Page 7 of 23
PA29.{2-3,9} | Endometrial Hyperplasia, Carcinoma & Uterine Smooth Muscle Tumors — SDL Guide (Part 3)
Uterine Leiomyoma — The Benign Smooth Muscle Tumour
Uterine leiomyoma (commonly called a fibroid, though it contains no fibrous tissue) is the most common tumour in women — found in up to 70% of women over 50, with higher prevalence in women of African descent.
Hormonal dependence:
Leiomyomas are estrogen-dependent and progesterone-dependent (both hormones promote growth). They:
• Grow during the reproductive years and regress post-menopause.
• Enlarge during pregnancy (high estrogen/progesterone).
• Regress with GnRH agonist therapy (chemical menopause).
• Never arise in prepubertal girls.
Pathogenesis: Monoclonal proliferations arising from a single smooth muscle cell. Common cytogenetic abnormalities include deletions/translocations involving chromosomes 7 and 12, and mutations in MED12 (mediator complex — transcriptional regulation).
Gross features:
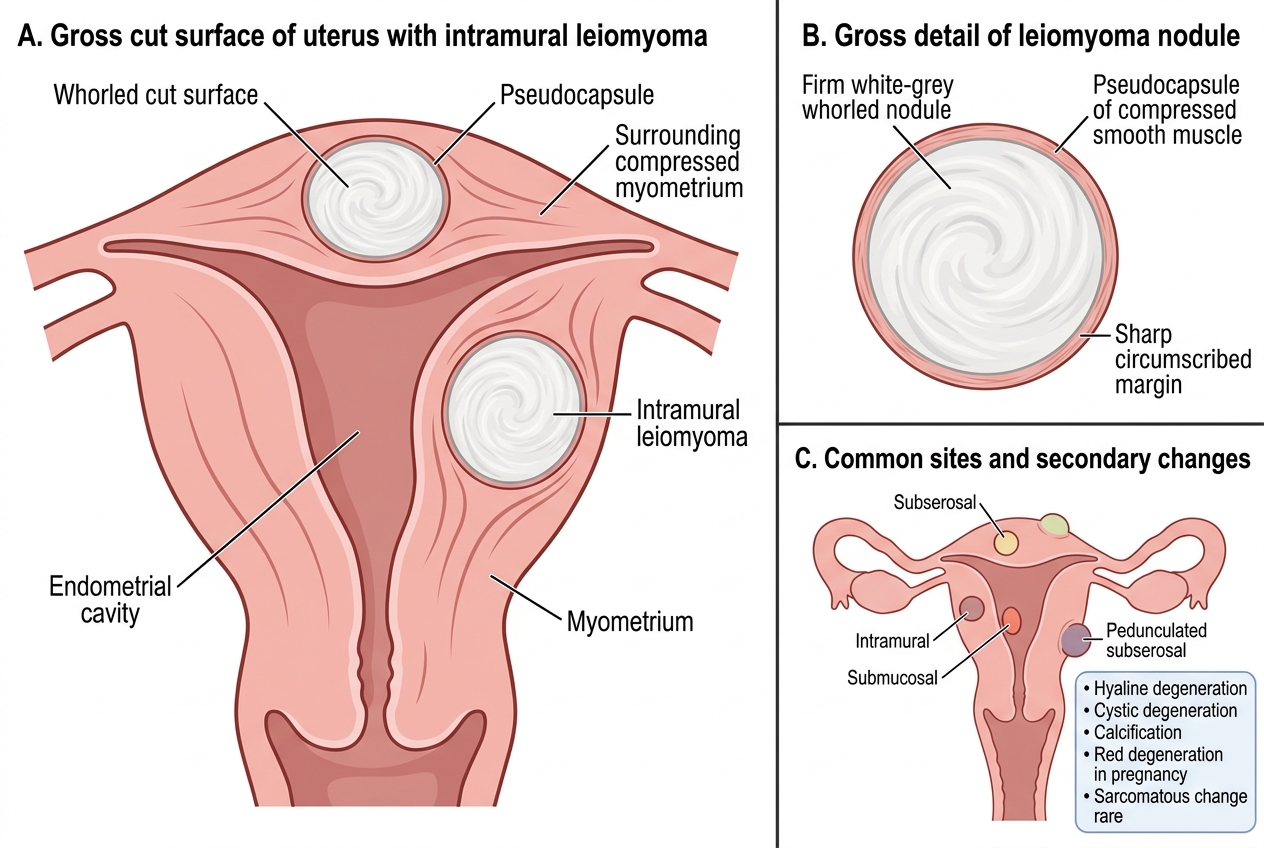
Gross Cut Surface of Intramural Uterine Leiomyoma
- Well-circumscribed, white-grey, whorled cut surface.
