Page 16 of 23
PA29.{5,10} | Gestational Trophoblastic Disease & Female Genital Morphology — SDL Guide (Part 3)
Ovarian Tumors — Epithelial Tumors: Serous and Mucinous
Ovarian tumors are classified by their cell of origin: surface epithelium (~70%), germ cells (~20%), sex-cord stromal (~8%), and metastatic (~5–10%). The practical exam requires recognition of each major type.
Serous tumors (most common epithelial subtype):
Benign serous cystadenoma: Unilocular or multilocular thin-walled cyst, smooth inner surface, watery serous fluid. Micro: single layer of ciliated tubal-type epithelium, no atypia, no stromal invasion.
Serous borderline tumor: Papillary projections into cyst lumen; micro: stratified epithelium, mild atypia, no destructive stromal invasion (< 5 mm microinvasion tolerated).
High-grade serous carcinoma (HGSC): Bilateral in ~70%; solid and cystic; papillary, micropapillary, or cribriform architecture; marked nuclear atypia, aberrant p53, TP53 mutation; slit-like spaces; psammoma bodies (laminated calcifications).
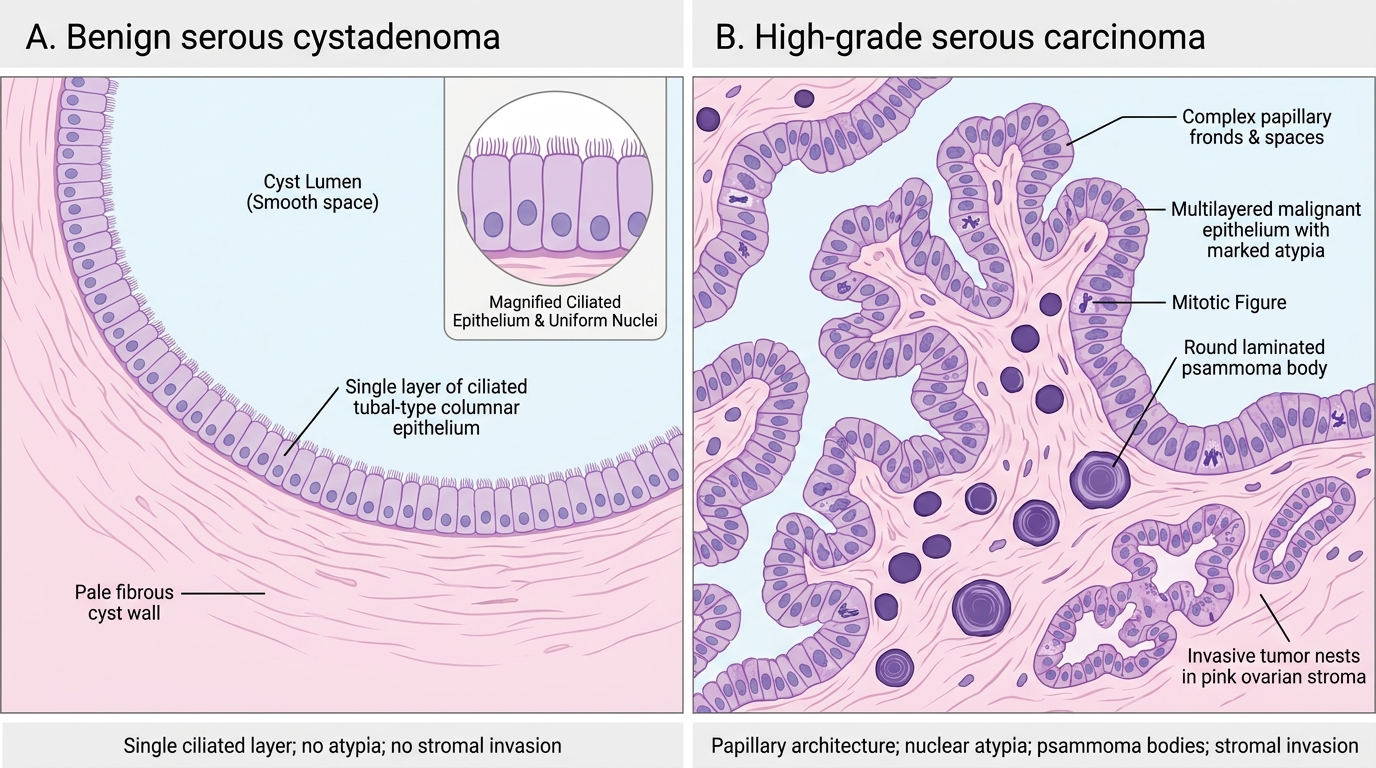
Serous Cystadenoma vs High-Grade Serous Carcinoma
Mucinous tumors:
Mucinous cystadenoma: Multilocular cyst filled with thick mucinous fluid; micro: tall columnar cells with basal nuclei and apical mucin (resembling endocervical or intestinal epithelium); no atypia.
