Page 12 of 23
PA29.4 | Ovarian Tumors — SDL Guide (Part 4)
Metastatic Tumors to the Ovary: Krukenberg Tumor
The ovary is a common site of metastasis from carcinomas of the gastrointestinal tract, breast, and other sites. Metastatic tumors account for ~5% of ovarian tumors and are frequently bilateral (versus most primary ovarian tumors which are unilateral).
Krukenberg Tumor:
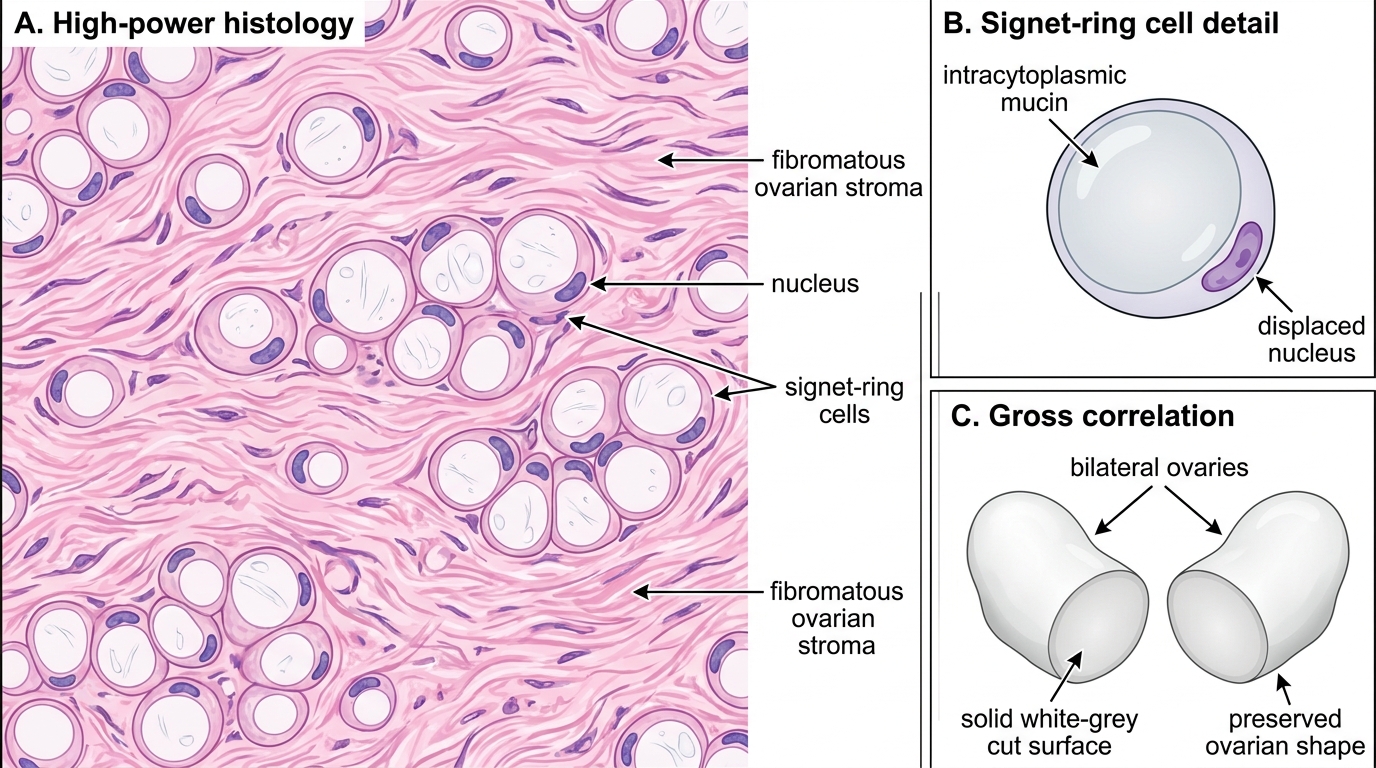
• Defined specifically as bilateral metastatic signet-ring cell carcinoma of the ovary
• Origin: classically from gastric adenocarcinoma (diffuse type, poorly cohesive); also from colorectal, appendiceal, breast, and biliary carcinomas
• Mechanism of spread: hematogenous (blood-borne), lymphatic, or transcoelomic; the bilateral nature and ovarian tropism suggest hormonal or surface receptor-mediated implantation
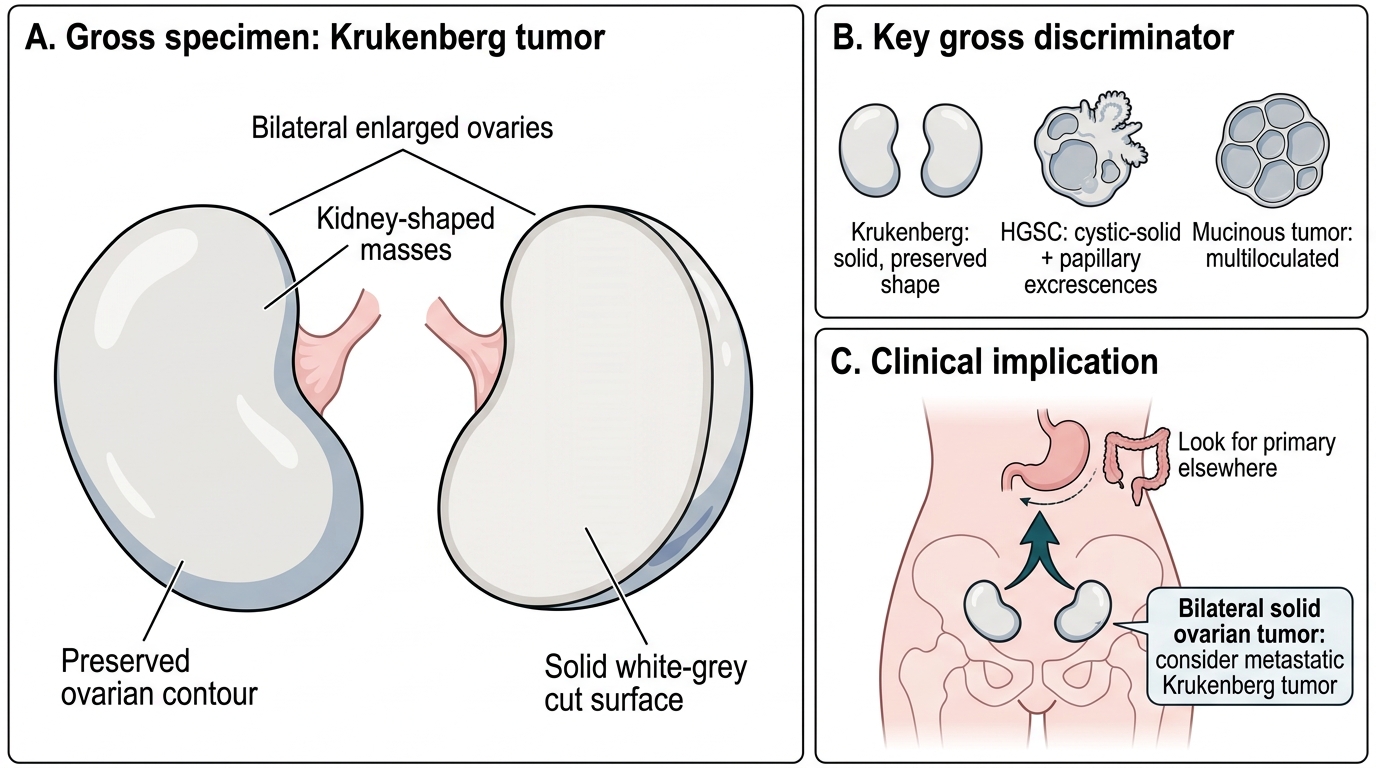
• Gross: bilateral, solid (not cystic), preserved ovarian shape ("kidney-shaped"), firm white-grey masses
• Micro: signet-ring cells — mucin-filled cells that displace the nucleus to the periphery, creating a crescent ("signet ring") appearance — embedded in a cellular edematous fibromatous stroma (reactive stroma derived from ovarian stroma, not desmoplasia)
