Page 9 of 23
PA29.4 | Ovarian Tumors — SDL Guide
Learning Objectives
- Classify ovarian tumors by cell of origin using the WHO classification framework
- Describe the etiology, pathogenesis, gross and microscopic pathology of each major tumor category
- Explain the clinical course, spread patterns (transcoelomic seeding, omental caking), and staging of ovarian carcinoma
- Identify key tumor markers (CA-125, AFP, hCG, inhibin) and correlate them with specific tumor types
- Recognize high-yield clinico-pathological features: psammoma bodies, Call-Exner bodies, Schiller-Duval bodies, pseudomyxoma peritonei, Meigs syndrome, Krukenberg tumor, struma ovarii
- Apply risk factor knowledge (BRCA1/2, nulliparity, Lynch syndrome) and protective factors (OCP, breastfeeding, parity) to clinical counselling contexts
- List complications of ovarian tumors: torsion, rupture, ascites, paraneoplastic hypercalcemia
INSTRUCTIONS
Ovarian cancer is the most lethal gynecological malignancy — it kills more women than cervical and uterine cancers combined because 75% of cases present at Stage III or IV, after transcoelomic spread has already seeded the peritoneum. The reason? The ovary sits deep in the pelvis with no early symptom pathway. As a clinician, you will be expected to recognize the subtle features, order the right tumor markers, stage correctly, and counsel patients about hereditary risk. This module unpacks a large and complex topic through the lens of WHO classification by cell of origin — the same framework used in examination questions, pathology reports, and oncology MDT meetings.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 22 (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch. 23 (textbook)
- WHO Classification of Tumours: Female Genital Tumours, 5th ed. (2020) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 54-year-old woman visits her physician for bloating, early satiety, and vague abdominal discomfort for 3 months. She has seen two doctors already — both told her it was IBS. On examination today, there is ascites and a firm, irregular pelvic mass. CT scan reveals a complex adnexal mass with peritoneal deposits and omental thickening. CA-125 is 480 U/mL. She is taken to surgery: the omentum is a solid cake of tumor, both ovaries are replaced by papillary growths with gritty white deposits, and the peritoneum is studded with grey-white nodules. Her surgeon tells her this is Stage IIIC ovarian carcinoma.
The tragedy here is not just clinical — it is pathological. This cancer grew silently for years. The peritoneal spread was not because it was detected late; it was because transcoelomic seeding is the biological default for this tumor. To understand why — and to recognize, classify, and manage ovarian tumors — you need the framework in this module.
WHY THIS MATTERS
Ovarian tumors appear in MBBS examinations, USMLE Step 1 & 2, and postgraduate entrance tests with striking regularity. They test your ability to integrate morphology with markers, clinical features with histological subtypes, and etiology with prognosis. In clinical practice:
- An OBG resident must be able to explain a CA-125 result and what it means for staging
- A general surgeon will encounter Krukenberg tumors during gastric cancer workups
- A physician managing a patient with ascites must consider an ovarian primary
- A family medicine doctor counselling a BRCA1 carrier needs to know surveillance and prophylactic options
NMC competency PA29.4 maps directly to this SDL. Every item in this module — classification, etiology, morphology, spread, complications — is examinable.
RECALL
Before we build new knowledge, anchor to what you already know:
- Embryology of the ovary: the ovary has three cellular components — (1) surface epithelium (modified peritoneum / mesothelium), (2) germ cells (arrive from yolk sac endoderm), and (3) sex cord–stromal cells (from gonadal ridge mesenchyme). This embryological tripartite origin directly maps to the WHO classification of ovarian tumors.
- Normal ovarian histology: you've seen follicles, corpus luteum, granulosa cells, theca cells, and the surface epithelium in your histology practicals.
- Tumor biology basics: you know that tumors can be benign or malignant; that malignant tumors invade and metastasize; and that some tumors produce hormones or markers.
- Peritoneal anatomy: the peritoneum lines the abdominal cavity, and the greater omentum hangs from the stomach like an apron over the bowel — it is the first place ovarian cancer seeds when it spreads.
