Page 15 of 23
PA29.{5,10} | Gestational Trophoblastic Disease & Female Genital Morphology — SDL Guide (Part 2)
Cervix & Endometrium — Practical Recognition (Cervicitis and Endometriosis)
The second half of this SDL is your morphology-practical walk-through. The approach for every lesion is: Gross first → Architecture low power → Cell detail high power → Clinical correlate.
Cervicitis
Acute cervicitis: Mucosal surface infiltrated by neutrophils; surface erosion common. Associated with Neisseria gonorrhoeae, Chlamydia trachomatis (intracellular organisms not visible on H&E — require special tests). Clinically: mucopurulent discharge.
Chronic cervicitis: Dense lymphoplasmacytic infiltrate in the stroma; reactive squamous metaplasia in the transformation zone; nabothian cysts (mucus retention) may be grossly visible as pearly white nodules on the ectocervix.
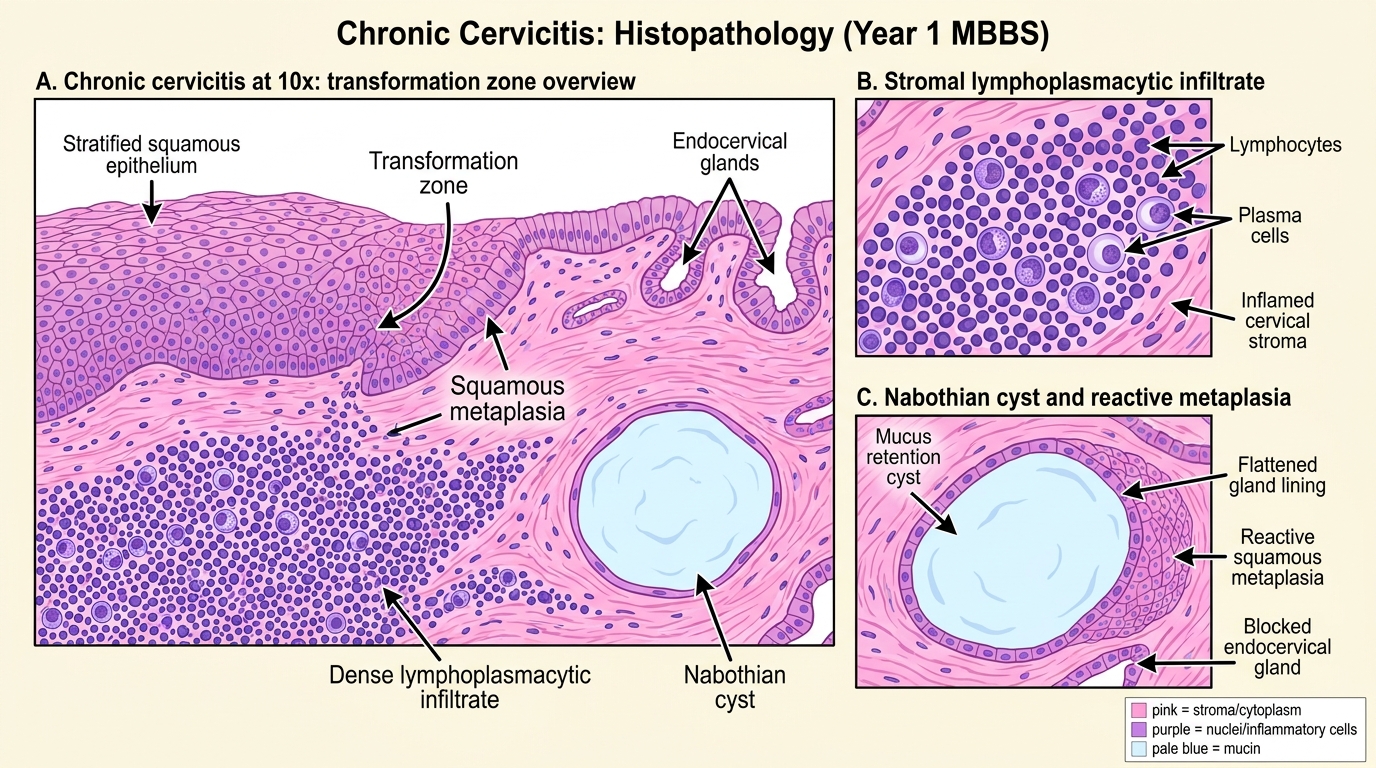
Chronic Cervicitis: H&E Recognition at 10x
Endometriosis (PA29.10 high-yield practical)
Defined by the triad:
1. Endometrial glands outside the uterine cavity
2. Endometrial stroma surrounding those glands
3. Hemosiderin-laden macrophages (evidence of cyclical hemorrhage)
Gross: chocolate cysts (endometriomas) in the ovary — filled with dark brown, thick, altered blood. Powder-burn lesions on peritoneum.
