Page 14 of 23
PA29.{5,10} | Gestational Trophoblastic Disease & Female Genital Morphology — SDL Guide
Learning Objectives
- Describe the etiology, pathogenesis, and karyotypic basis of complete and partial hydatidiform moles, distinguishing their villous morphology and malignant potential
- Explain the pathology and clinical course of invasive mole, choriocarcinoma, and placental site trophoblastic tumor, including modes of spread and complications
- Identify the gross and microscopic features of key female genital tract lesions — cervicitis, endometriosis, endometrial hyperplasia, endometrial carcinoma, leiomyoma, leiomyosarcoma — in a practical context
- Recognise the major categories of ovarian tumors (epithelial, germ cell, sex-cord stromal, metastatic) by their characteristic gross and microscopic appearances
- Apply pattern-recognition strategies to discriminate between morphologically similar entities in the examination practical
INSTRUCTIONS
This is the morphology-consolidation SDL for the Female Genital Tract cluster. Before reading, pull out your atlas or practical manual. Every content block is paired with a specimen-level image description — mentally match what you read to images you have seen in your practical sessions. Gestational trophoblastic disease is covered in full for PA29.5, and the second half systematically walks through the gross-and-micro signature of every major lesion you are expected to identify at the bench. Expect 35 minutes of active reading plus atlas cross-referencing.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 22 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old woman presents with hyperemesis, a uterus larger than expected for dates, and an hCG of 480,000 mIU/mL. Ultrasound shows a 'snowstorm' pattern with no fetal heartbeat. The suction curettage specimen is sent to pathology: the pot is filled with translucent grape-like vesicles.
The pathologist's next question is not 'Is this a mole?' — the answer is obvious. The real question is: 'Is this a complete or partial mole, and does the trophoblast look sufficiently atypical to warrant closer follow-up?' That distinction — rooted entirely in karyotype and histomorphology — determines whether this patient goes home reassured or enters a surveillance protocol for gestational trophoblastic neoplasia.
This SDL teaches you to answer that question from the glass slide — and to extend the same morphology-first thinking to every major female genital tract lesion you will meet at the practical bench.
WHY THIS MATTERS
Gestational trophoblastic disease (GTD) is one of the few human cancers curable even with widespread metastasis, because of its extraordinary sensitivity to chemotherapy. That curability hinges on early recognition — which hinges on histology and serial hCG. For the NMC practical, the female genital tract is one of the highest-yield organ systems: the examiner can show you a cervicitis smear, an endometrial hyperplasia strip, a fibroid uterus, an ovarian cystic teratoma, or a choriocarcinoma — sometimes three in a single session. PA29.5 and PA29.10 together cover the full range. This SDL synthesises both into a single practical-facing document.
RECALL
Before you proceed, test your baseline:
- Name two morphological features that distinguish a complete hydatidiform mole from hydropic degeneration of a miscarriage.
- What is the chromosome complement of a partial mole?
- The term 'biphasic pattern' in trophoblastic tumors refers to which two cell types?
- Name three ovarian tumors associated with specific serum tumor markers.
- What microscopic triad defines endometriosis?
If questions 1, 3, or 5 are uncertain, flag those sections as you read.
Complete Hydatidiform Mole — Karyotype, Pathogenesis, and Morphology
Complete hydatidiform mole (CHM) arises from fertilisation of an empty (anucleate) ovum by a single sperm that then duplicates its genome, yielding a diploid androgenetic karyotype — 46,XX in ~90% of cases (or 46,XY if two different sperm fertilise the empty egg). Because all chromosomes are paternal, the placental tissue grows abnormally while embryonic development fails entirely.
Pathogenesis: Paternal imprinting normally suppresses trophoblastic proliferation; with a purely androgenetic genome, this suppression is lost, driving uncontrolled villous trophoblast expansion and massive hCG secretion.
Gross appearance: The uterine cavity is packed with translucent, fluid-filled vesicular villi resembling a bunch of grapes; no identifiable fetus or fetal membranes.