Hold onto these anchors. The entire WHO classification flows from the first point.
WHO Classification: Overview and Cell of Origin Framework
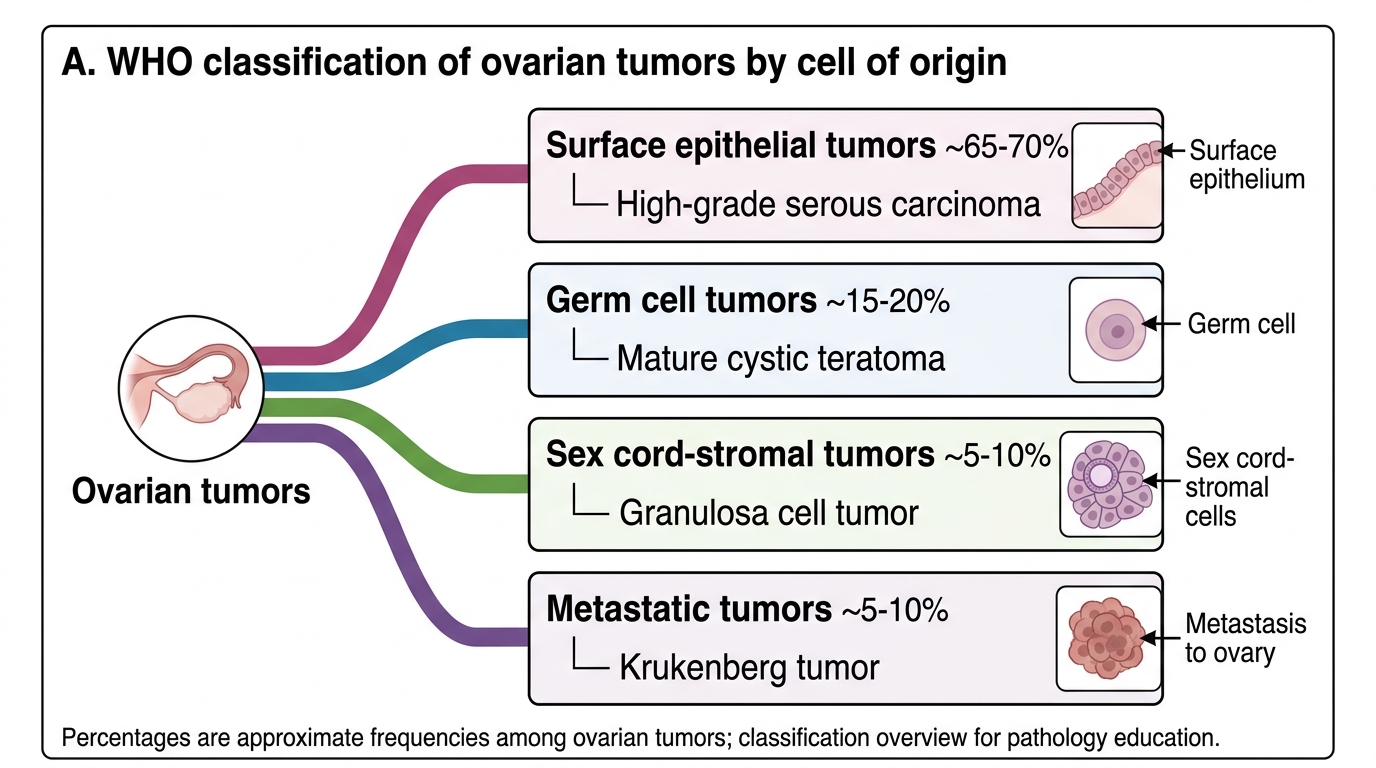
The WHO Classification of Ovarian Tumors is organized by the cell of origin — the most clinically and prognostically useful framework. There are four main categories:
| WHO Category | Cell of Origin | % of Ovarian Tumors | Key Example |
|---|---|---|---|
| Surface epithelial-stromal | Müllerian surface epithelium (peritoneal mesothelium) | ~65–70% | Serous carcinoma |
| Germ cell | Primordial germ cells | ~15–20% | Mature cystic teratoma |
| Sex cord–stromal | Gonadal ridge mesenchyme | ~5–10% | Granulosa cell tumor |
| Metastatic | Secondary deposits from other primaries | ~5% | Krukenberg tumor |
Key principle: epithelial tumors are most common in post-menopausal women; germ cell tumors are most common in young women and girls (peak: 2nd–3rd decade); sex cord–stromal tumors span all ages but often present with hormonal effects.