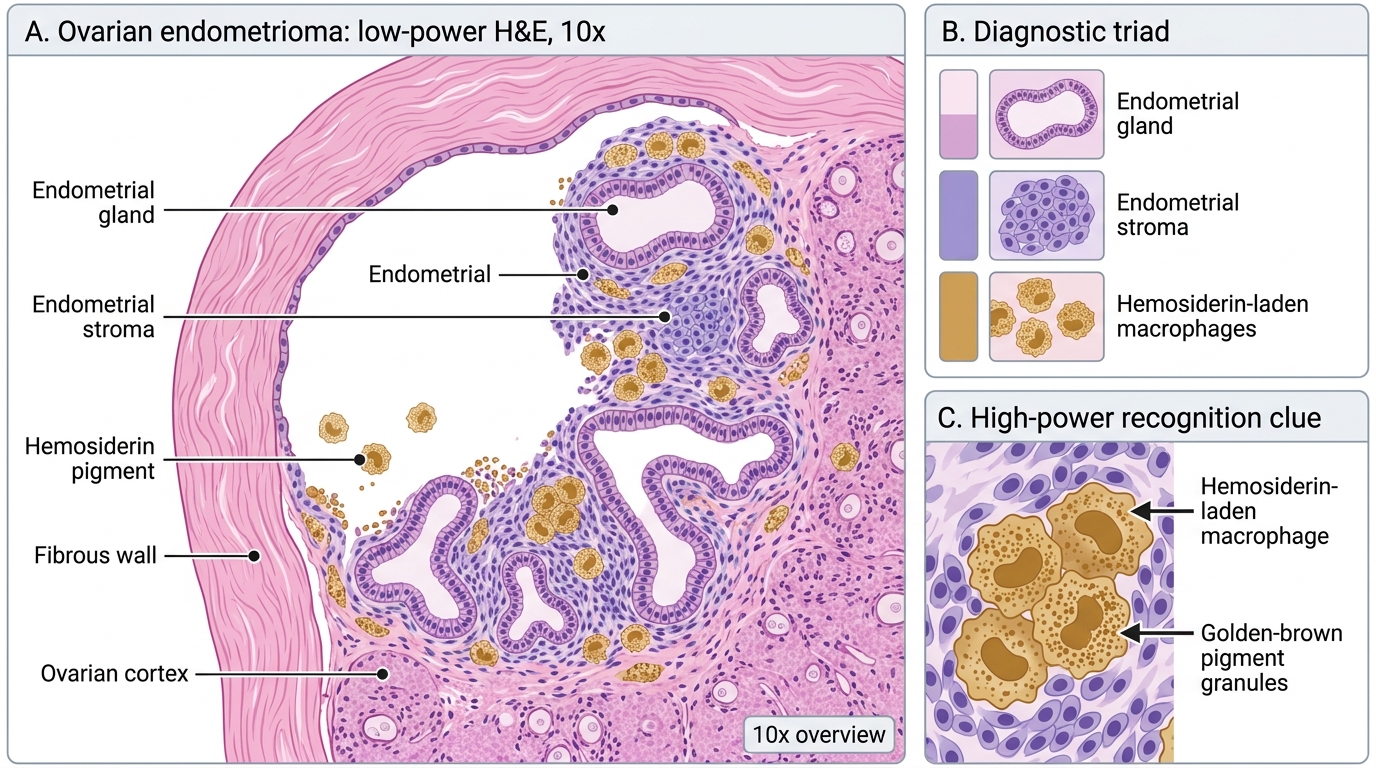
Ovarian Endometrioma on H&E
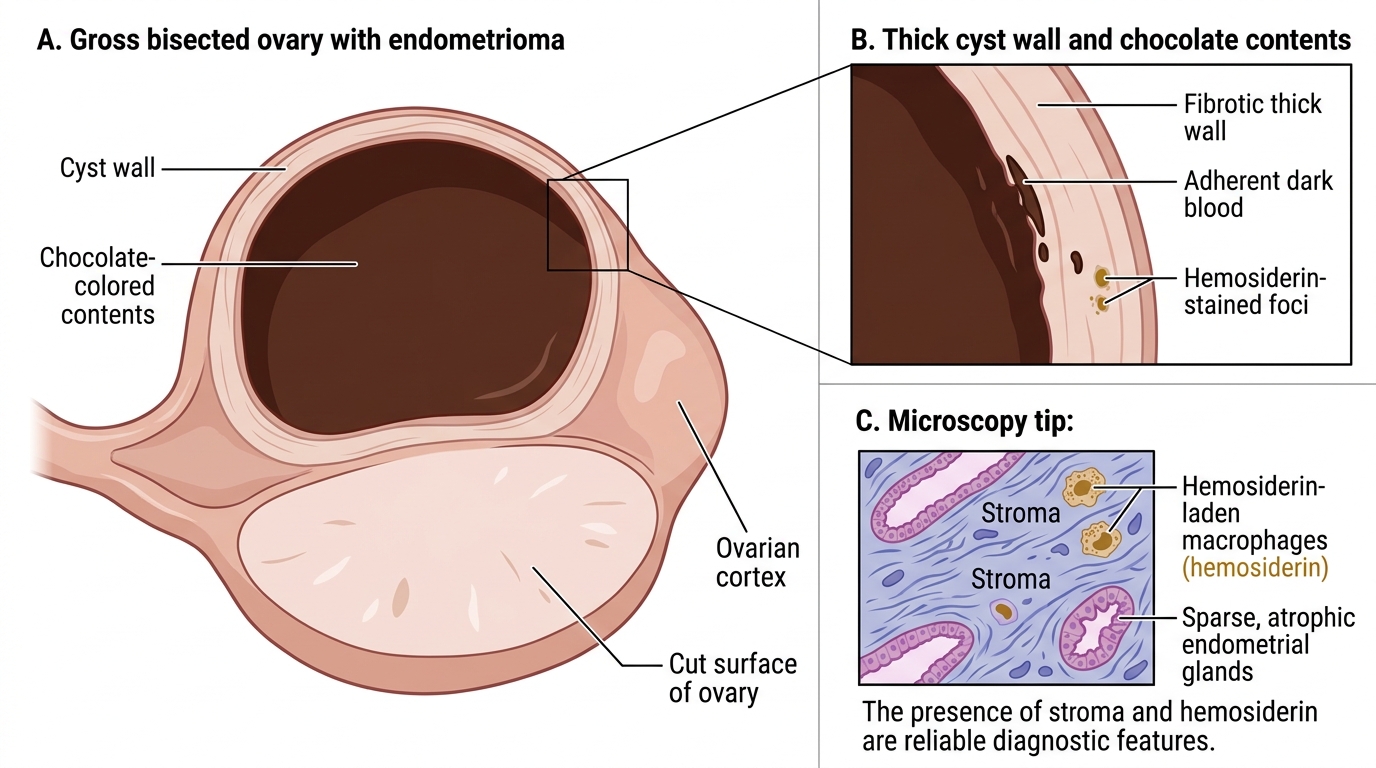
Ovarian Chocolate Cyst Endometrioma
Microscopy tip: The glands may be atrophic or inactive — the stroma and hemosiderin are the more reliable diagnostic features when endometrial glands look bland.
Endometrial Hyperplasia vs Endometrial Carcinoma — Pattern Recognition
Endometrial hyperplasia (WHO classification: simple → complex → atypical) is the morphological spectrum from glandular crowding without atypia to the precancerous lesion with nuclear atypia.
Simple hyperplasia: Increased gland-to-stroma ratio; glands dilated (cystically), lined by bland columnar cells; architecture abnormal but orderly.
Complex hyperplasia: Markedly crowded, back-to-back glands, minimal intervening stroma; no nuclear atypia → low malignant potential.
Atypical hyperplasia: Same crowded architecture PLUS nuclear atypia (large vesicular nuclei, prominent nucleoli, loss of polarity) — the direct precursor to endometrioid carcinoma; ~25–30% risk of progression.