Mucinous carcinoma: Infiltrative glands with stromal invasion; goblet cells may be present (intestinal type); distinguish from appendiceal mucinous carcinoma metastasis (bilateral mucinous = suspect metastasis).
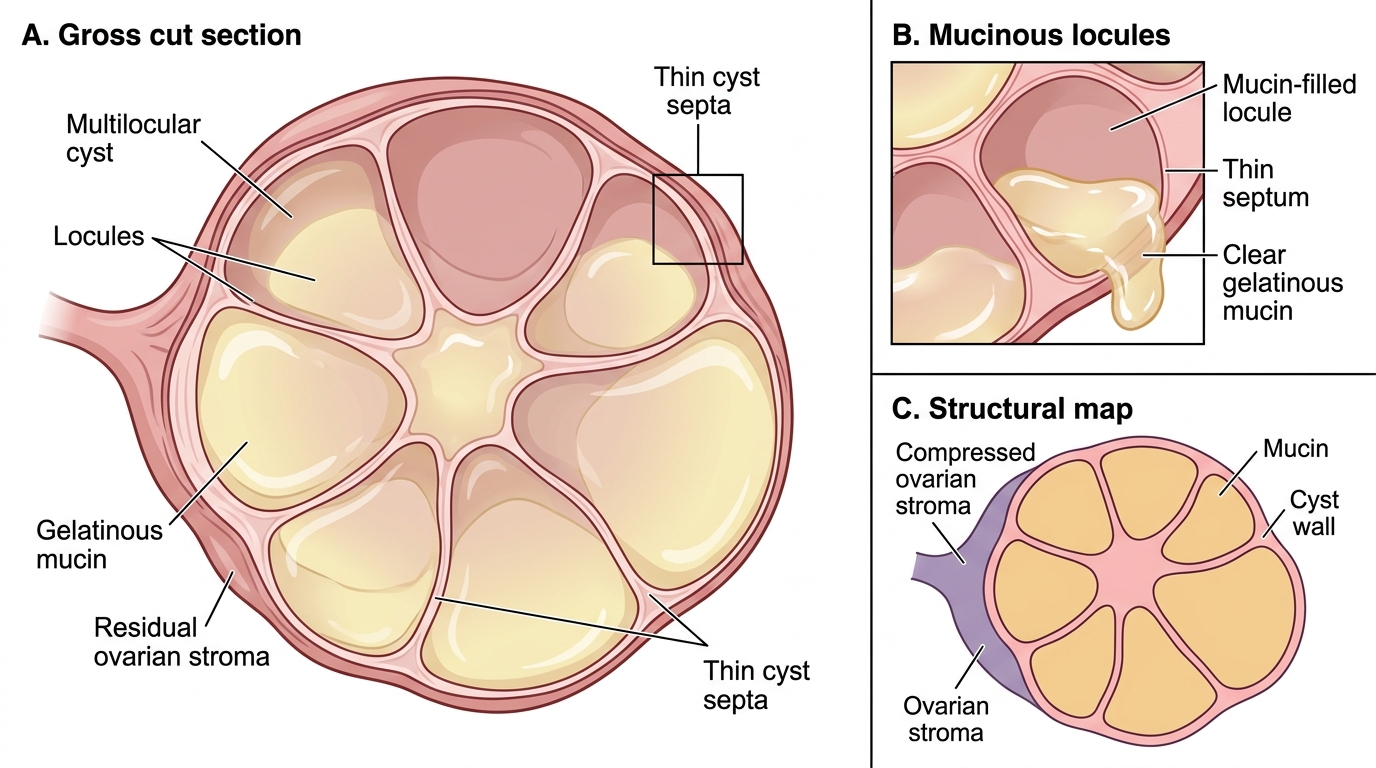
Gross Features of Ovarian Mucinous Cystadenoma
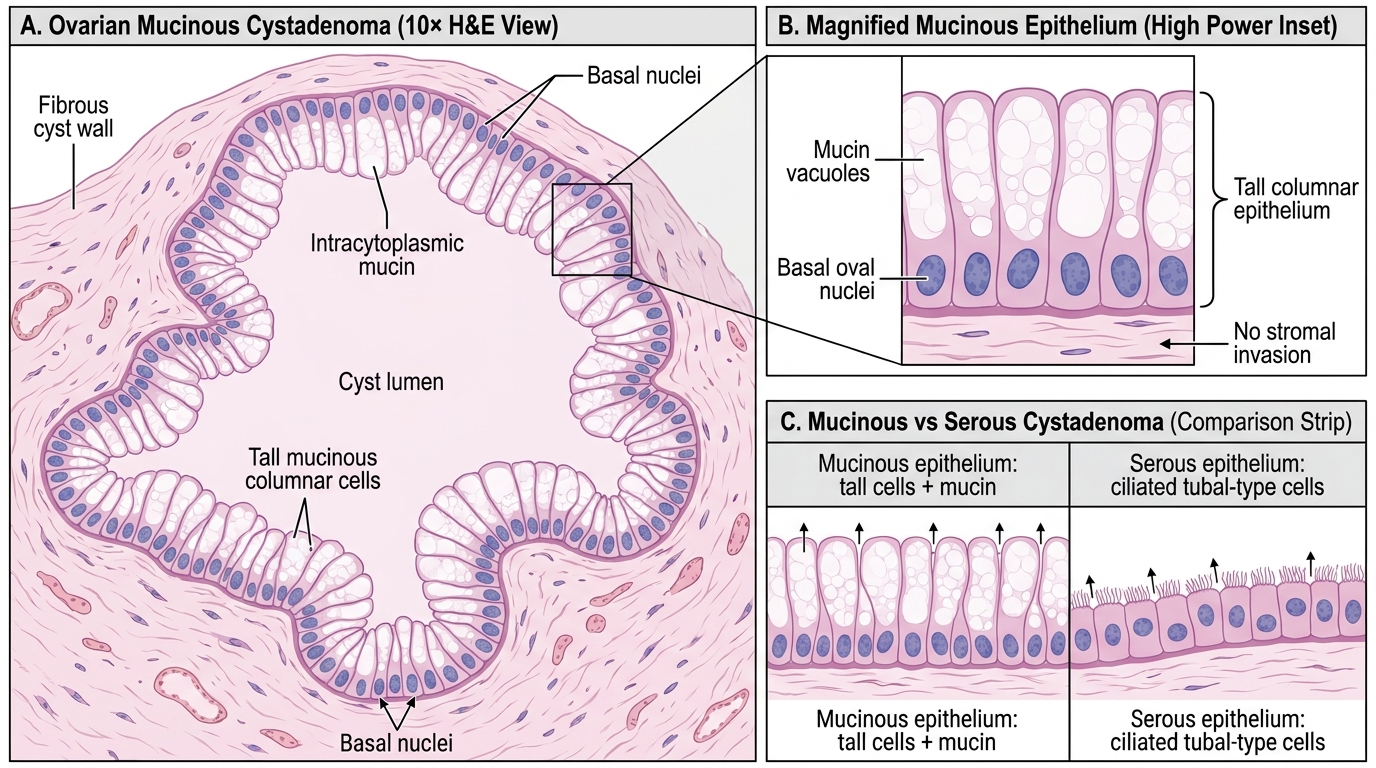
Mucinous Cystadenoma of Ovary: H&E 10× Features
Ovarian Tumors — Germ Cell, Sex-Cord Stromal, and Metastatic Tumors
Mature cystic teratoma (dermoid cyst) — most common ovarian germ-cell tumor:
- Gross: Cystic, contains hair, sebaceous material, teeth, bone (ectodermal elements dominate); cut surface shows a Rokitansky protuberance (solid mural nodule from which teeth/hair arise)
- Micro: All three germ layers — squamous epithelium with hair follicles, sebaceous glands (ectoderm); intestinal/respiratory epithelium (endoderm); cartilage, smooth muscle (mesoderm)
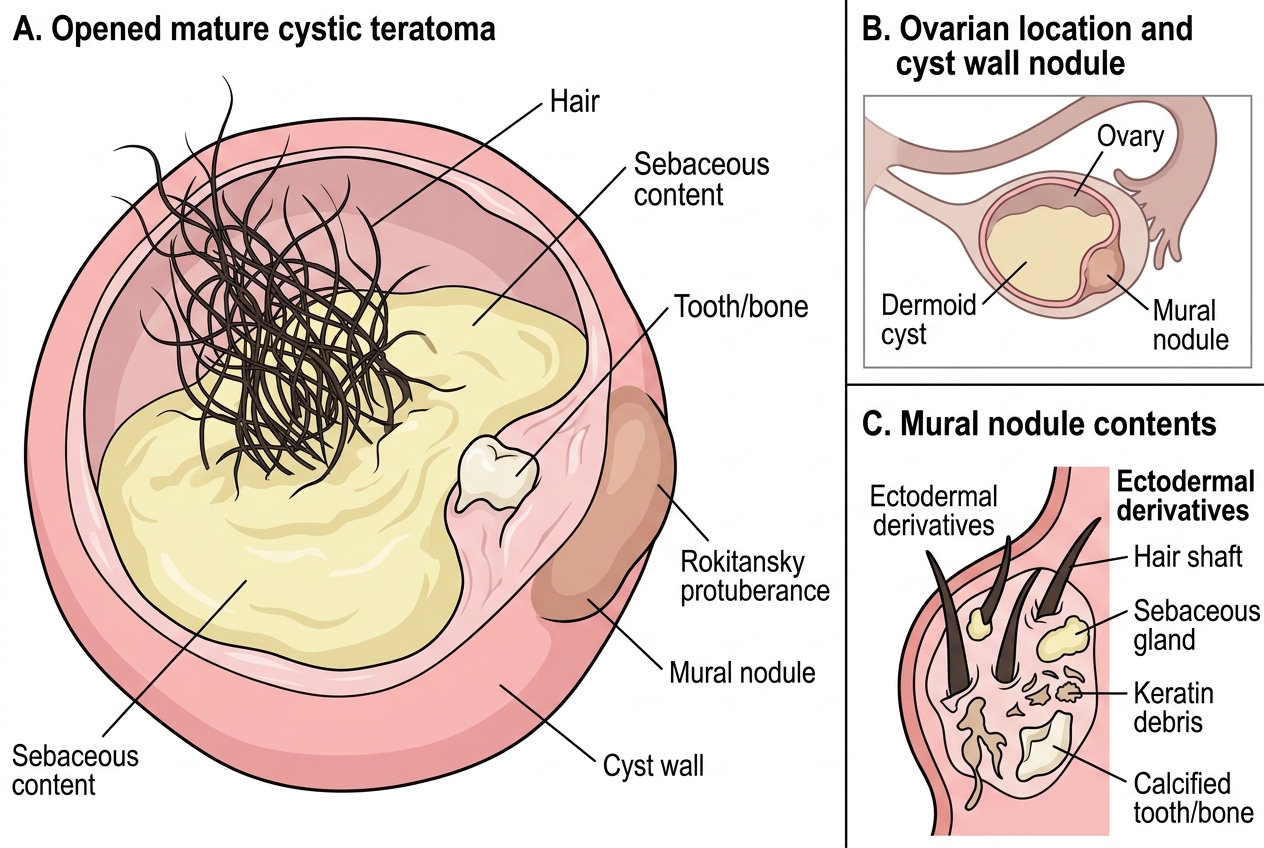
Mature Cystic Teratoma: Gross Features