Within surface epithelial tumors, each type can be benign, borderline (low malignant potential, LMP), or malignant. This three-tier subdivision is unique to the surface epithelial group and is exam-critical.
WHO Classification of Ovarian Tumors by Cell of Origin
Risk Factors and Protective Factors for Ovarian Carcinoma
Understanding risk is essential for counselling and early detection strategies.
High-risk factors:
- BRCA1 mutation: lifetime risk ~39–46% (vs 1.3% population risk). BRCA1 is on chromosome 17q; it encodes a DNA repair protein (homologous recombination). BRCA1-mutated tumors are almost always high-grade serous carcinoma (HGSC).
- BRCA2 mutation: lifetime risk ~10–27%. Chromosome 13q.
- Lynch syndrome (hereditary non-polyposis colorectal cancer, HNPCC): mutations in MMR genes (MLH1, MSH2). Increased risk of endometrioid and clear cell ovarian carcinoma.
- Nulliparity: unopposed incessant ovulation → repeated surface epithelium disruption and repair → accumulation of mutations.
- Early menarche / late menopause: more ovulatory cycles → more surface epithelium repair cycles.
- Endometriosis: direct precursor to clear cell and endometrioid carcinoma ("endometriosis-associated ovarian carcinoma", EAOC).
- HRT (estrogen-only, long-term): modest increased risk.
Protective factors (reduce ovulation cycles):
- Oral contraceptive use: 50% risk reduction with 5 years of use — one of the strongest chemoprevention data points in oncology.
- Multiparity: each pregnancy suppresses ovulation for ~9 months.
