Page 10 of 23
PA29.4 | Ovarian Tumors — SDL Guide (Part 2)
Surface Epithelial Tumors: Mucinous Tumors and Pseudomyxoma Peritonei
Mucinous tumors are lined by mucin-secreting columnar cells resembling endocervical or intestinal epithelium.
Mucinous Cystadenoma (benign):
• Second most common benign ovarian tumor after serous cystadenoma
• Usually unilateral, multiloculated ("honeycomb" appearance), filled with thick viscous mucin
• Can be enormous — reported up to 50 kg!
• Micro: single layer of tall columnar cells with basal nuclei and abundant apical mucin (intestinal or endocervical type)
Borderline Mucinous Tumor:
• Epithelial stratification and mild atypia without stromal invasion
• Two subtypes: intestinal type (common) and endocervical (Müllerian) type
Mucinous Carcinoma (primary ovarian, rare):
• Truly primary ovarian mucinous carcinomas are uncommon — most bilateral mucinous tumors are metastatic (from appendix, colorectum, stomach, pancreas)
• A practical rule: bilateral mucinous ovarian tumor = think metastatic until proven otherwise
Pseudomyxoma Peritonei (PMP):
• A rare but dramatic complication defined as mucin accumulation throughout the peritoneal cavity ("jelly belly")
• Classically associated with a low-grade mucinous neoplasm of the appendix (low-grade appendiceal mucinous neoplasm, LAMN) — the ovary is secondarily involved, not the primary
• Peritoneal cavity fills with gelatinous mucin, causing progressive abdominal distension
• Histologically, the mucin pools may contain sparse, bland epithelial cells
• Prognosis: indolent but incurable with standard chemotherapy; treatment is cytoreductive surgery + HIPEC (hyperthermic intraperitoneal chemotherapy)
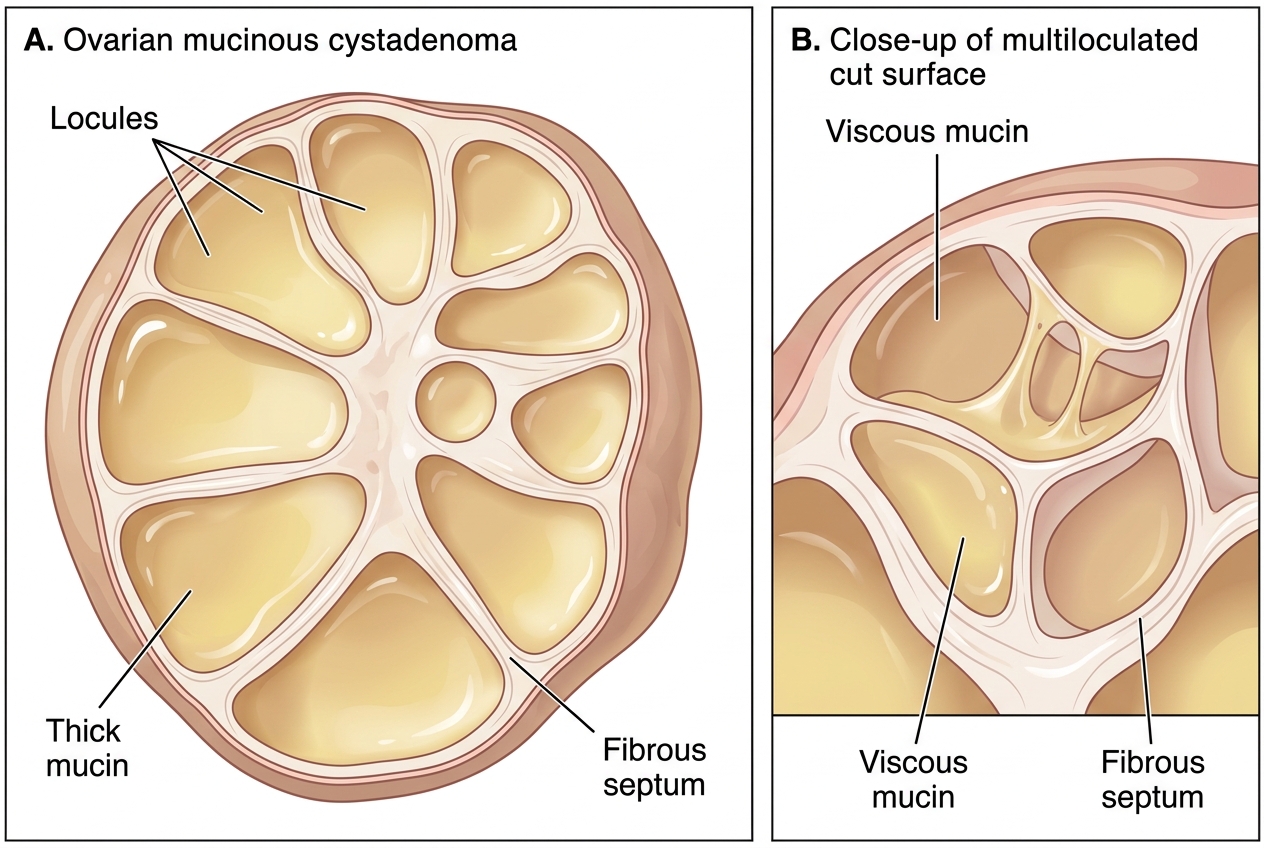
Gross Mucinous Cystadenoma of Ovary
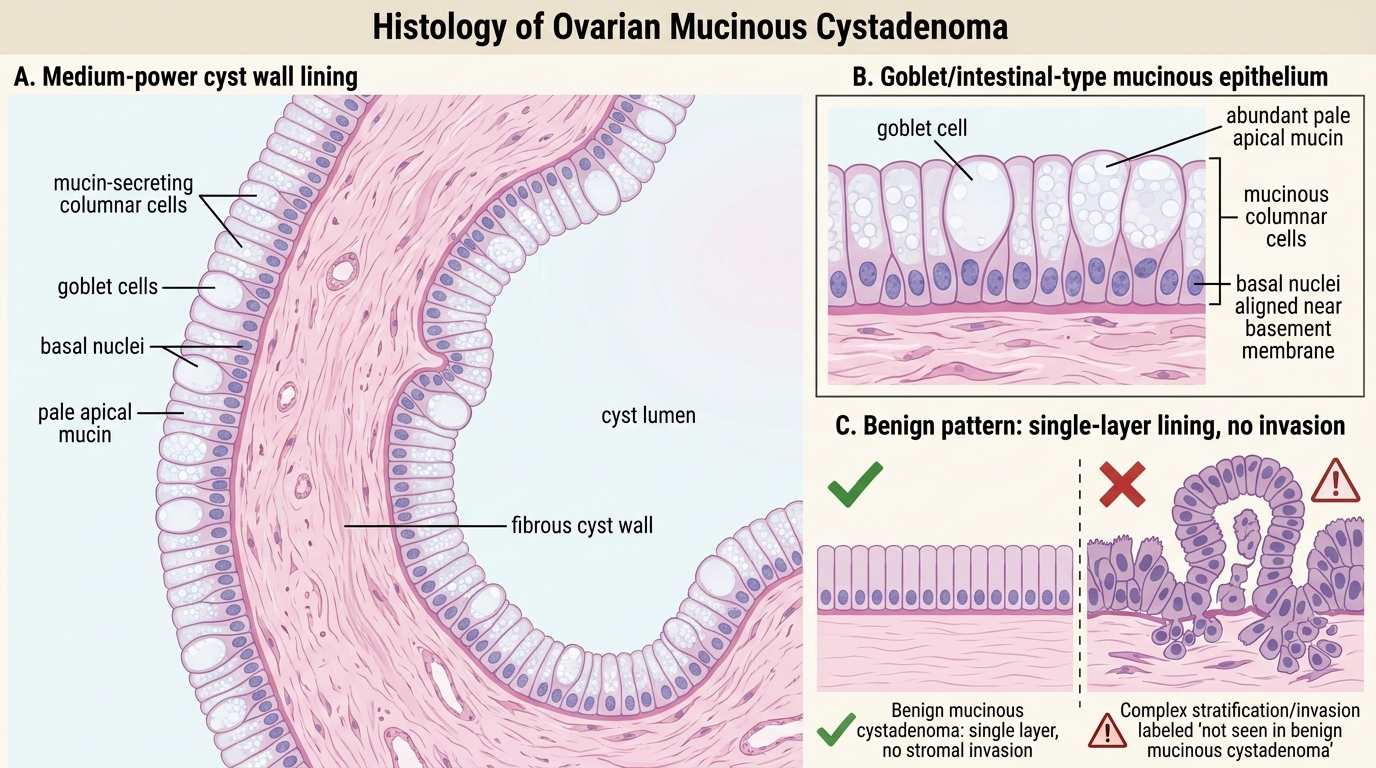
Mucinous Cystadenoma: Histology
Surface Epithelial Tumors: Endometrioid, Clear Cell, and Brenner Tumors
Endometrioid Carcinoma:
• Second most common ovarian carcinoma (~10–20%)