• Marker: positive for mucin stains (PAS, Alcian blue); CK20+, CDX2+, CK7± (gastric primary); negative for ovarian markers (WT1, PAX8)
Clinical importance:
• A woman presenting with bilateral ovarian masses must be worked up for a GI primary before assuming a primary ovarian tumor
• Prognosis: very poor (reflects the metastatic gastric primary)
Other common metastatic tumors to the ovary:
• Colorectal carcinoma: CK20+, CDX2+, CK7−; "garland pattern" glands with dirty necrosis
• Breast carcinoma: lobular type most common (discohesive cells mimicking signet rings); ER+, GATA3+
• Appendiceal mucinous neoplasm → pseudomyxoma peritonei (discussed under mucinous tumors)
Krukenberg Tumor: Signet-Ring Cells in Fibromatous Ovarian Stroma
Gross Specimen of Krukenberg Tumor
CLINICAL PEARL
Bilateral ovarian tumor = Krukenberg until proven otherwise is an examination mantra — but it requires nuance. Bilateral ovarian tumors can be: (1) bilateral primary (HGSC is bilateral in 65%; borderline serous ~30%; dysgerminoma 5–10%), OR (2) bilateral metastatic (Krukenberg, colorectal, breast). The key discriminators: Krukenberg tumors are solid and preserve ovarian shape; HGSC is cystic-solid with papillary excrescences; mucinous tumors are multiloculated. Always look for a primary elsewhere when bilateral solid ovarian masses are found.
