Page 11 of 23
PA29.4 | Ovarian Tumors — SDL Guide (Part 3)
Germ Cell Tumors: Dysgerminoma, Yolk Sac Tumor, and Choriocarcinoma
Dysgerminoma:
• The most common malignant GCT; counterpart of testicular seminoma in the male
• Peak age: 10–30 years
• 5–10% are bilateral
• Gross: solid, grey-white to tan, lobulated mass; rubbery consistency
• Micro: uniform large cells with clear cytoplasm and central nuclei arranged in sheets and nests, separated by fibrous septae infiltrated by lymphocytes (characteristic lymphocytic stroma); mitoses present but morphology is monotonously uniform
• Marker: placental alkaline phosphatase (PLAP), LDH; hCG may be mildly elevated if syncytiotrophoblastic giant cells are present
• Highly radiosensitive and chemosensitive — excellent prognosis (>95% cure rate with BEP)
• Association: 5% occur in patients with gonadal dysgenesis (e.g., 46,XY pure gonadal dysgenesis — Swyer syndrome)
Yolk Sac Tumor (Endodermal Sinus Tumor):
• Second most common malignant GCT
• Peak age: childhood and early adolescence (median ~19 years)
• Rapidly growing, unilateral, usually large
• Micro: two hallmarks — (1) Schiller-Duval bodies: glomeruloid structures with a central vessel surrounded by tumor cells (resembles the yolk sac glomerulus / rat placental sinus) — (2) eosinophilic hyaline globules containing PAS-positive material (AFP)