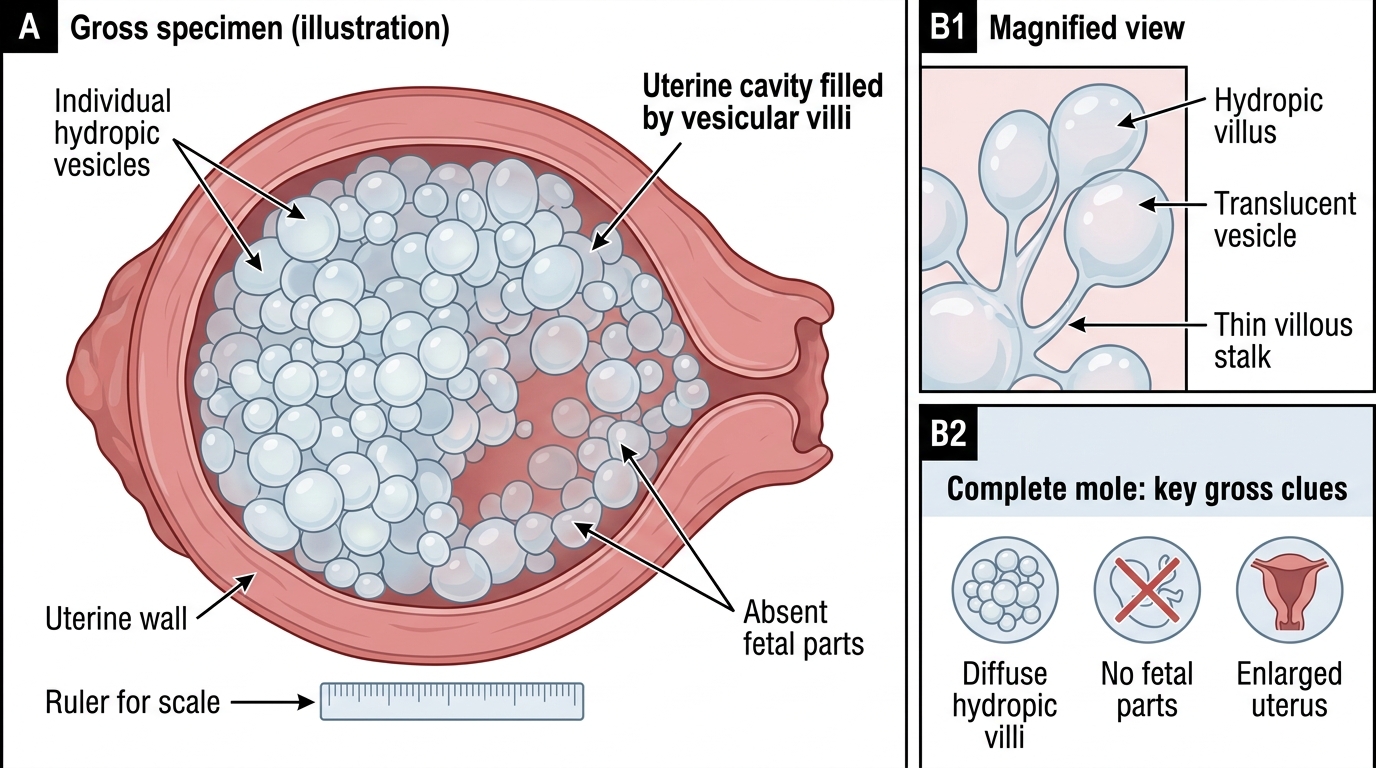
Complete Hydatidiform Mole: Gross Appearance
Microscopy: All villi are hydropic (stromal oedema with central cistern formation), avascular (no fetal vessels), and show circumferential trophoblastic hyperplasia involving both cyto- and syncytiotrophoblast. Atypia in the trophoblastic cells is the histological red flag for progression.