Dysgerminoma (counterpart of testicular seminoma):
- Most common malignant ovarian germ-cell tumor in young women
- Gross: Solid, fleshy, cream-colored tumor
- Micro: Large polygonal cells with clear glycogen-rich cytoplasm and central prominent nuclei, arranged in sheets and nests separated by fibrous septa with lymphocytic infiltrate
- Marker: LDH and placental-like alkaline phosphatase (PLAP); hCG elevated only if syncytiotrophoblastic elements present
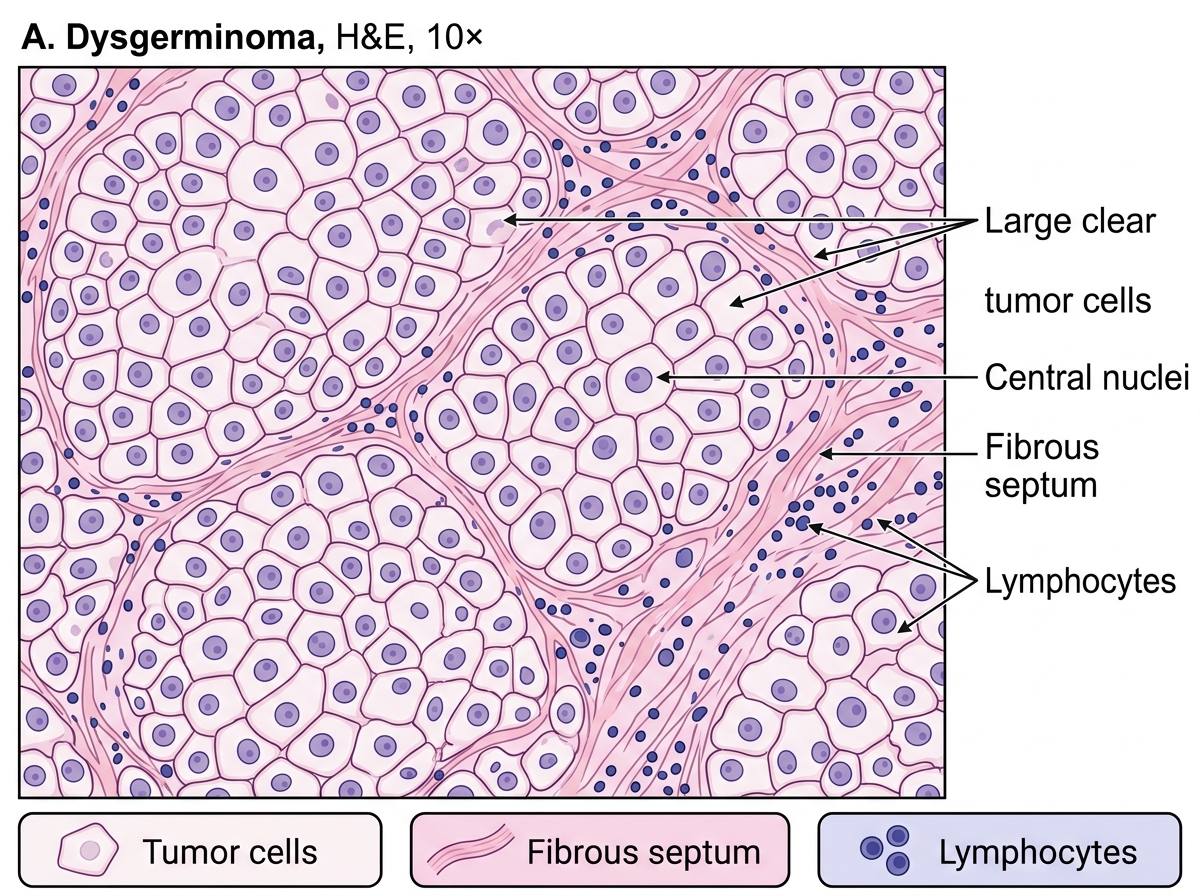