• Marker: AFP (alpha-fetoprotein) — dramatically elevated; used for diagnosis and monitoring response to treatment
• Treatment: BEP chemotherapy; prognosis depends on stage
Ovarian Choriocarcinoma (Non-gestational):
• Extremely rare; may occur in pure form or as a component of mixed GCT
• Micro: biphasic pattern of cytotrophoblasts (mononuclear, pale) and syncytiotrophoblasts (large, multinucleated, dark, with lacunae)
• Marker: beta-hCG — extremely elevated; causes isosexual pseudoprecocity in pre-pubertal girls
• Highly aggressive; often presents with metastases
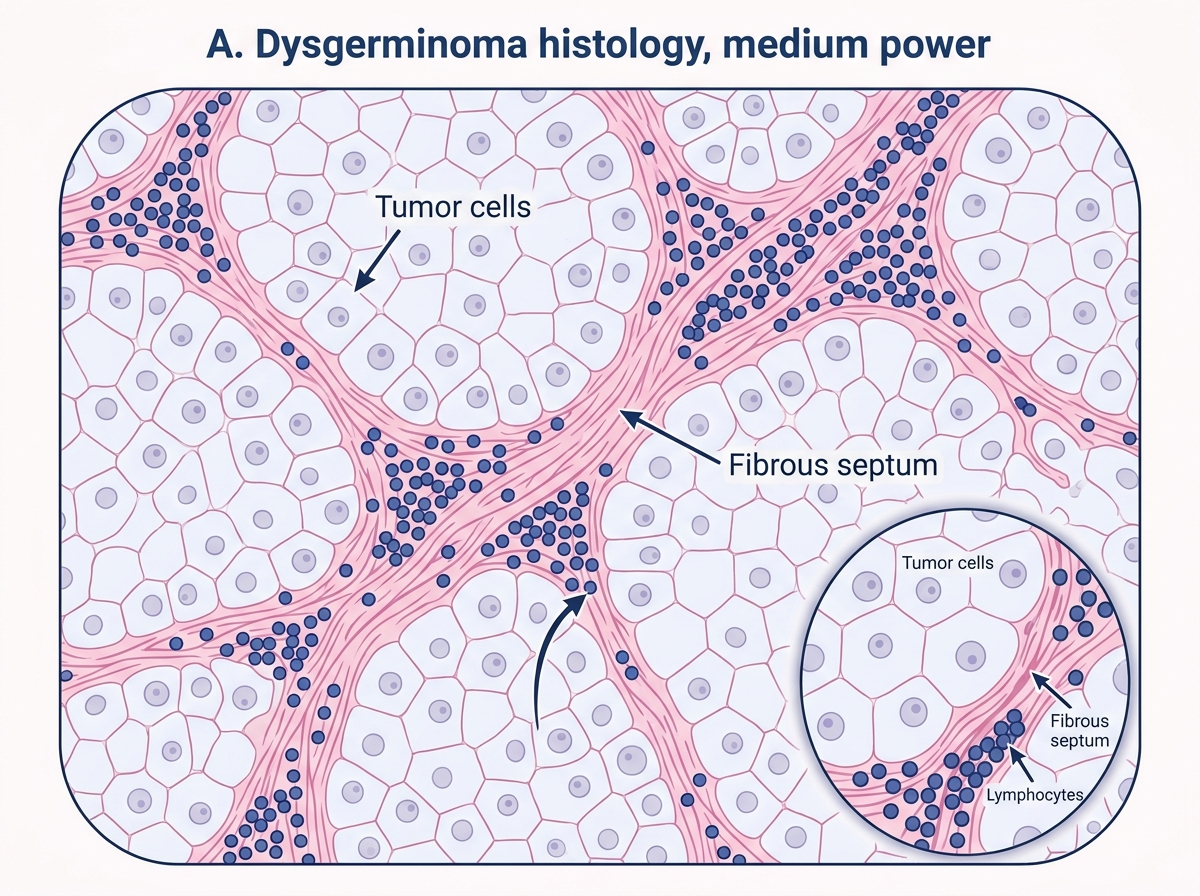
Histology of Dysgerminoma
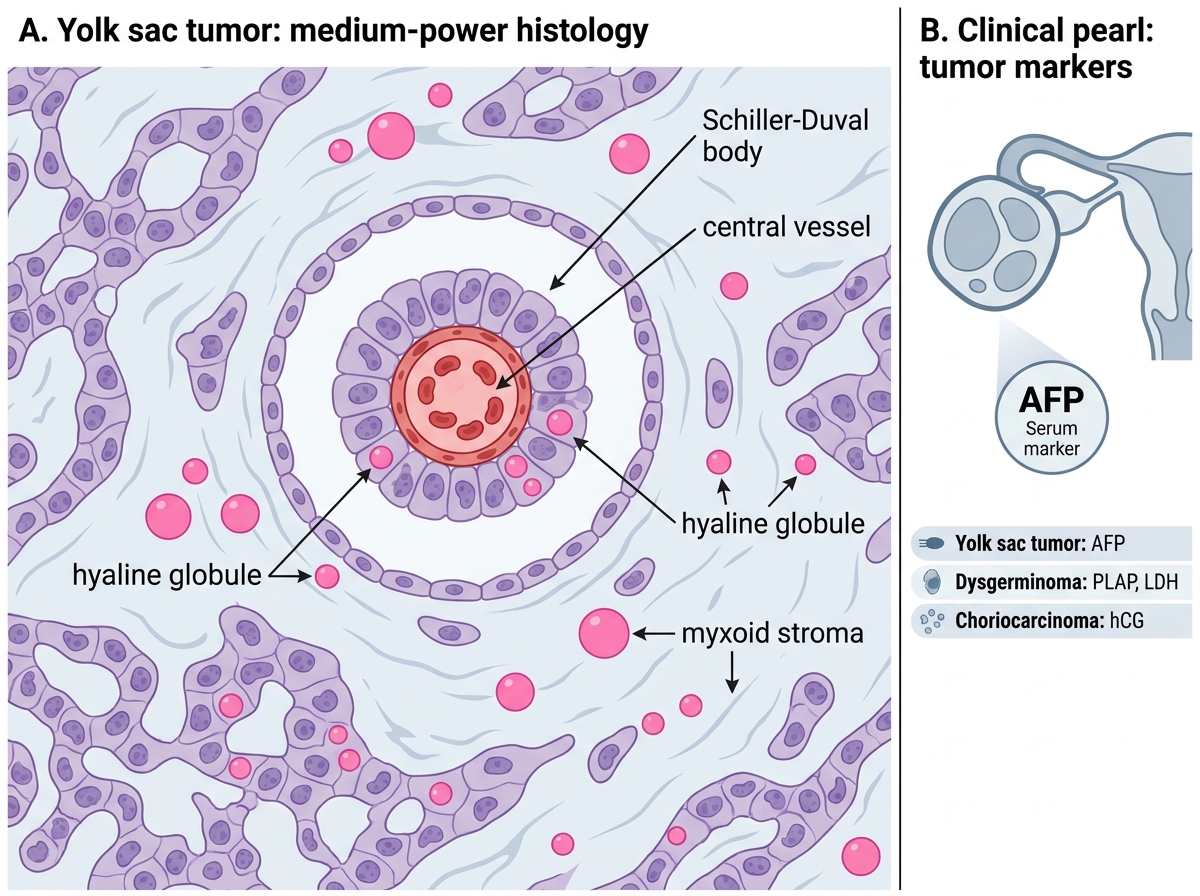
Yolk Sac Tumor Histology: Schiller-Duval Body
CLINICAL PEARL
AFP is the tumor marker for yolk sac tumor — not for dysgerminoma. Many students confuse the two. A memory trick: Yolk sac → AFP (Y and A are alphabetically adjacent; yolk sac = AFP). Dysgerminoma uses PLAP and LDH. Choriocarcinoma uses hCG. These pairings are directly examinable. In clinical practice, a 15-year-old girl with a large rapidly growing ovarian mass and AFP of 1,200 ng/mL should be presumed to have yolk sac tumor until proven otherwise — this is a surgical and oncological emergency.