- Firm rubbery consistency.
- A pseudo-capsule of compressed smooth muscle surrounds each nodule (facilitates enucleation).
- Often multiple (average 6–7 per uterus).
- Locations: intramural (most common), submucosal (most symptomatic — distorts cavity), subserosal (can be pedunculated), cervical, broad ligament, intraligamentous.
Secondary changes: Hyaline degeneration (most common), cystic degeneration, calcification ("womb stones" on X-ray), red (carneous) degeneration during pregnancy (acute haemorrhagic infarction → severe pain), sarcomatous change (extremely rare, < 0.1%).
Microscopy:
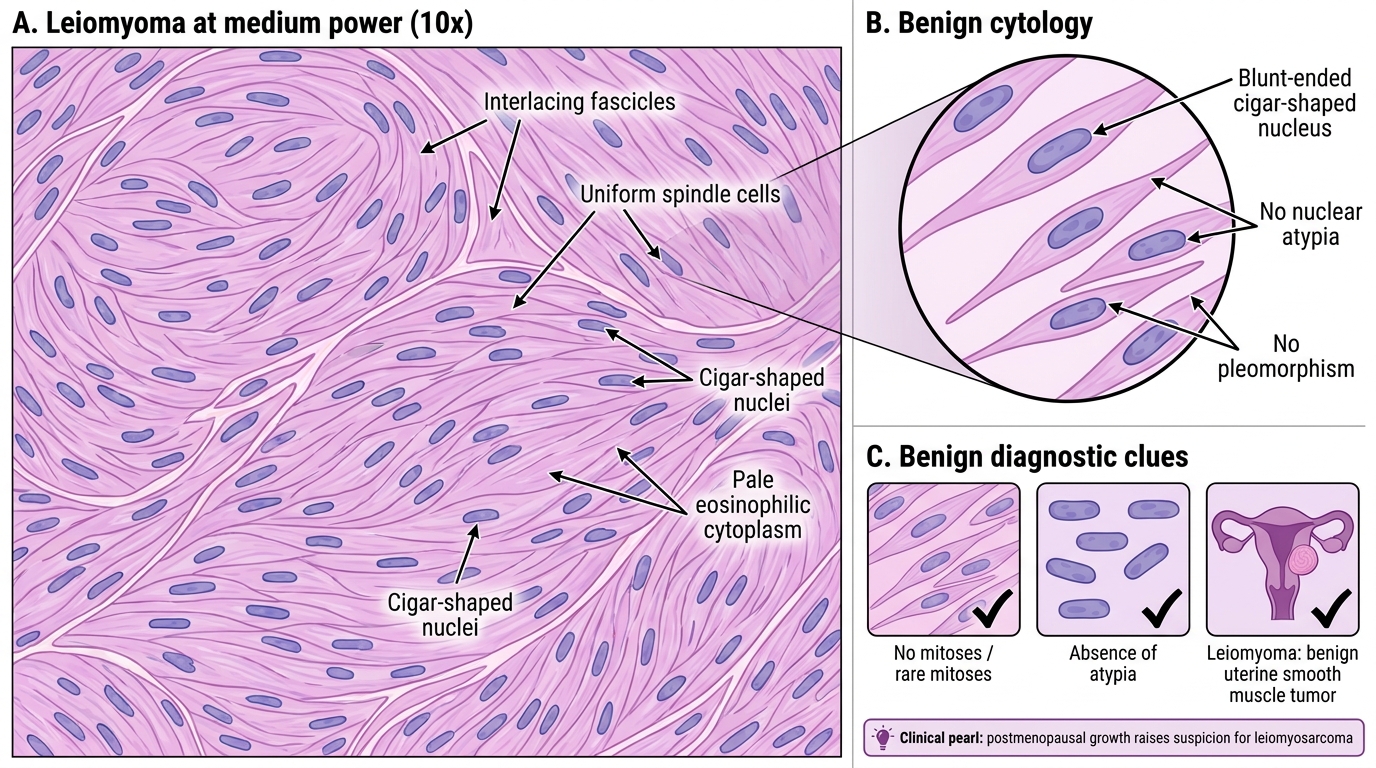
Leiomyoma at Medium Power: Benign Smooth Muscle Fascicles
- Interlacing fascicles of uniform spindle cells.