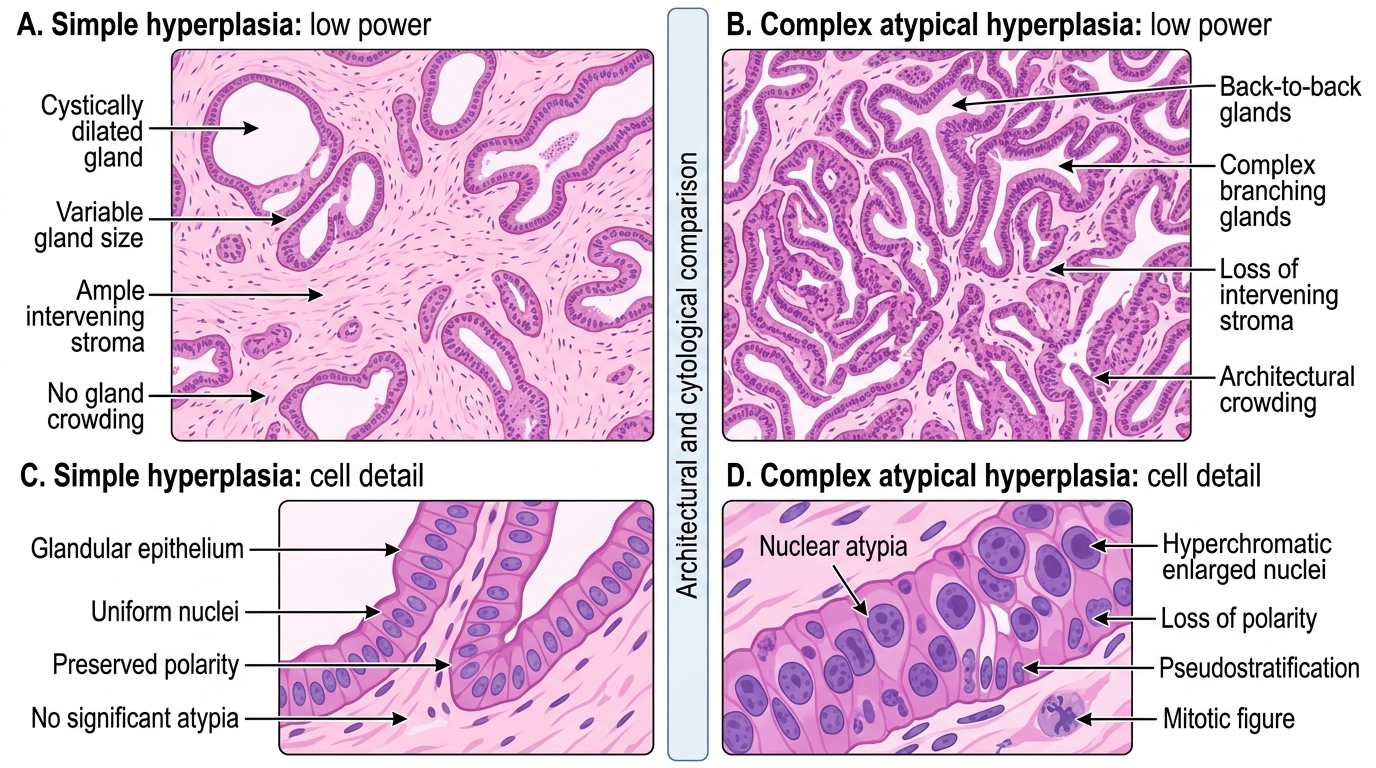
Simple vs Complex Atypical Endometrial Hyperplasia
Endometrioid endometrial carcinoma (most common type, ~80%):
- Gross: Polypoid or fungating mass arising in fundus or posterior wall; pale, soft, friable
- Micro: Infiltrative glands with stromal desmoplasia; malignant glands may closely mimic complex atypical hyperplasia, but invasion (irregular infiltration, desmoplastic stroma, back-to-back glands without stroma) confirms carcinoma
- Grade is by architectural pattern: Grade 1 = >95% glandular; Grade 3 = >50% solid
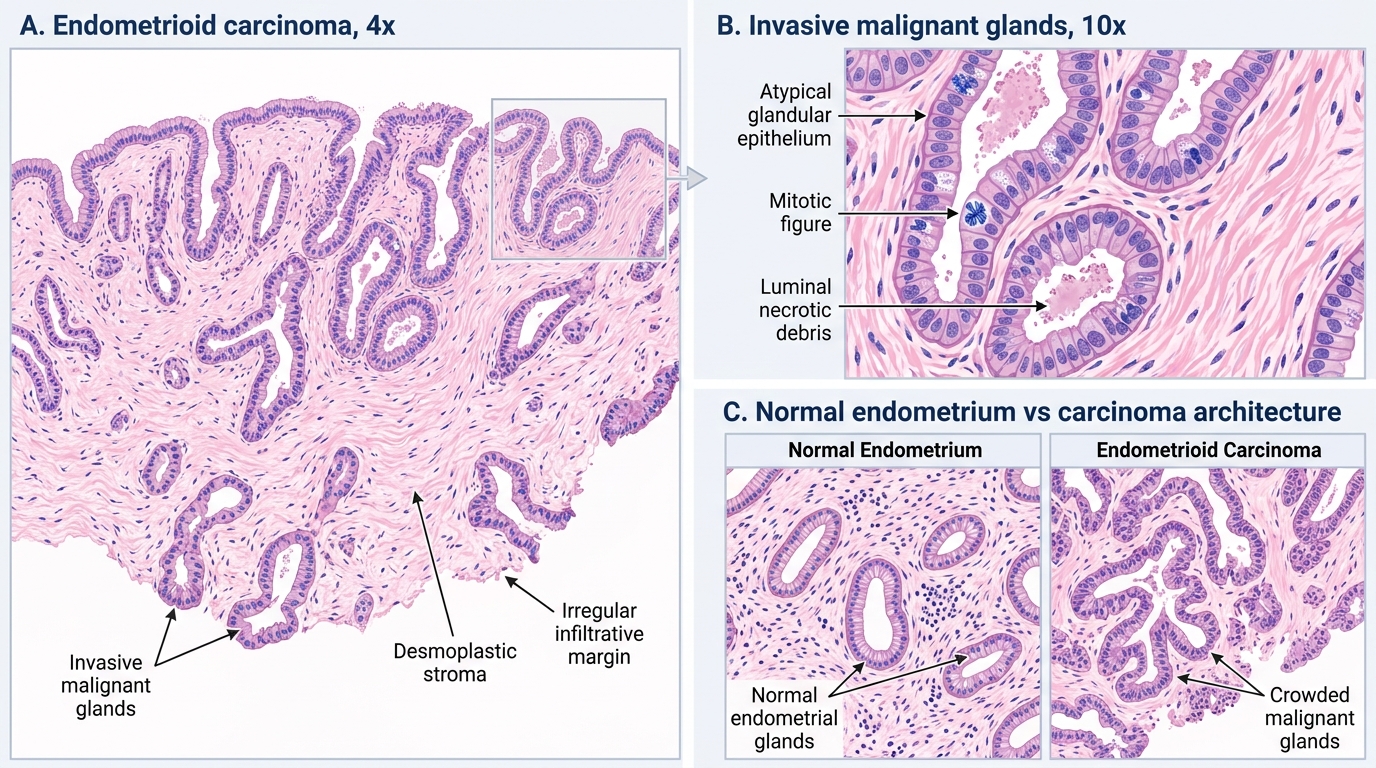
Endometrioid Endometrial Carcinoma: Invasive Glands and Desmoplasia
CLINICAL PEARL
'Atypical hyperplasia' and 'endometrial intraepithelial neoplasia (EIN)' are the same lesion under different classification systems. The 2003 WHO classification uses the 4-tier scheme (simple/complex ± atypia); the EIN schema (more reproducible) uses a single binary: EIN (precancer) vs not-EIN. In practice, when you see 'atypical hyperplasia' in a report, treat it as a high-risk precancer requiring hysterectomy workup, not watchful waiting. Coexistent carcinoma is found in 25–40% of hysterectomy specimens resected for atypical hyperplasia diagnosed on biopsy.
Leiomyoma vs Leiomyosarcoma — Myometrial Tumors
Leiomyoma (fibroid) is the most common benign pelvic tumor in women.