Sex Cord–Stromal Tumors: Granulosa Cell Tumor and Thecoma-Fibroma
Sex cord–stromal tumors arise from the gonadal ridge mesenchyme and recapitulate the supporting cells of the ovarian follicle. They are functionally active — producing estrogen or androgen — and their hormonal effects are clinically distinctive.
Granulosa Cell Tumor (GCT):
• Most important malignant sex cord–stromal tumor
• Two types:
1. Adult type (95%): peak age 50–55 years (peri/post-menopausal)
2. Juvenile type (5%): children/young women; different histology and behavior
- Functional: produces estrogen → causes endometrial hyperplasia (and risk of endometrial carcinoma in ~5%), breast tenderness, pseudo-precocious puberty in girls, irregular uterine bleeding
- Gross: typically unilateral, well-encapsulated, solid-cystic; yellow-grey cut surface with areas of hemorrhage (bloody cysts due to hormonal corpus-luteum-like tissue)
- Micro: three characteristic patterns:
- Call-Exner bodies: small follicle-like structures with central pink amorphous material (resembling primitive follicles) — pathognomonic
- Microfollicular, macrofollicular, trabecular, insular patterns
- Cells have "coffee-bean" nuclear grooves (longitudinal nuclear groove) — like Brenner but in a different context
- Marker: inhibin (most sensitive and specific), AMH (anti-Müllerian hormone), estradiol
- Molecular: FOXL2 mutation (C134W) in >95% of adult GCT — highly specific
- Behavior: low-grade malignancy; recurrences may occur decades after initial treatment ("Sleeping Beauty" tumor); late recurrence is the rule, not the exception
Thecoma:
• Benign; composed of lipid-filled theca cells; produces estrogen
• Gross: solid, yellow (due to lipid); unilateral
• Micro: sheets of spindle cells with pale lipid-filled cytoplasm and Reinke crystals may be present
Fibroma:
• Most common sex cord–stromal tumor; benign; composed of fibroblasts/collagen; hormonally inert
• Associated with Meigs syndrome: ovarian fibroma + ascites + right-sided pleural effusion — all resolve after tumor resection (mechanism: fluid transudation from tumor surface → peritoneal → pleural via diaphragmatic lymphatics)
• Also associated with Gorlin syndrome (basal cell nevus syndrome): multiple fibromas + calcifying odontogenic keratocysts + basal cell carcinoma
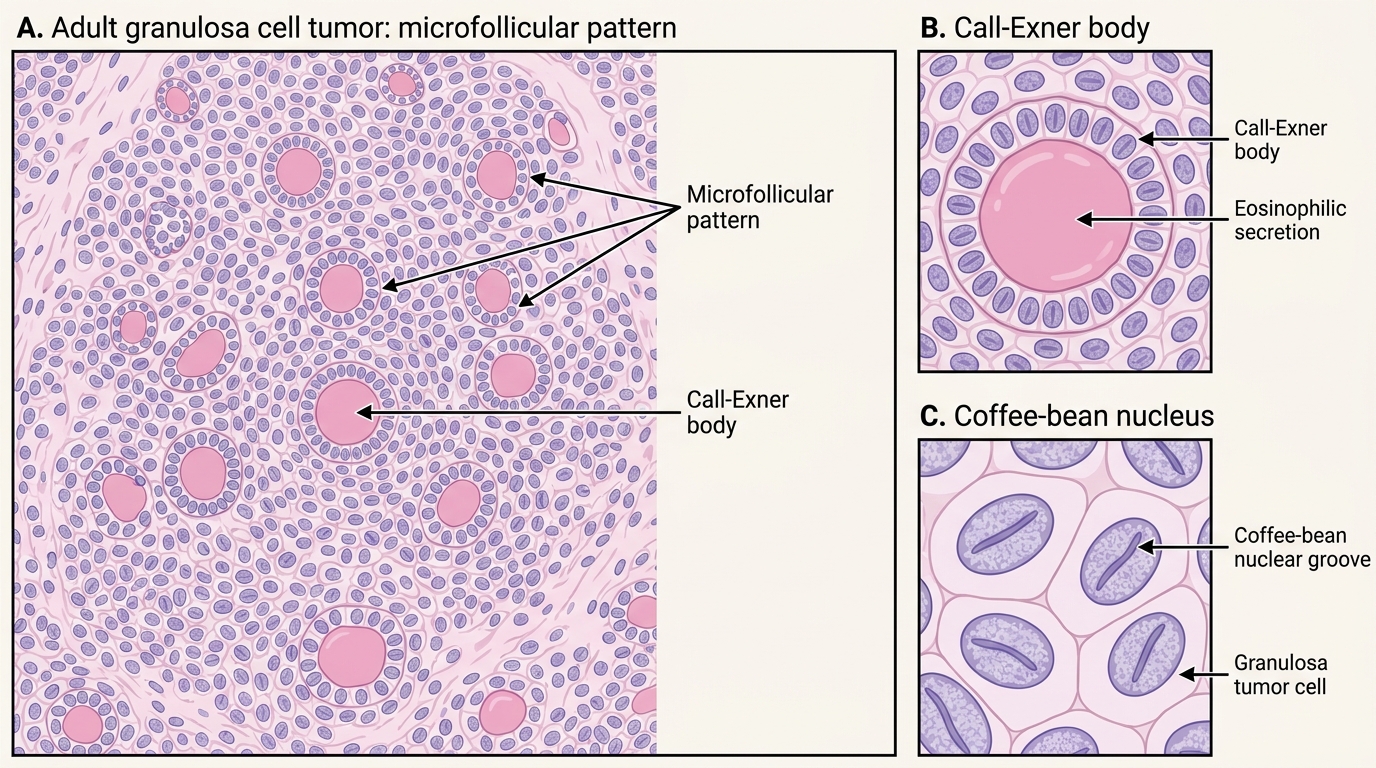
Adult Granulosa Cell Tumor: Histology