- Breastfeeding: suppresses ovulation via prolactin.
- Tubal ligation: possibly blocks ascent of carcinogens from the lower genital tract; recent evidence also suggests the fallopian tube fimbriae are the site of origin for HGSC.
- Prophylactic salpingo-oophorectomy: definitively protective in BRCA carriers (reduces HGSC risk by ~80–96%).
Surface Epithelial Tumors: Serous Tumors
Serous tumors are the most common ovarian epithelial neoplasm and account for the majority of ovarian cancer deaths. The lining cells resemble fallopian tube epithelium (ciliated columnar, secretory).
Serous Cystadenoma (benign):
• Most common benign ovarian tumor
• Usually unilateral, thin-walled, unilocular cyst
• Lining: single layer of ciliated columnar cells (resembles endosalpinx)
• Content: watery, serous fluid (hence the name)
• Often an incidental finding in reproductive-age women
Borderline Serous Tumor (Low Malignant Potential):
• Epithelial stratification and tufting without stromal invasion
• Often bilateral (~30%)
• Can spread to peritoneum as "implants" — but these implants are non-invasive (better prognosis) or rarely invasive (worse prognosis)
• Excellent prognosis: 5-year survival >95% for Stage I–II
High-Grade Serous Carcinoma (HGSC):
• Most common and most lethal ovarian malignancy
• Strongly associated with BRCA1/2 mutations (present in ~15% germline, ~50% somatic BRCA-like alterations)
• TP53 mutation is nearly universal (>96%) — a molecular hallmark
• Newer evidence: many HGSC originate from serous tubal intraepithelial carcinoma (STIC) in the fimbrial end of the fallopian tube, not from ovarian surface epithelium