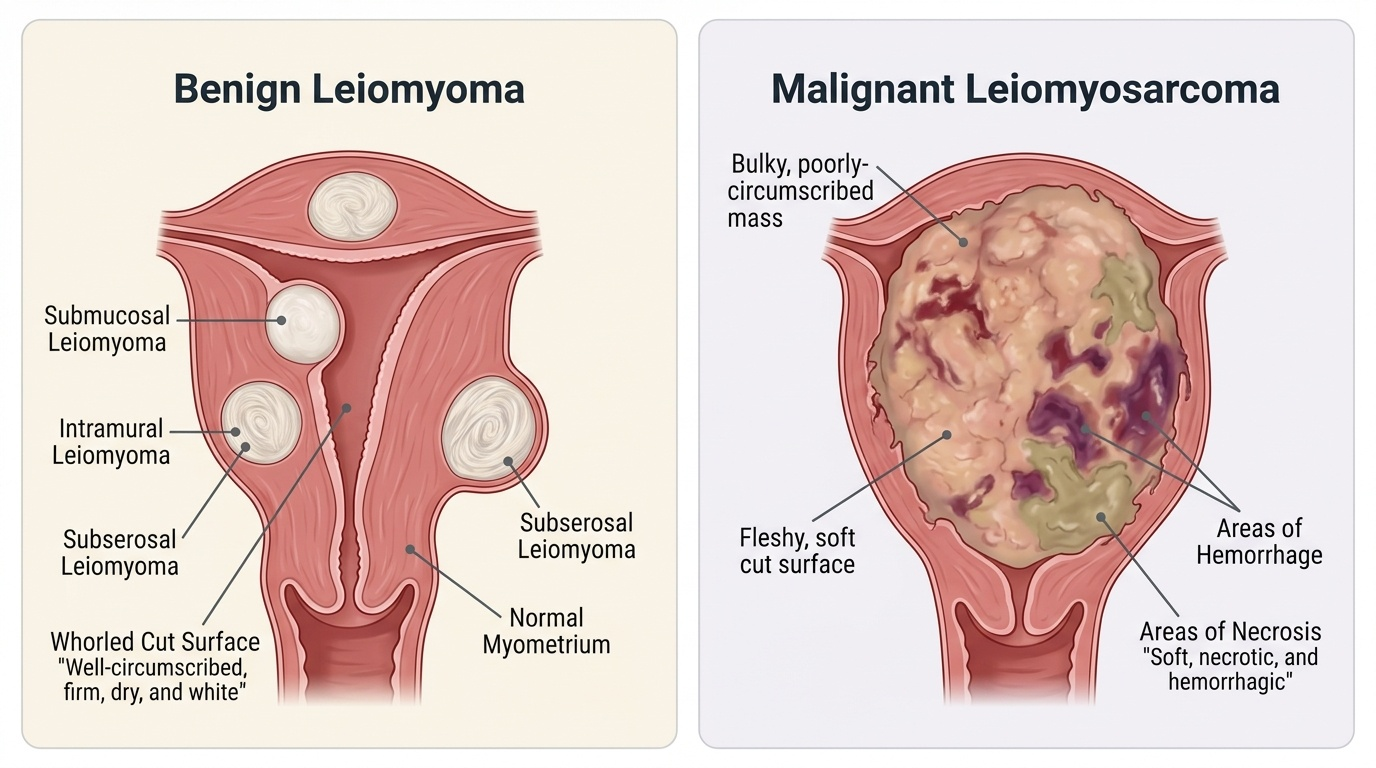
Provided image
Gross: Well-circumscribed, firm, white, whorled nodules within the myometrium (intramural), projecting into the uterine cavity (submucosal), or beneath the serosa (subserosal). May be multiple. Cut surface: interlacing white bundles with a 'whorled' pattern.
Micro: Uniform spindle cells arranged in intersecting fascicles; no nuclear atypia, few or no mitoses; cells have blunt-ended ('cigar-shaped') nuclei; no necrosis.
Leiomyosarcoma — malignant smooth muscle tumor: de novo, not from leiomyoma.
Gross: Larger, bulky, soft, fleshy, with areas of hemorrhage and necrosis (contrast with the firm, white, dry cut surface of a fibroid).