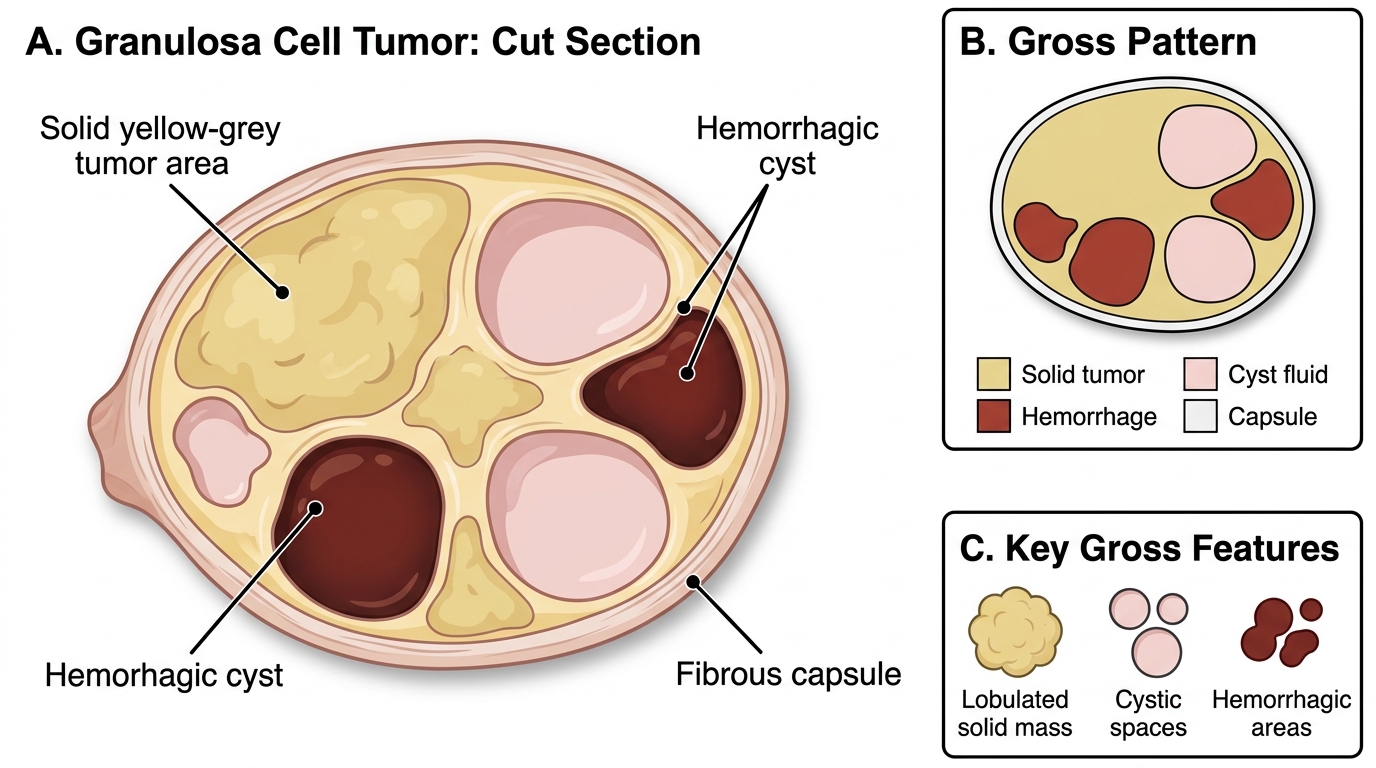
Gross Cut Section of Granulosa Cell Tumor
Sex Cord–Stromal Tumors: Sertoli-Leydig Cell Tumor (Androblastoma)
Sertoli-Leydig cell tumor (also called androblastoma) is a rare sex cord–stromal tumor that recapitulates the testicular cellular architecture — Sertoli cells (sex cord component) + Leydig cells (stromal component).
Clinical features:
• Peak age: 20–30 years
• Produces androgens (testosterone, DHEA-S) → virilization: hirsutism, acne, clitoromegaly, deepening of voice, temporal balding, cessation of menses
• Sequence: defeminization (loss of female secondary sex characteristics) precedes masculinization
• Unilateral in >95%; usually low-grade malignant potential
Gross: solid, lobulated, grey-white to yellow; small (usually <15 cm)
Micro:
• Well-differentiated: hollow tubules lined by Sertoli cells; Leydig cells (polygonal, eosinophilic, with Reinke crystals — rod-shaped cytoplasmic inclusions pathognomonic of Leydig cells) between the tubules
• Moderately differentiated: cords and nests of Sertoli cells without lumina; Leydig cells in clusters
• Poorly differentiated: sarcomatoid pattern; worse prognosis
• Heterologous elements (mucinous glands, cartilage) in ~20%