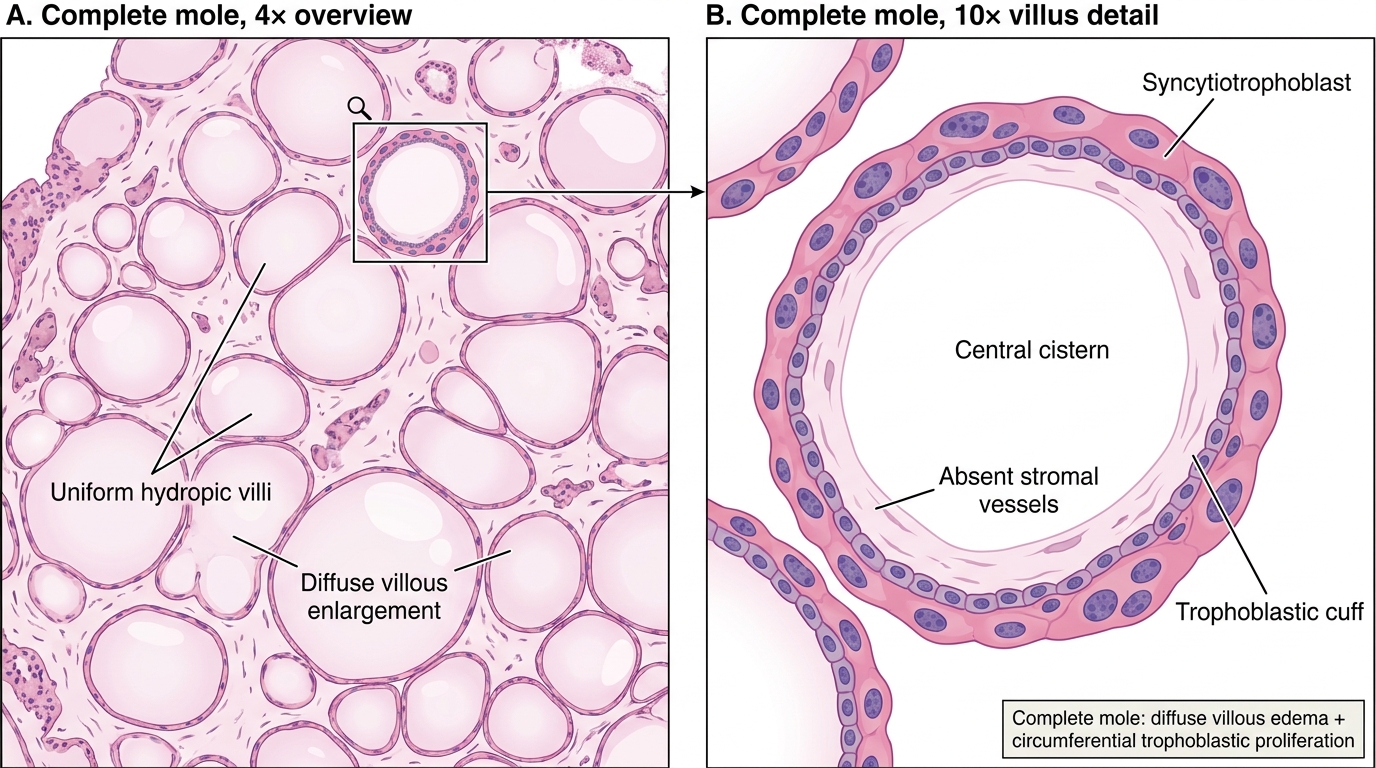
Complete Hydatidiform Mole on H&E
Clinical features: Uterus large-for-dates; hCG markedly elevated (often >100,000 mIU/mL); theca-lutein cysts in ovaries from hCG stimulation; risk of preeclampsia before 20 weeks. Risk of progression to persistent GTD or choriocarcinoma ~15–20% — highest of all GTD categories.
Partial Hydatidiform Mole — Karyotype, Pathology, and Comparison with Complete Mole
Partial hydatidiform mole (PHM) results from fertilisation of a normal ovum by two sperms (dispermy), producing a triploid karyotype — 69,XXY (most common), 69,XXX, or 69,XYY. One set of chromosomes is maternal, two are paternal.
Gross appearance: Only some villi are hydropic; fetal parts (embryo, cord, membranes) are often identifiable. The molar change is focal, not diffuse.