Micro: The Stanford triad of malignancy — (1) nuclear atypia (pleomorphism, prominent nucleoli), (2) ≥10 mitoses/10 HPF, (3) coagulative tumor cell necrosis. Any two of the three, especially the mitotic count, essentially confirms malignancy.
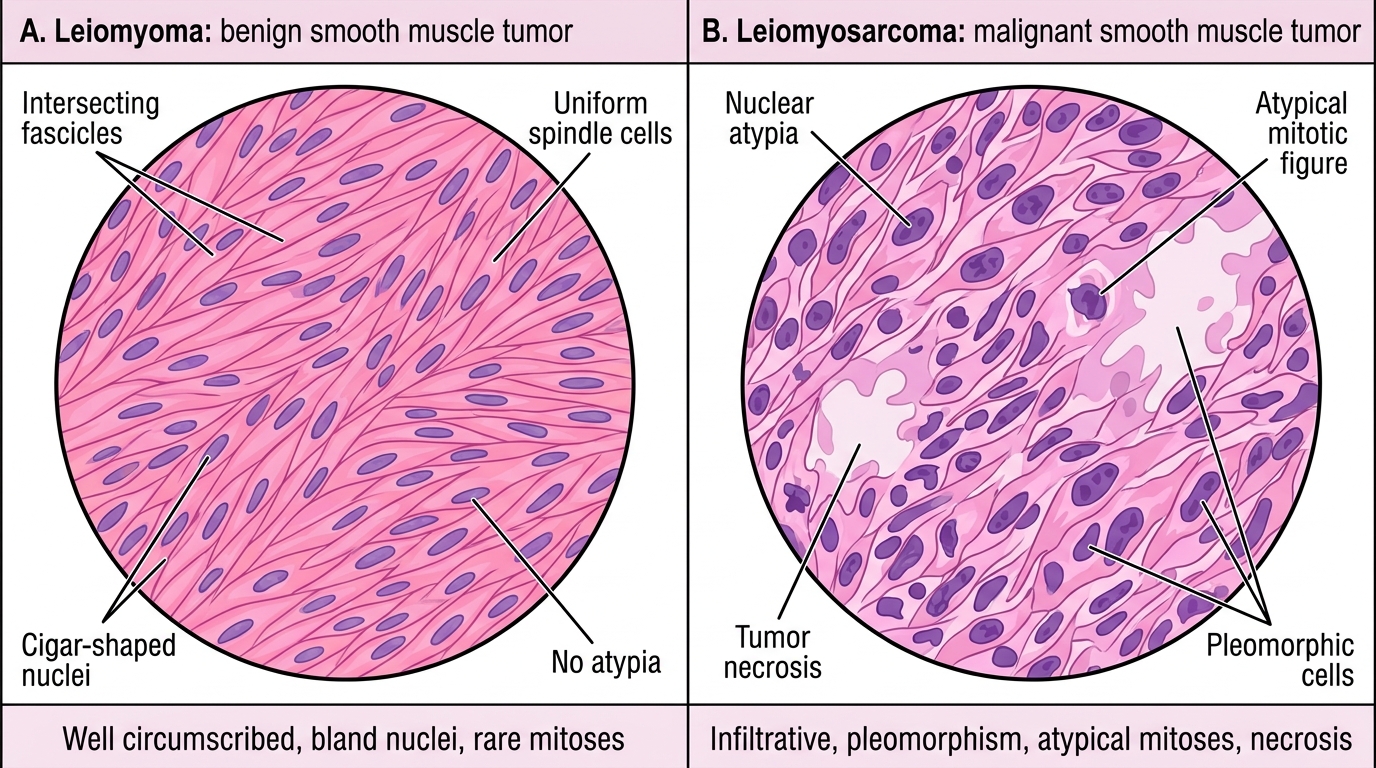
Leiomyoma vs Leiomyosarcoma on H&E
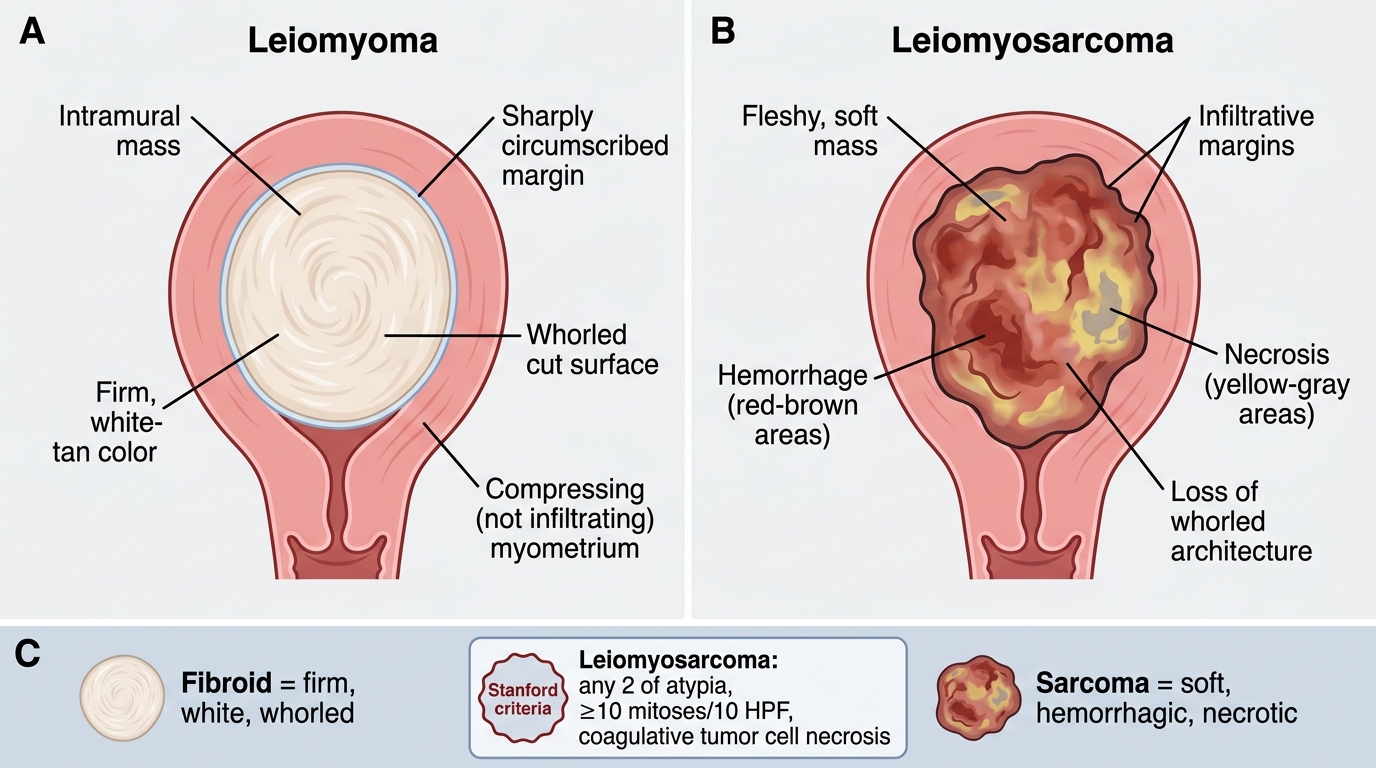
Gross Comparison: Leiomyoma vs Leiomyosarcoma
Memory rule: Fibroid = firm, white, whorled; Leiomyosarcoma = soft, hemorrhagic, necrotic. If the cut surface looks like 'brain with a bleed' rather than 'white rubber', think sarcoma.
SELF-CHECK
Histological sections of a uterine spindle-cell tumor show: 12 mitoses per 10 HPFs, geographic coagulative necrosis, and moderate nuclear pleomorphism. The most appropriate diagnosis is:
A. Leiomyoma with hyaline degeneration
B. Cellular leiomyoma
C. Leiomyosarcoma
D. Endometrial stromal sarcoma
Reveal Answer
Answer: C. Leiomyosarcoma
The Stanford criteria for leiomyosarcoma require any 2 of: nuclear atypia, ≥10 mitoses/10 HPF, and coagulative tumor cell necrosis. This case has all three: 12 mitoses/10 HPF (exceeds threshold), coagulative necrosis, and moderate pleomorphism — unambiguous leiomyosarcoma. Cellular leiomyoma has increased cellularity but <5 mitoses/10 HPF and no atypia. Endometrial stromal sarcoma arises from the endometrial stroma (not smooth muscle) and has a different immunoprofile (CD10+).