Dysgerminoma: H&E Section at 10×
Granulosa cell tumor (sex-cord stromal, most common):
- Gross: Solid and cystic, yellow-tinged (luteinization); may have hemorrhagic foci (danger: torsion or rupture → hemoperitoneum)
- Micro: Call-Exner bodies — rosette-like arrangements of granulosa cells around a central space containing eosinophilic material (resembling primordial follicles); 'coffee-bean' (longitudinally grooved) nuclei
- Endocrine: Produces estrogen → endometrial hyperplasia, precocious puberty (in girls), postmenopausal bleeding in older women
- Marker: Inhibin (serum and IHC)
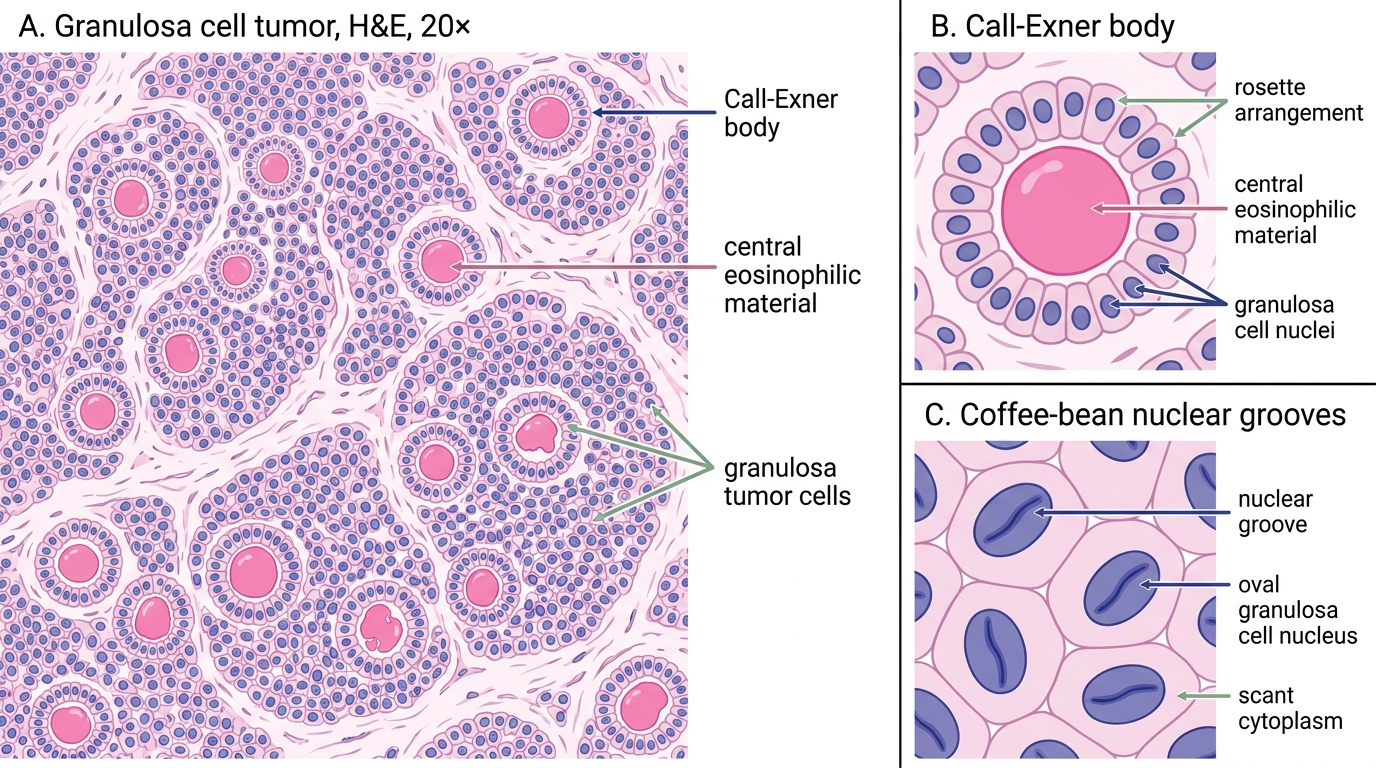
Granulosa Cell Tumor: Call-Exner Bodies and Nuclear Grooves
Krukenberg tumor (metastatic):
- Definition: Bilateral ovarian metastasis with signet-ring cells distending with mucin in a cellular fibromatous stroma
- Primary: Classically gastric adenocarcinoma (diffuse type); also colorectal, appendix, breast
- Gross: Bilateral, solid or solid-cystic; ovarian architecture partially preserved