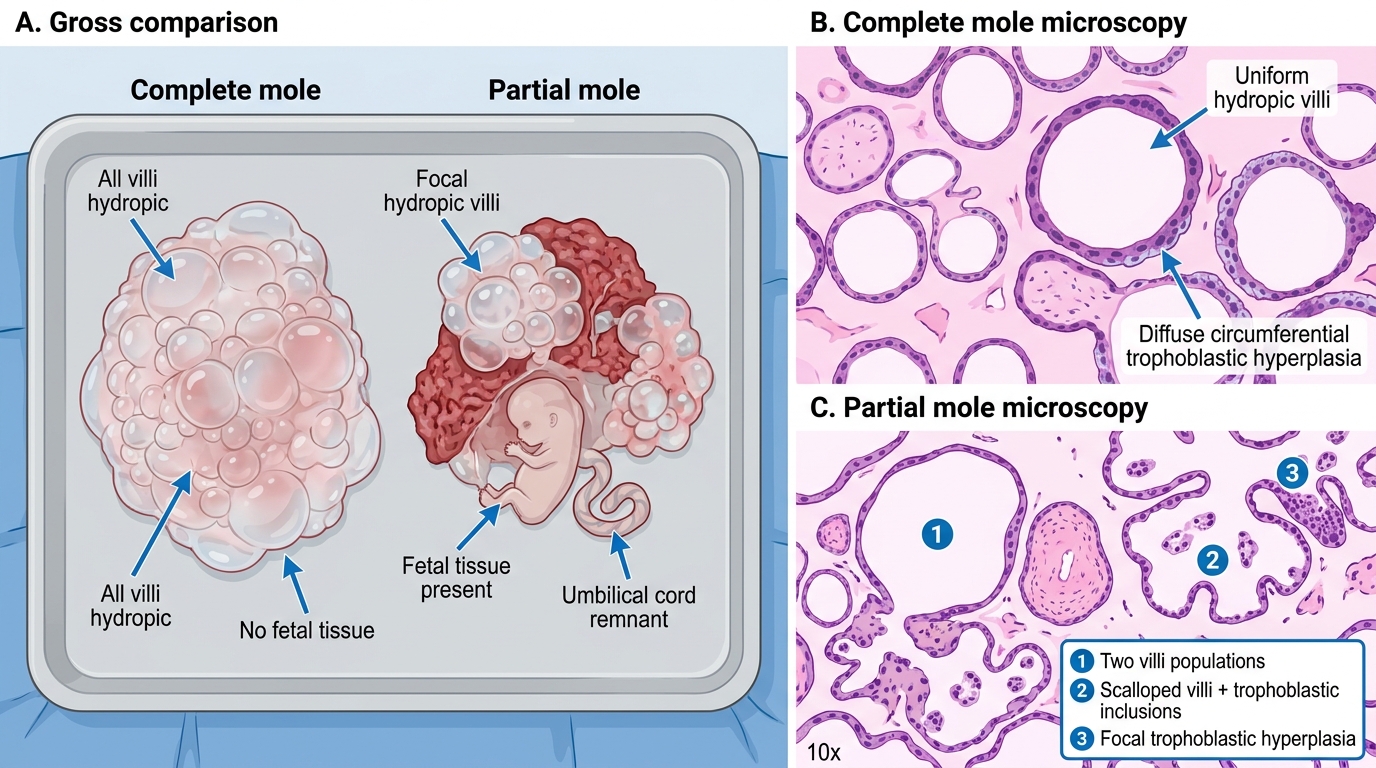
Complete Mole vs Partial Mole
Microscopy — the three hallmarks of PHM:
1. Two villi populations — large hydropic villi alternating with small fibrotic normal villi
2. Scalloped (fjord-like) villi with irregular outlines and trophoblastic inclusions (invaginations of trophoblast into the stroma)
3. Focal trophoblastic hyperplasia (far less than the circumferential proliferation of CHM)
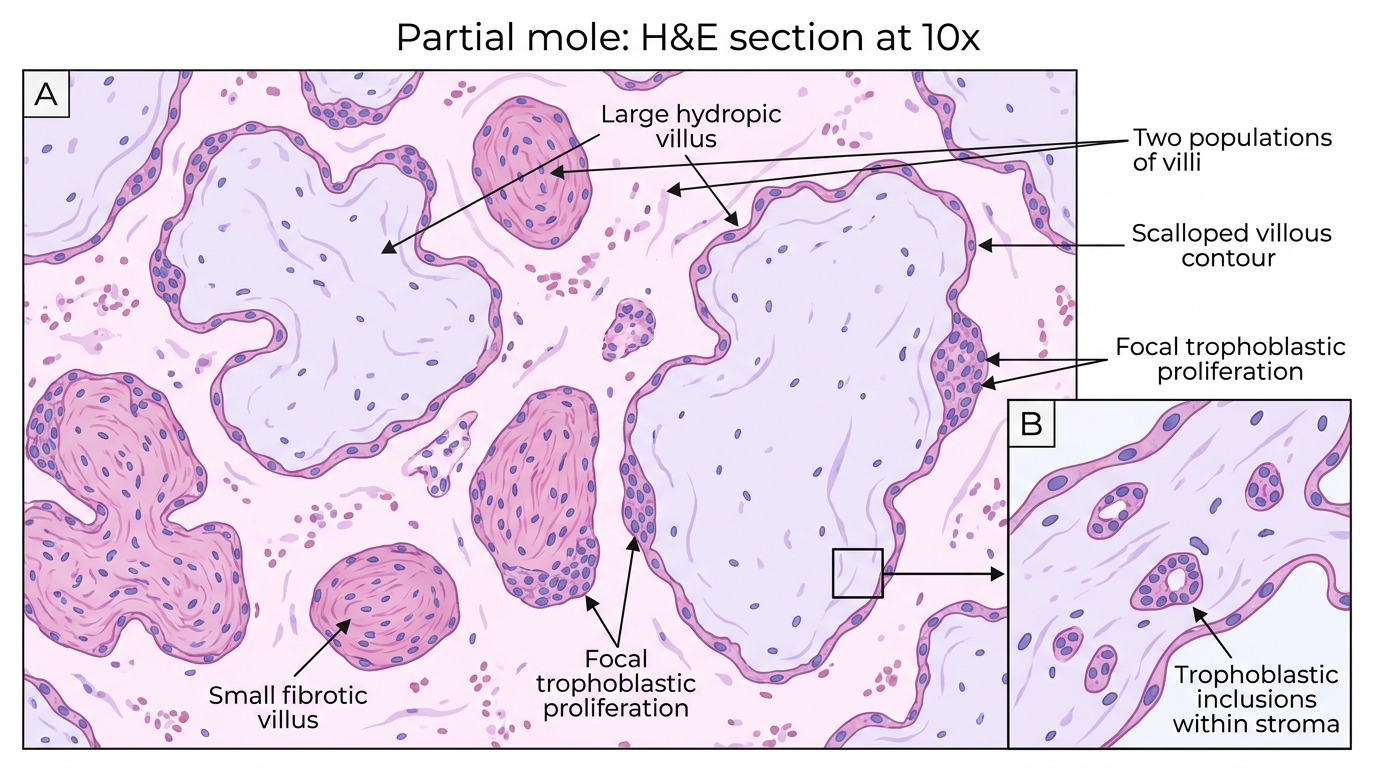
Partial Mole on H&E at 10x
Comparison table:
| Feature | Complete Mole | Partial Mole |
|---|---|---|
| Karyotype | 46,XX (androgenetic diploid) | 69,XXY (triploid) |
| Fetal parts | Absent | May be present |
| Villi | All hydropic | Mixed (hydropic + normal) |
| Trophoblastic hyperplasia | Circumferential | Focal |
| hCG | Very high | Moderately elevated |
| Choriocarcinoma risk | ~2% | Negligible |
hCG in PHM is lower than in CHM; ultrasound shows a mixed echo pattern rather than the classic snowstorm. Choriocarcinoma following a partial mole is extremely rare.
CLINICAL PEARL
The p57 immunostain discriminates CHM from PHM and hydropic abortion. p57^KIP2^ is a paternally imprinted, maternally expressed gene product — it is absent from trophoblast and villous stroma in a complete mole (entirely androgenetic genome → no maternal allele expressed) but positive in partial moles and hydropic abortions (maternal chromosomes present). In practice: p57-negative trophoblast + p57-negative stroma on a hydropic specimen = complete mole, refer for GTD surveillance.
Invasive Mole, Choriocarcinoma, and Placental Site Trophoblastic Tumor
Invasive mole is characterised by molar villi invading directly into the myometrium or entering uterine vasculature. The villi retain their histological identity (unlike choriocarcinoma). Clinically important because it can cause uterine perforation or distant emboli (most commonly to lung), but it almost never metastasises as true malignancy and responds well to chemotherapy.