Markers: inhibin, testosterone, androstenedione
Treatment: surgical (unilateral oophorectomy in young women who desire fertility); BEP chemotherapy for malignant variants
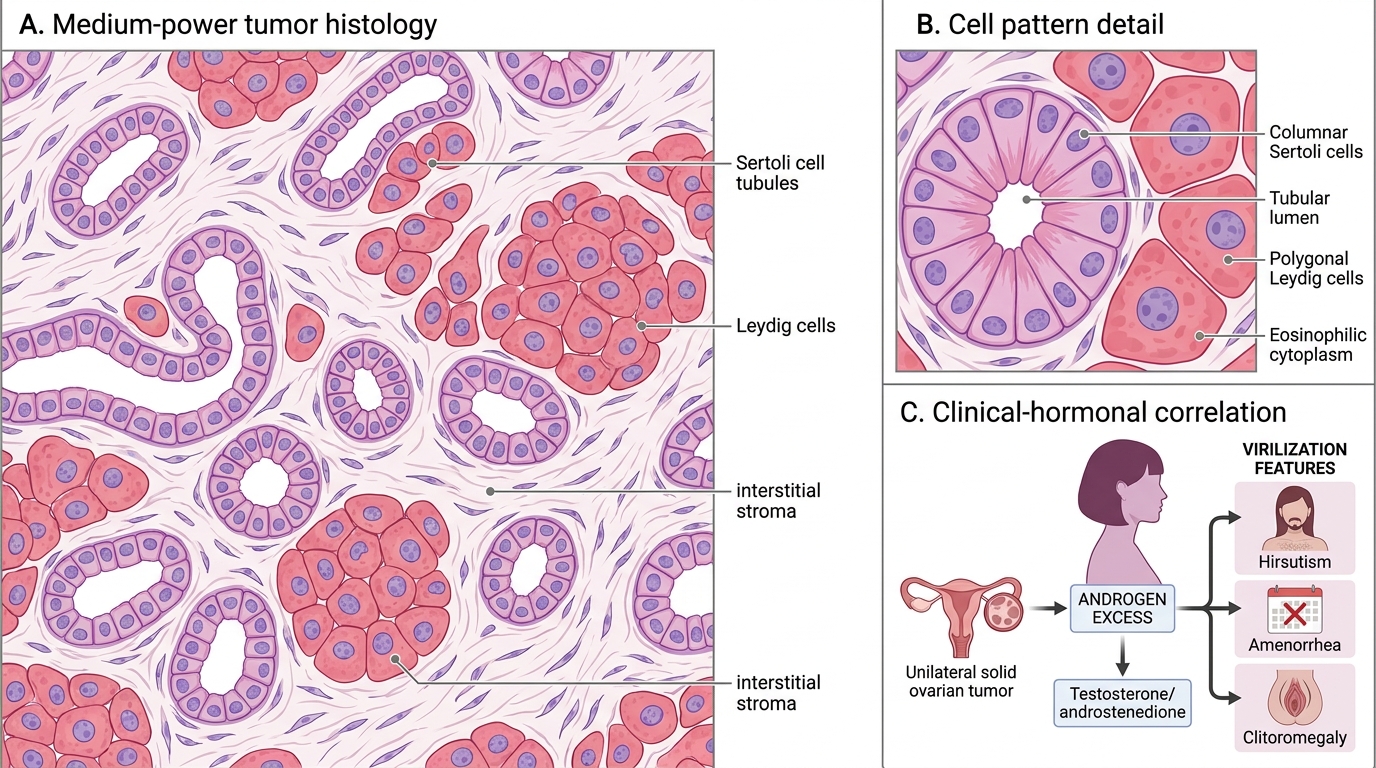
Sertoli-Leydig Cell Tumor: Histology and Androgenic Presentation
SELF-CHECK
A 28-year-old woman presents with hirsutism, amenorrhea, and clitoromegaly of 6 months duration. Pelvic ultrasound reveals a 7 cm solid, unilateral ovarian mass. Testosterone is markedly elevated. The most likely diagnosis and its characteristic hormonal marker are:
A. Granulosa cell tumor; inhibin
B. Thecoma; estradiol
C. Sertoli-Leydig cell tumor; testosterone/androstenedione
D. Dysgerminoma; PLAP and LDH
Reveal Answer
Answer: C. Sertoli-Leydig cell tumor; testosterone/androstenedione
The clinical triad of virilization (hirsutism, clitoromegaly, amenorrhea) + solid unilateral ovarian mass + markedly elevated testosterone in a young woman is the classic presentation of Sertoli-Leydig cell tumor (androblastoma). It produces androgens. Granulosa cell tumor produces estrogen and is associated with endometrial hyperplasia, feminizing effects, and inhibin as its marker. Thecoma produces estrogen, and dysgerminoma is non-functional but associated with PLAP/LDH.