- Micro: Signet-ring cells (nucleus pushed to periphery by mucin vacuole) in a hypercellular fibromatous ovarian stroma
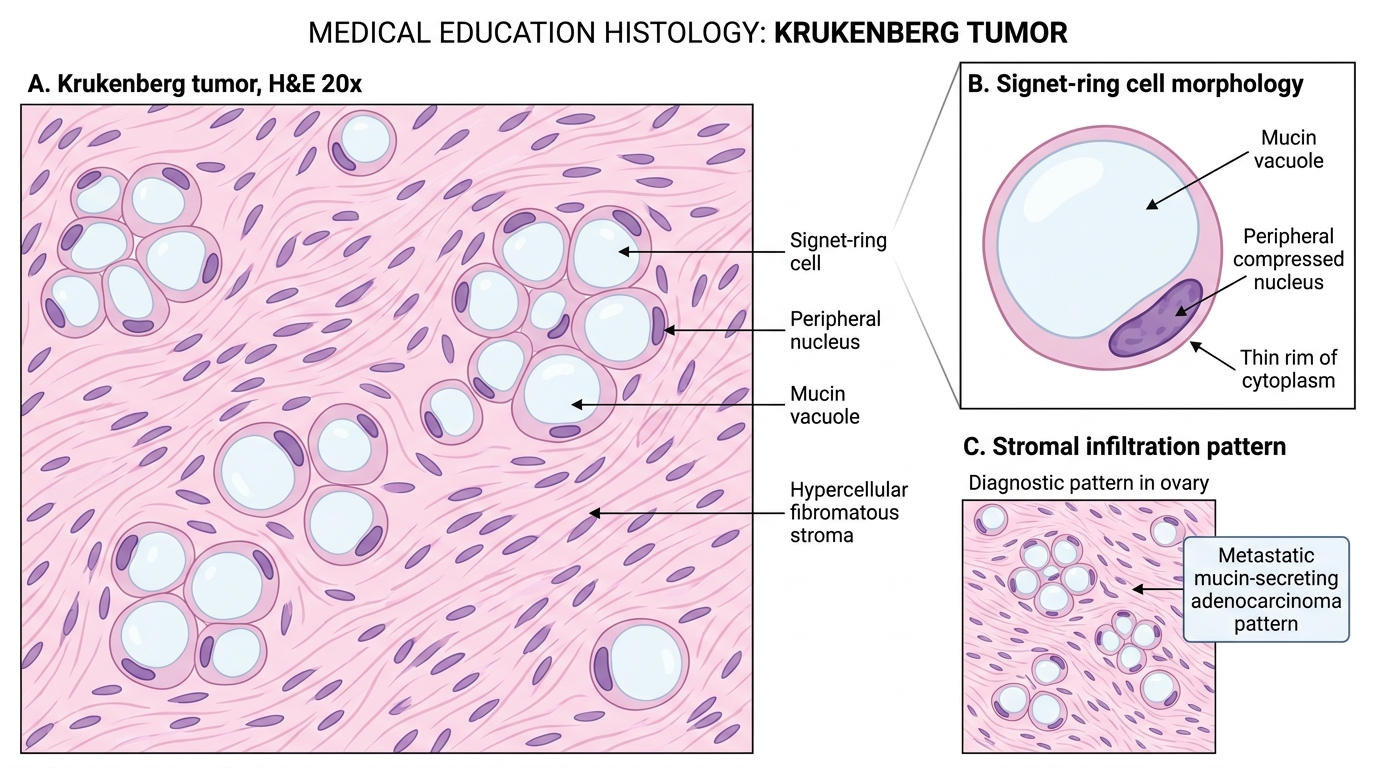
Krukenberg Tumor: Signet-Ring Cells in Ovarian Stroma
Master Recognition Table — Female Genital Tract Practical Quick-Reference
Use this table as your bench-side reference. For each entity, the examiner expects you to name the gross appearance, the key microscopic feature, and the clinical-diagnostic clue.