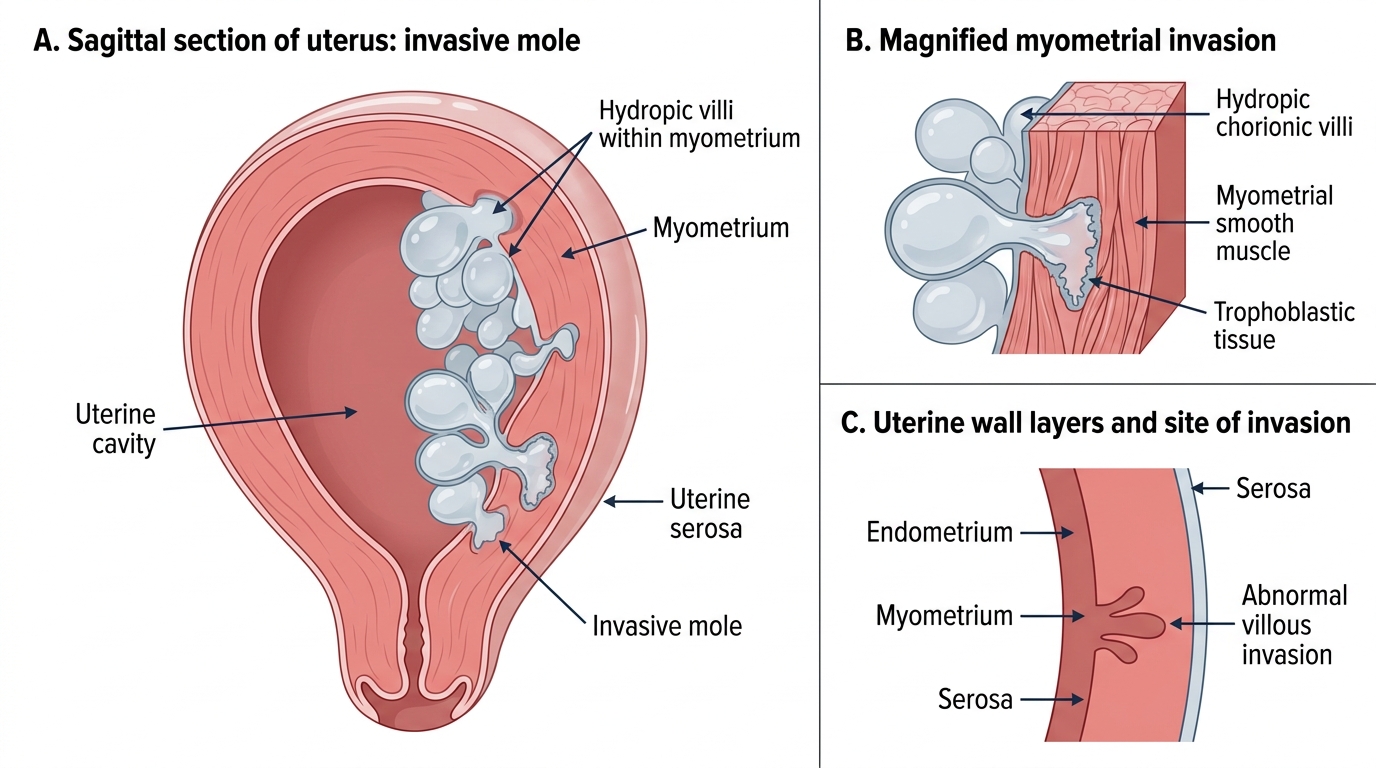
Invasive Mole in Sagittal Section of Uterus
Choriocarcinoma is a highly malignant tumor of trophoblast. Key features:
- Biphasic pattern: sheets of pale cytotrophoblast (mononuclear, mitotically active) capped by syncytiotrophoblast (multinucleate giant cells with abundant eosinophilic cytoplasm) — no chorionic villi are present (their absence is a defining diagnostic criterion)
- Gross: Hemorrhagic, necrotic, dark-red mass in the uterus; the center is often entirely necrotic with only a thin viable rim
- Spread: Predominantly hematogenous — early and widespread metastases to lung (cannon-ball nodules on CXR), brain, liver, kidney
- hCG: Markedly elevated; used both for diagnosis and as the single most sensitive tumor marker for monitoring response