• Histologically resembles endometrial adenocarcinoma: glands lined by stratified columnar epithelium with squamoid differentiation (squamous morules)
• Strongly associated with endometriosis (20–30% arise in an endometriotic cyst — "chocolate cyst") and with synchronous endometrial carcinoma (present in 15–30% of cases — may be independent primary tumors, not metastases)
• Molecular profile: CTNNB1 (β-catenin), PTEN, PIK3CA mutations; microsatellite instability (Lynch syndrome link)
• Prognosis: better than HGSC when diagnosed at early stage
Clear Cell Carcinoma:
• ~5–10% of ovarian carcinomas
• Also strongly associated with endometriosis (EAOC); highest frequency in Japan and East Asia
• Gross: solid-cystic mass, often arising within an endometriotic cyst
• Micro: two distinctive cell types — (1) clear cells: large cells with abundant clear cytoplasm (glycogen-rich, washed out in H&E processing) — (2) hobnail cells: cells with nuclei bulging into the lumen like a hobnail boot
• ARID1A mutation is the molecular hallmark (~50%); also PIK3CA
• Notably chemo-resistant to standard platinum–taxane regimens — a major clinical challenge
• Paraneoplastic hypercalcemia occurs in ~10% (PTHrP secretion)
Brenner Tumor:
• Uncommon; usually benign (>95%)
• Contains nests of transitional epithelium (resembles urothelium / bladder lining) embedded in dense fibrous stroma — "coffee bean" nuclei
• Often an incidental finding; may be associated with mucinous cystadenoma in the same ovary
• Gross: small, firm, white-grey; may be calcified
• Malignant Brenner tumor: rare; aggressive behavior
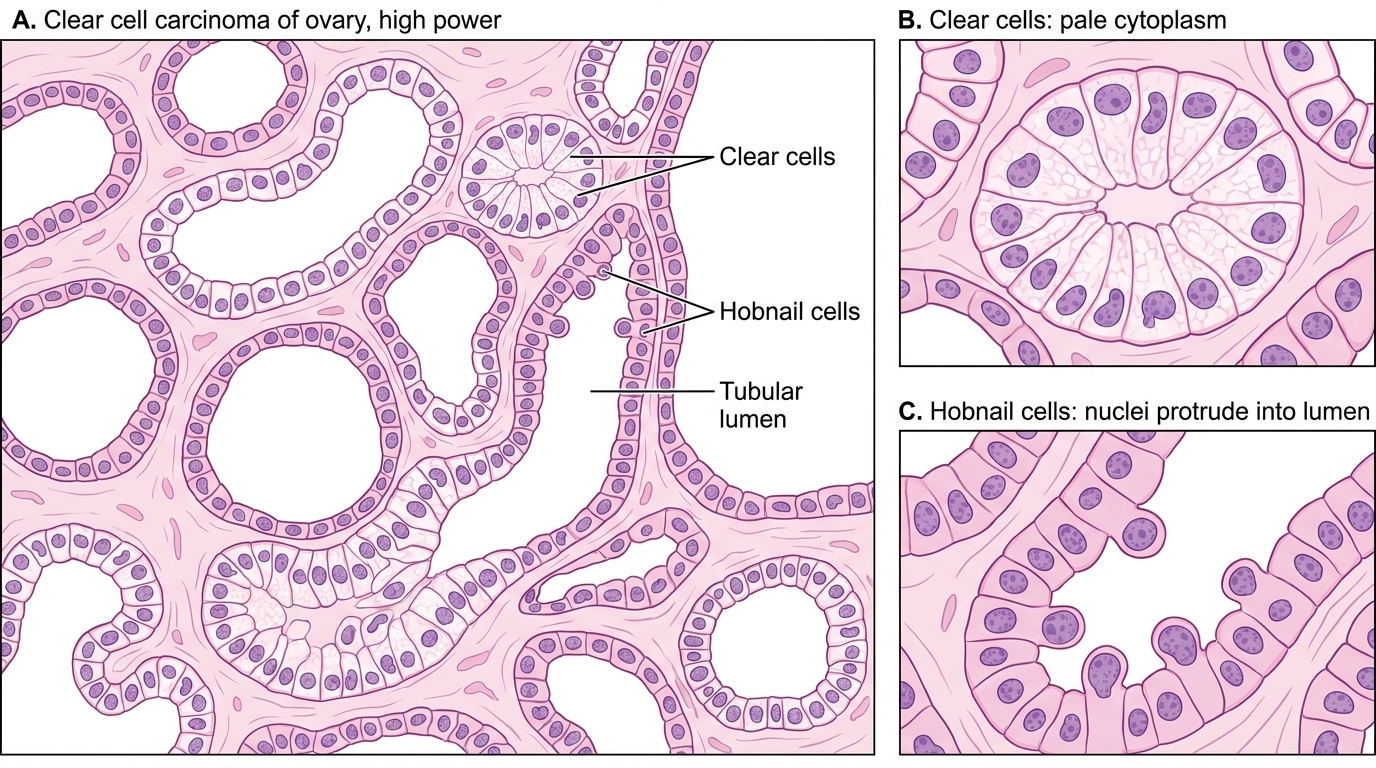
Ovarian Clear Cell Carcinoma: Tubulocystic Pattern
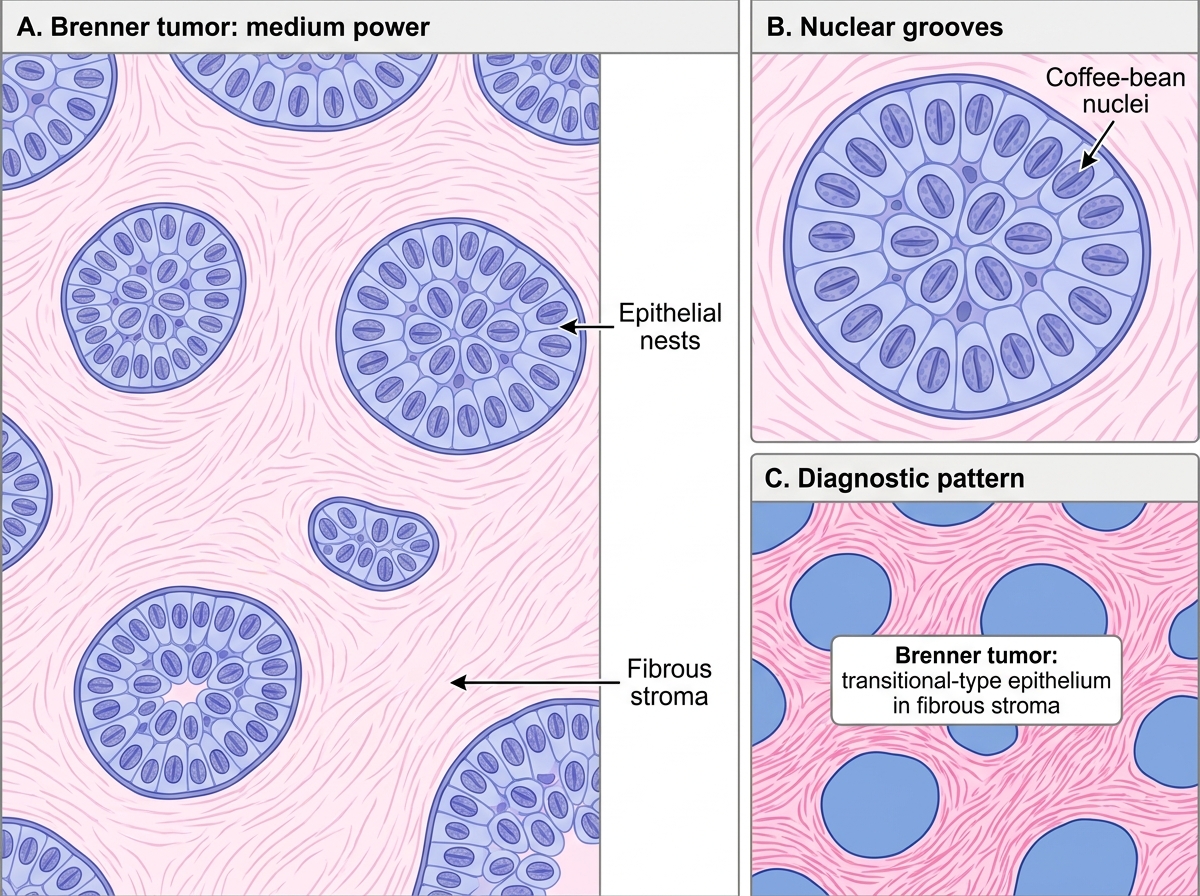
Histology of Brenner Tumor
SELF-CHECK
A 62-year-old woman presents with bilateral adnexal masses, ascites, and CA-125 of 520 U/mL. Histology shows complex papillary architecture with high nuclear grade, frequent mitoses, and gritty calcified spherules within the papillae. BRCA1 germline mutation is confirmed. What are the calcified spherules called, and what is the molecular hallmark of this tumor type?
A. Schiller-Duval bodies; AFP overexpression
B. Psammoma bodies; near-universal TP53 mutation
C. Call-Exner bodies; inhibin secretion
D. Asteroid bodies; KRAS mutation
Reveal Answer
Answer: B. Psammoma bodies; near-universal TP53 mutation
The gritty calcified spherules are psammoma bodies — concentrically laminated calcifications formed at papillary tips — classic for high-grade serous carcinoma (HGSC). HGSC shows near-universal TP53 mutation (>96%) and is strongly associated with BRCA1/2 mutations. Schiller-Duval bodies are found in yolk sac tumor (with AFP). Call-Exner bodies with inhibin characterize granulosa cell tumor. KRAS/BRAF mutations are the hallmark of low-grade serous carcinoma.
Germ Cell Tumors: Mature Cystic Teratoma and Immature Teratoma
Germ cell tumors (GCTs) arise from primordial germ cells and reproduce the developmental potential of the egg — hence, they may contain derivatives of all three germ layers (ectoderm, mesoderm, endoderm). GCTs are the most common ovarian tumors in women under 20.