| Lesion | Gross | Key Micro Feature | Clinical / Practical Clue |
|---|---|---|---|
| Chronic cervicitis | Reddened, erosive ectocervix; nabothian cysts | Lymphoplasmacytic stroma, squamous metaplasia | Common; nabothian cysts = mucus retention |
| Endometriosis | Chocolate cyst (ovary); powder-burn peritoneum | Endometrial glands + stroma + hemosiderin macrophages | Triad mandatory for diagnosis |
| Simple hyperplasia | Thickened endometrium | Dilated cystic glands, abundant stroma, no atypia | Low malignant risk; exogenous estrogen history |
| Atypical hyperplasia | Polypoid thickening | Crowded glands, nuclear atypia, prominent nucleoli | 25–30% risk carcinoma; precancerous |
| Endometrioid carcinoma | Polypoid fundal mass | Invasive glands, desmoplastic stroma, graded by solid % | Postmenopausal bleeding; Grade 1–3 |
| Leiomyoma | Firm, white, whorled nodule | Uniform spindle cells, intersecting fascicles, no atypia | Most common pelvic tumor; multiple |
| Leiomyosarcoma | Soft, fleshy, hemorrhagic | Atypia + ≥10 mit/10HPF + coagulative necrosis | De novo; not from fibroid |
| Complete mole | Grape-like vesicular villi, no fetus | All hydropic villi, circumferential trophoblastic hyperplasia | Very high hCG; 46,XX androgenetic |
| Partial mole | Focal vesicular + fetal parts | Two villi populations, scalloped villi, trophoblastic inclusions | Triploid 69,XXY; lower hCG |
| Choriocarcinoma | Hemorrhagic, necrotic uterine mass | Biphasic cyto + syncytiotrophoblast; NO villi | Markedly elevated hCG; MTX-curable |
| Serous cystadenoma | Unilocular, smooth, watery | Ciliated single-layer tubal epithelium | Benign; most common benign epithelial |
| HGSC ovary | Solid-cystic, bilateral | Papillary architecture, marked atypia, psammoma bodies | Most lethal; TP53; serous carcinoma |
| Mucinous cystadenoma | Multilocular, gelatinous | Tall columnar cells, basal nuclei, apical mucin | Unilateral; can be massive |
| Mature teratoma | Cyst with hair/sebum/teeth | All 3 germ layers; squamous lining dominant | Most common germ-cell tumor; benign |
| Dysgerminoma | Solid, fleshy, cream | Clear cells in sheets; fibrous septa with lymphocytes | Young women; LDH marker |
| Granulosa cell tumor | Yellow, solid-cystic | Call-Exner bodies; coffee-bean nuclei | Estrogen-secreting; inhibin marker |
| Krukenberg tumor | Bilateral, solid | Signet-ring cells in cellular fibromatous stroma | GI primary (stomach); bilateral metastasis |
CLINICAL PEARL
The bilateral ovary rule: When you see bilateral ovarian tumors, think metastasis first until proven otherwise. Primary ovarian tumors are bilateral in ~70% of high-grade serous carcinomas (and the bilaterality is part of their spread pattern), but a mucinous, signet-ring-cell, or solid bilateral ovarian tumor should trigger a search for a GI primary. The classic exam question pairs bilateral ovarian solid tumors with a gastric history — that is Krukenberg.
SELF-CHECK
On a practical slide you see: an ovarian tumor with polygonal cells arranged in sheets, clear glycogen-rich cytoplasm, centrally placed nuclei with prominent nucleoli, and fibrous septa infiltrated by lymphocytes. The most likely tumor is:
A. Granulosa cell tumor
B. Dysgerminoma
C. High-grade serous carcinoma
D. Krukenberg tumor
Reveal Answer
Answer: B. Dysgerminoma
This is the classic histological description of dysgerminoma — large polygonal cells with clear cytoplasm (glycogen), prominent nuclei, arranged in sheets separated by fibrous septa with a lymphocytic infiltrate. Granulosa cell tumors have Call-Exner bodies and coffee-bean grooved nuclei. High-grade serous carcinoma shows papillary architecture, psammoma bodies, and marked atypia without the lymphocytic septa or clear-cell quality. Krukenberg shows signet-ring cells in a fibromatous stroma.