- Chemosensitivity: Extraordinary — methotrexate (± actinomycin D) achieves cure rates >95% even in metastatic disease
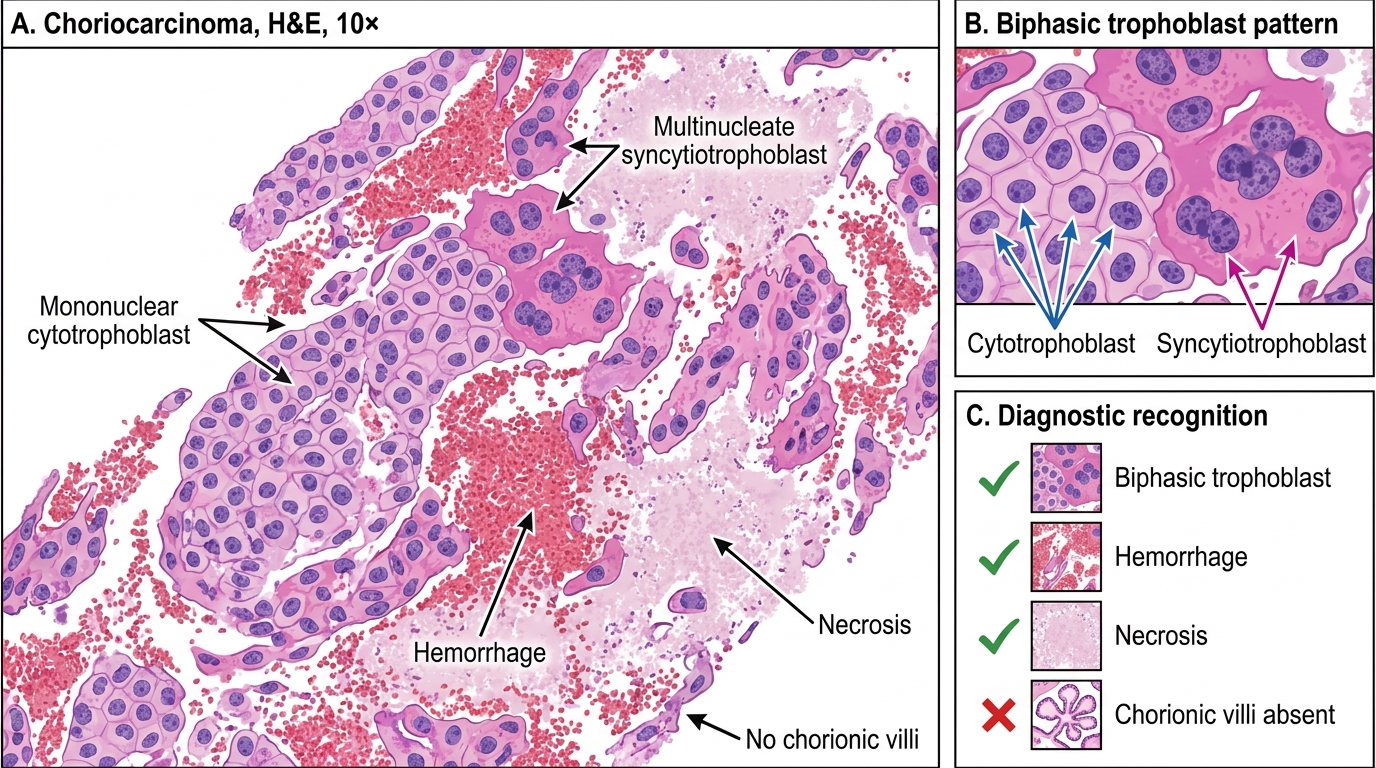
Choriocarcinoma: Biphasic Trophoblast Without Villi
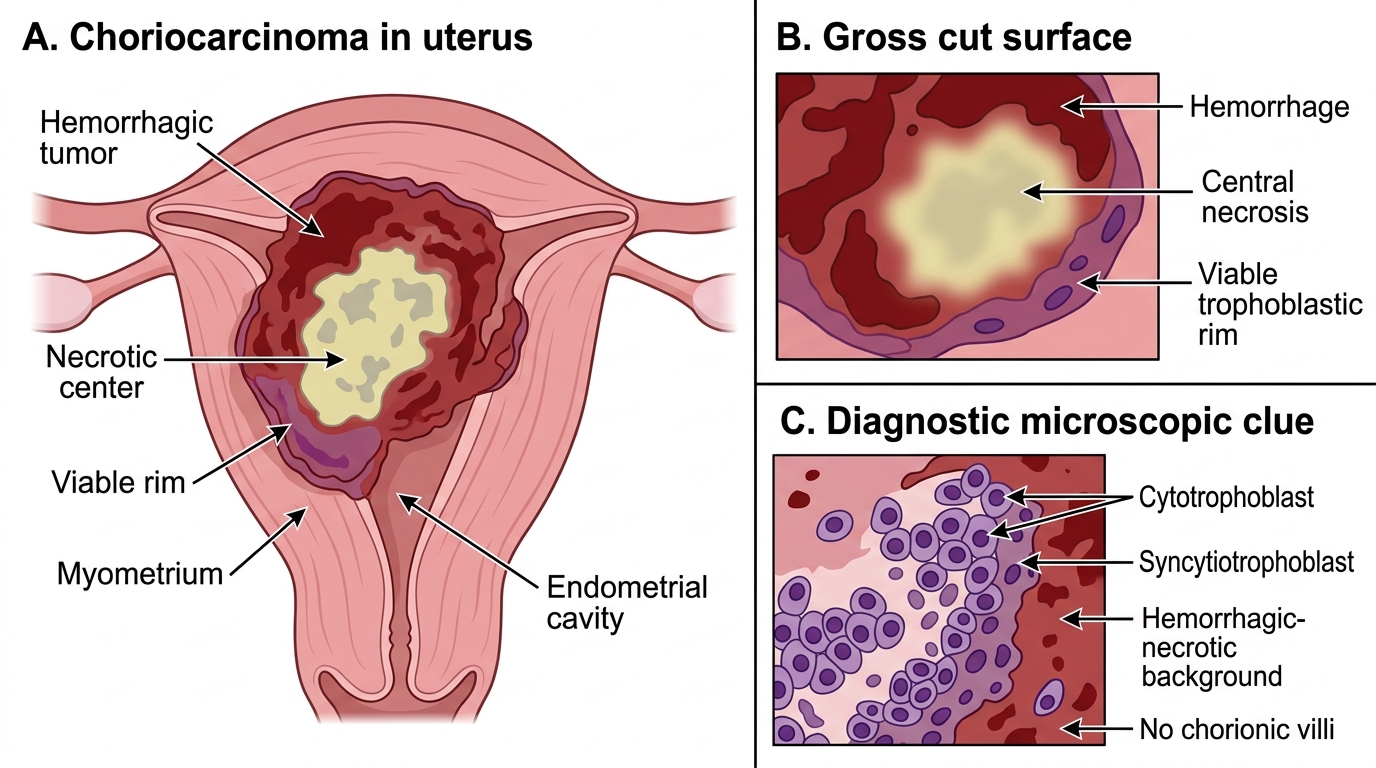
Choriocarcinoma of the Uterus: Gross and Diagnostic Features
Placental site trophoblastic tumor (PSTT) is a rare GTD arising from intermediate trophoblast at the placental implantation site:
- Composed of monomorphic intermediate trophoblastic cells infiltrating between myometrial fibers
- Secretes hPL (human placental lactogen) >> hCG (hCG is low or only mildly elevated — does NOT reliably track disease)
- Less chemosensitive than choriocarcinoma; treatment is hysterectomy rather than chemotherapy alone
- Intermediate prognosis between benign GTD and choriocarcinoma
SELF-CHECK
A 26-year-old has persistent uterine bleeding 8 months after a normal delivery. Serum hCG is 380 mIU/mL. Curettage shows sheets of mononuclear and multinucleate trophoblastic cells without any chorionic villi; the tumor is hemorrhagic and necrotic. What is the most likely diagnosis?
A. Complete hydatidiform mole
B. Partial hydatidiform mole
C. Choriocarcinoma
D. Placental site trophoblastic tumor
Reveal Answer
Answer: C. Choriocarcinoma
The defining histological feature here is the ABSENCE of chorionic villi with a biphasic trophoblastic proliferation (cytotrophoblast + syncytiotrophoblast) in a hemorrhagic-necrotic background — this is choriocarcinoma. A mole (complete or partial) always contains villi. PSTT is monomorphic intermediate trophoblast with low hCG and high hPL. Choriocarcinoma can arise after any pregnancy event including a normal delivery, molar pregnancy, or abortion.