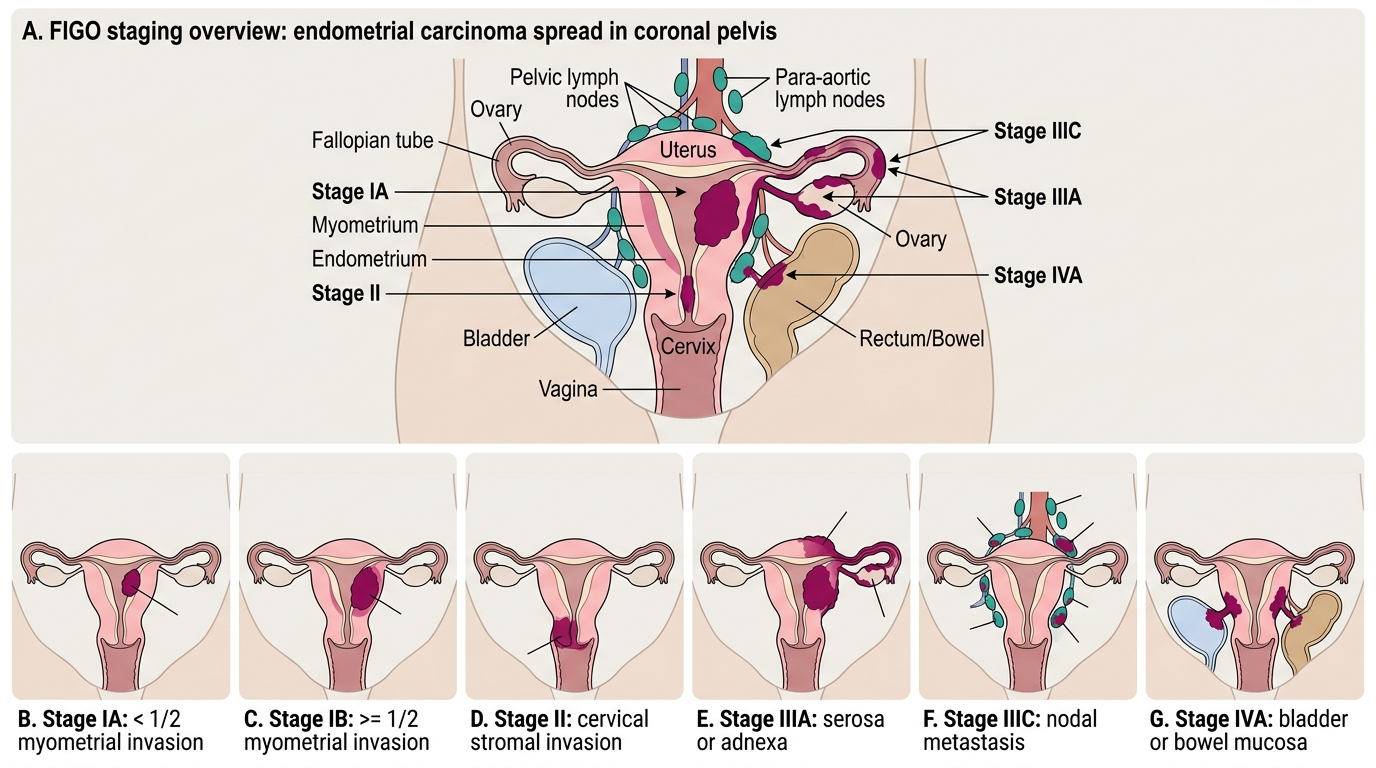
FIGO Staging of Endometrial Carcinoma
Myometrial invasion is the single most important prognostic factor in Stage I disease. Depth correlates directly with lymphovascular invasion, nodal metastasis risk, and recurrence.
Routes of spread:
• Direct extension — to cervix, vagina, parametrium, bladder, rectum
• Lymphatic — to pelvic lymph nodes (obturator, internal iliac, external iliac), then para-aortic nodes (via ovarian lymphatics from the fundus)
• Transtubal (transcoelomic) — especially serous subtype — peritoneal seeding via fallopian tube
• Haematogenous — lungs, liver, bone (late stage)
SELF-CHECK
Histopathology of a hysterectomy specimen shows a Grade 2 endometrioid adenocarcinoma with invasion of exactly half the myometrial thickness. No cervical stromal involvement. No nodal or adnexal disease. What is the FIGO stage?
A. Stage IA
B. Stage IB
C. Stage II
D. Stage IIIA
Reveal Answer
Answer: B. Stage IB
Stage IB is defined as myometrial invasion of ≥ ½ the myometrial thickness with disease still confined to the uterine corpus. Stage IA is < ½ invasion. Stage II requires cervical stromal involvement. Stage IIIA requires serosa or adnexal spread. Since invasion is exactly half (≥ ½), this is Stage IB.