• Gross: bilateral (~65%), large, solid-cystic masses with papillary excrescences; hemorrhage and necrosis
• Micro: complex papillary or solid architecture; psammoma bodies (concentrically laminated calcified spherules) in ~30% — formed by calcification of papillary tips after ischemic necrosis; marked nuclear atypia; high mitotic index
• Spreads rapidly by transcoelomic seeding to omentum, peritoneum, bowel serosa
• Stage at diagnosis: 75% are Stage III–IV
• Marker: CA-125 (elevated in >80% of cases)
Low-Grade Serous Carcinoma (LGSC):
• Less common (~5% of serous carcinomas)
• KRAS/BRAF mutations (NOT TP53)
• Often arises from borderline tumor
• More indolent but chemoresistant (compared to HGSC which is initially chemo-sensitive)
• Micro: uniform small cells with scant cytoplasm; psammoma bodies common
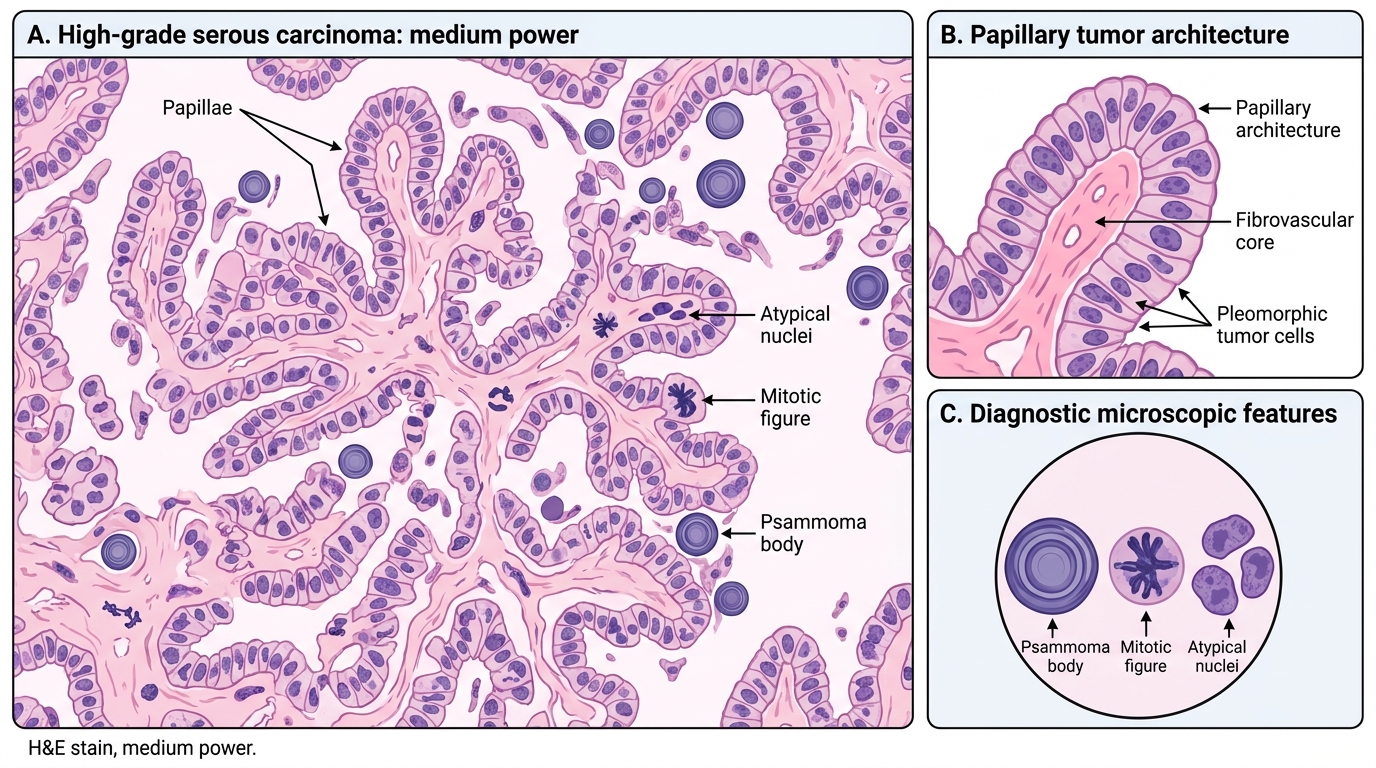
High-Grade Serous Carcinoma of Ovary: Histology
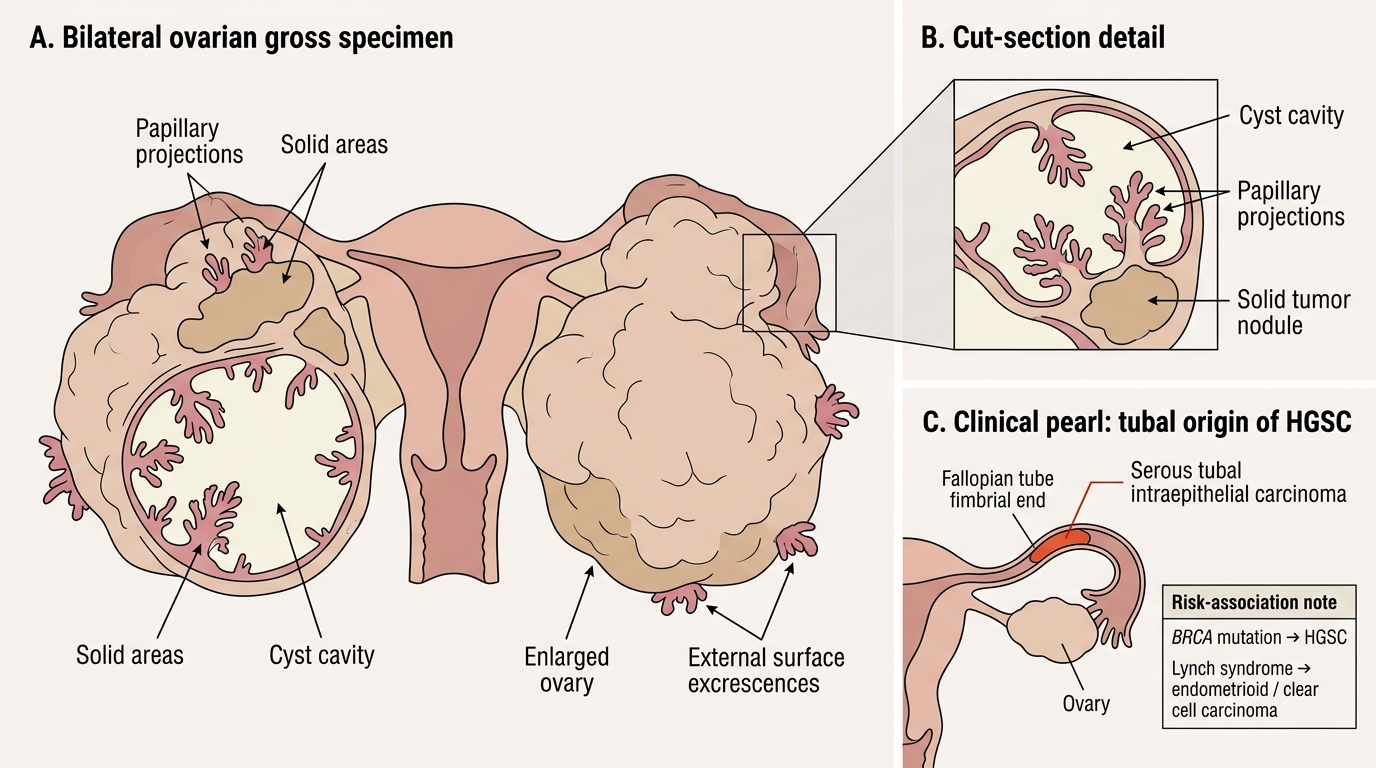
Bilateral Serous Cystadenocarcinoma of Ovaries
CLINICAL PEARL
The fallopian tube origin of HGSC is not just academic trivia — it has changed surgical practice. Prophylactic salpingectomy alone (removing tubes but not ovaries) is now offered to women who want to preserve ovarian function but reduce HGSC risk. This is called "opportunistic salpingectomy" and is recommended at the time of other pelvic surgeries (e.g., hysterectomy, tubal ligation). Remember: BRCA mutation → HGSC; Lynch syndrome → endometrioid/clear cell. This pairing is exam-reliable.