- Nuclei: cigar-shaped, blunt-ended, uniform, no atypia.
- Cytoplasm: pale eosinophilic, fibrillar.
- Mitoses: rare (< 5 per 10 high-power fields) — absence of significant mitotic activity is a key benign feature.
Clinical features:
• Abnormal uterine bleeding — menorrhagia (heavy periods) most common; submucosal fibroids cause heaviest bleeding (increased surface area, disrupted haemostatic mechanisms).
• Pressure symptoms — urinary frequency (anterior fibroid on bladder), constipation (posterior fibroid on rectum), venous compression.
• Infertility and recurrent miscarriage — submucosal fibroids distort the uterine cavity.
• Uterine enlargement — irregular, non-tender, firm uterus on examination.
CLINICAL PEARL
Leiomyoma regresses after menopause — leiomyosarcoma grows.
This is a critical clinical discriminator:
- A fibroid that enlarges after menopause must raise suspicion for leiomyosarcoma and requires imaging reassessment (MRI) and/or surgical evaluation.
- Sarcomatous transformation of a leiomyoma — while historically cited, is now considered extremely rare (< 0.1% of leiomyomas). Current evidence strongly suggests that leiomyosarcomas arise de novo from uterine smooth muscle, not from pre-existing leiomyomas.
- MRI features suggesting malignancy: indistinct margins, heterogeneous signal, central necrosis, rapid growth on serial imaging.
This de-novo origin is a common exam misconception — do NOT write "leiomyosarcoma arises from malignant transformation of leiomyoma" in a university examination.
Uterine Leiomyosarcoma — The Malignant Smooth Muscle Tumour
Leiomyosarcoma is the most common uterine sarcoma, accounting for 1–2% of uterine malignancies, but responsible for a disproportionate share of uterine cancer deaths.
Origin: Arises de novo from uterine smooth muscle. It does NOT arise from a pre-existing leiomyoma (a common but incorrect belief).
Gross features:
• Usually a solitary, large (often > 10 cm), fleshy, poorly circumscribed mass.
• Cut surface: variegated, haemorrhagic, necrotic — in stark contrast to the whorled white benign fibroid.
• Infiltrates surrounding myometrium without a true pseudocapsule.
Histological diagnosis — the Stanford criteria (all three required for definitive diagnosis):
| Criterion | Threshold |
|---|---|
| Cytological atypia | Moderate to severe nuclear atypia |
| Mitotic index | ≥ 10 mitoses per 10 HPF |
| Tumor cell necrosis | Geographic (coagulative) necrosis |