Mature Cystic Teratoma ("Dermoid Cyst"):
• Most common benign ovarian tumor in reproductive-age women and the most common germ cell tumor overall
• Contains well-differentiated tissues from ≥2 germ layers: most commonly skin (dermis, hair follicles, sebaceous glands — hence "dermoid"), teeth, bone, cartilage, thyroid tissue, neural tissue, respiratory epithelium
• Gross: cyst filled with yellow-grey sebaceous material and hair; may contain teeth visible on X-ray/imaging
• A specific structure: the Rokitansky protuberance (dermoid plug) — a solid nodule projecting into the cyst from which the diverse tissue elements arise
• Micro: all tissues are well-differentiated (mature) — this is the key distinction from immature teratoma
• Usually unilateral; 10–15% bilateral
• Complications: torsion (most common complication; presents as acute abdomen in young women), rupture (chemical peritonitis from sebaceous content), malignant transformation (<1%, usually to squamous cell carcinoma from the skin component)
• Struma ovarii: a monodermal teratoma composed predominantly of thyroid tissue; may cause hyperthyroidism; radioiodine scan shows pelvic uptake
Immature Teratoma:
• Contains immature (embryonic) tissue, especially immature neural tissue (neuroepithelial tubules/rosettes)
• Grading (I–III) based on the proportion of immature neural elements per slide (Grade III = most aggressive)
• Elevated AFP and LDH as markers
• Treatment: surgical + chemotherapy (BEP: bleomycin–etoposide–cisplatin); good prognosis with treatment
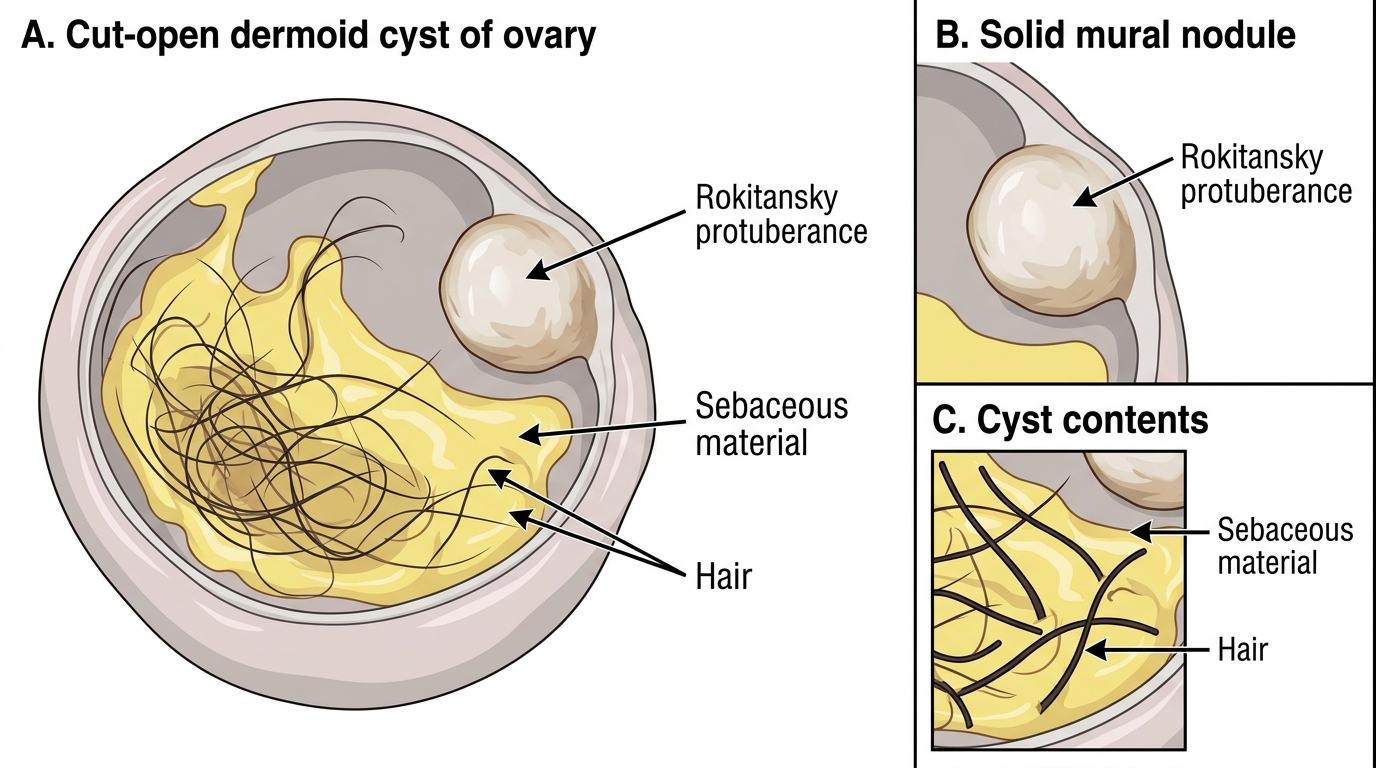
Gross Specimen of Mature Cystic Teratoma of Ovary
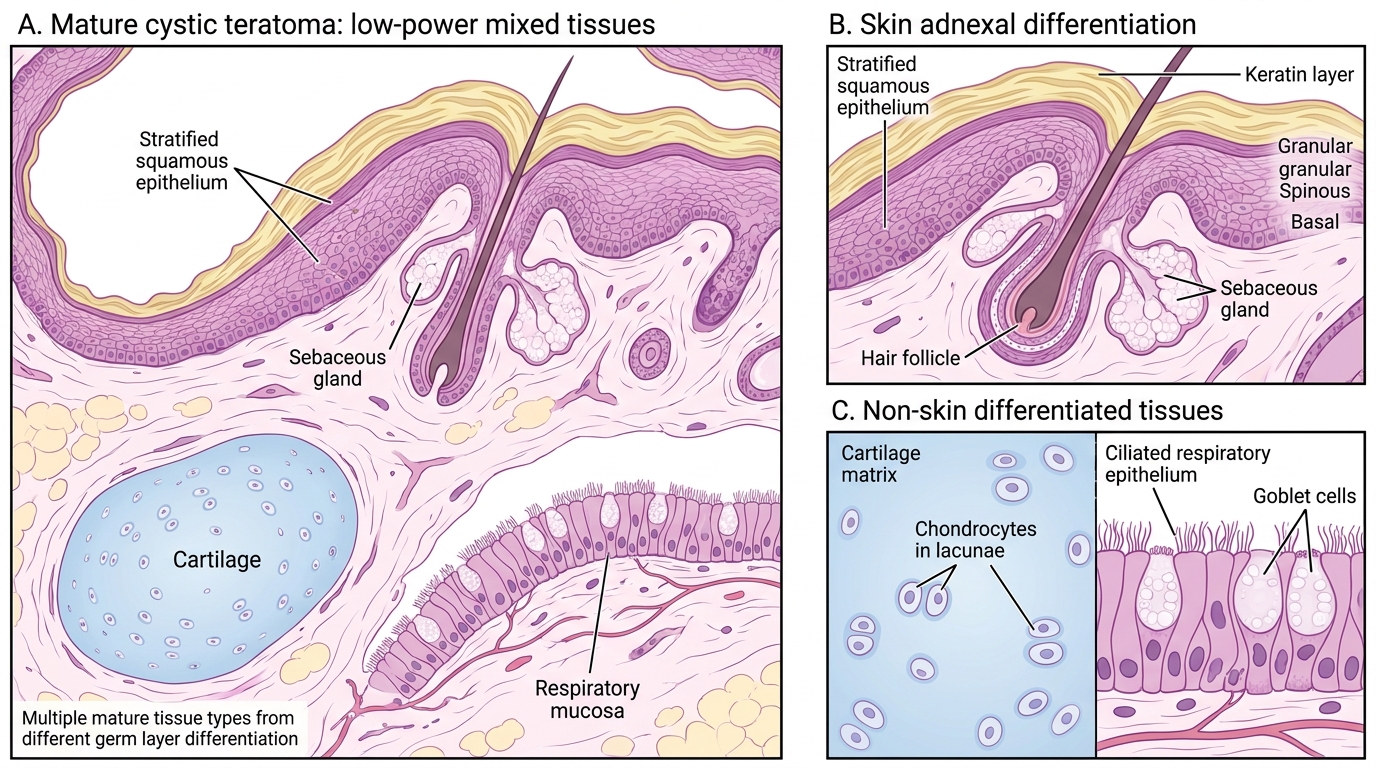
Mature Cystic Teratoma: Mixed Mature Tissues