Presence of 2 of 3 criteria supports the diagnosis in conjunction with clinical context. Cases not meeting full criteria are classified as smooth muscle tumors of uncertain malignant potential (STUMP).
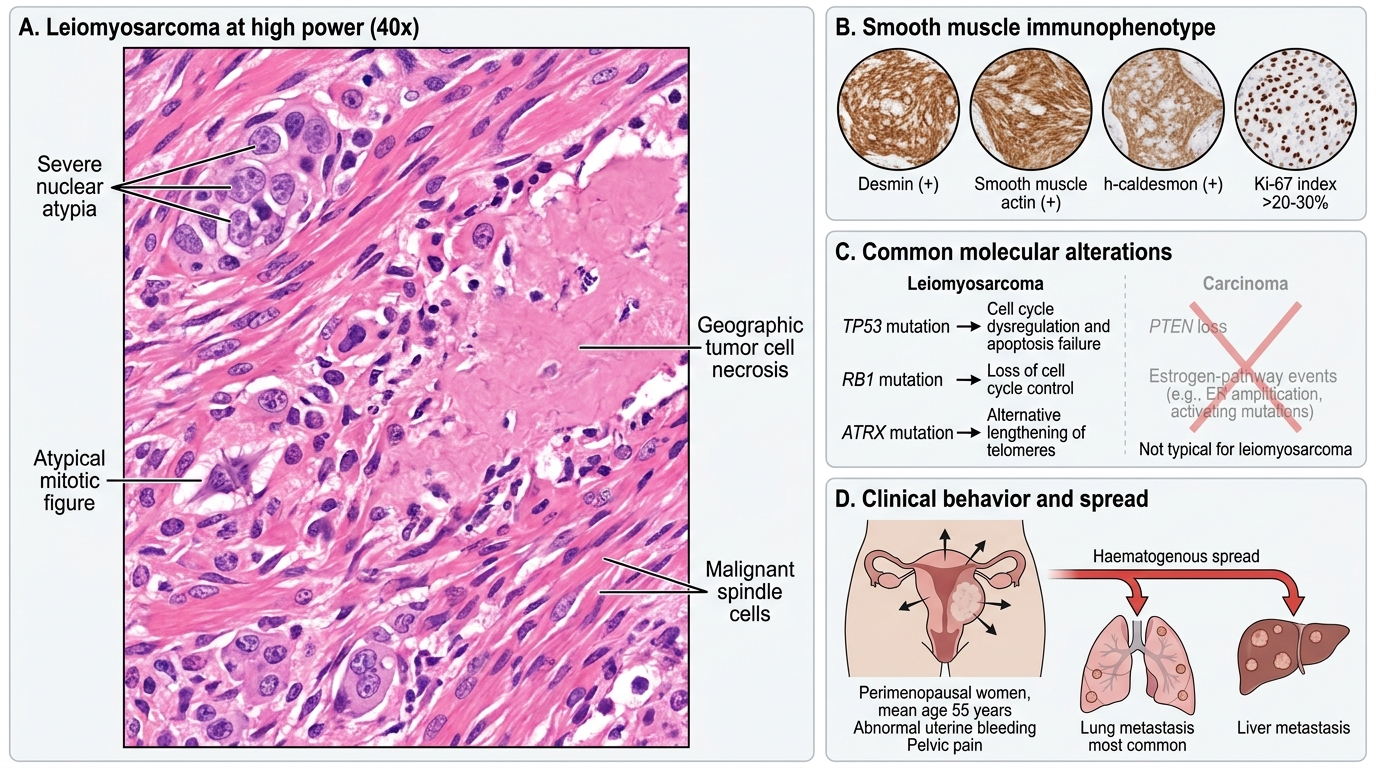
Leiomyosarcoma: High-Power Histology and Clinical Correlates
Immunohistochemistry: Positive for smooth muscle markers — desmin, smooth muscle actin (SMA), h-caldesmon. Ki-67 proliferation index is markedly elevated (> 20–30%).
Molecular alterations: Unlike carcinoma, leiomyosarcoma does not show PTEN loss or estrogen-pathway molecular events. Common alterations include TP53, RB1, and ATRX mutations.
Clinical behaviour:
• Typically presents in perimenopausal women (mean age 55 years).
• Symptoms: abnormal uterine bleeding, rapidly enlarging pelvic mass, pelvic pain.
• Spread: predominantly haematogenous — lung is the most common metastatic site, then liver. Lymph node metastasis is less frequent than in carcinoma.
• Five-year survival: ~50% for Stage I, dropping to < 15% for Stage III/IV — far worse than endometrioid carcinoma.
Leiomyoma vs Leiomyosarcoma — comparison table:
| Feature | Leiomyoma | Leiomyosarcoma |
|---|---|---|
| Frequency | Very common | Rare |
| Multiplicity | Usually multiple | Usually solitary |
| Post-menopausal behaviour | Regresses | Grows |
| Gross | Whorled, white, circumscribed | Fleshy, necrotic, infiltrative |
| Mitoses | < 5/10 HPF | ≥ 10/10 HPF |
| Nuclear atypia | Absent | Severe |
| Tumor cell necrosis | Absent | Present |
| Origin | Monoclonal SM cell | De novo from SM |
| Prognosis | Excellent (benign) | Poor |
SELF-CHECK
Histology of a uterine mass shows spindle cells with severe nuclear atypia, 12 mitoses per 10 HPF, and areas of geographic tumor cell necrosis. Immunostaining is positive for desmin and smooth muscle actin. What is the MOST likely diagnosis?
A. Cellular leiomyoma
B. Smooth muscle tumour of uncertain malignant potential (STUMP)
C. Leiomyosarcoma
D. Endometrial stromal sarcoma
Reveal Answer
Answer: C. Leiomyosarcoma
All three Stanford criteria for leiomyosarcoma are met: severe cytological atypia, ≥ 10 mitoses per 10 HPF, and geographic tumor cell necrosis. Positive desmin and SMA confirm smooth muscle differentiation. Cellular leiomyoma has increased cellularity but no atypia or significant mitoses. STUMP is diagnosed when criteria are incompletely met. Endometrial stromal sarcoma arises from endometrial stroma, not smooth muscle, and would show CD10 positivity.