Spread, Staging, and Clinical Features of Ovarian Carcinoma
Routes of spread (most important for pathological and clinical staging):
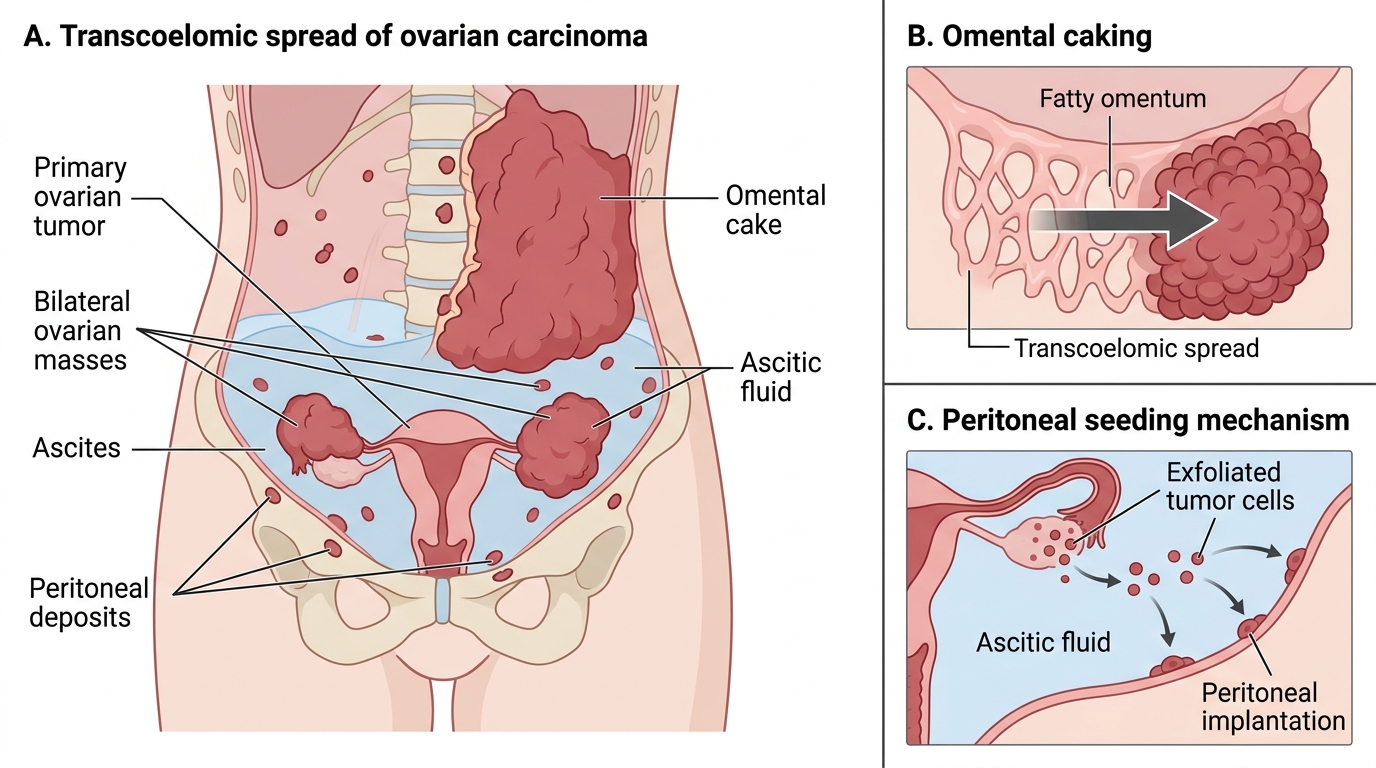
1. Transcoelomic (transperitoneal) seeding — the dominant and most important route
• Malignant cells shed from the ovarian surface into the peritoneal cavity
• Circulate via peritoneal fluid
• Implant preferentially on: omentum ("omental caking" — solid replacement of the greater omentum by tumor), peritoneum, bowel serosa, diaphragm (especially right hemidiaphragm), paracolic gutters, pouch of Douglas
• Ascites develops from obstruction of lymphatic drainage and tumor fluid secretion
- Lymphatic spread: to para-aortic nodes (via gonadal lymphatics) and pelvic nodes
- Direct extension: to fallopian tube, uterus, broad ligament
- Hematogenous spread: late; to liver parenchyma, lung (liver surface deposits = transcoelomic, not blood-borne)
FIGO Staging (simplified):
| Stage | Description |
|---|---|
| I | Confined to ovary/ovaries |
| Ia | One ovary, intact capsule, no surface tumor |
| Ib | Both ovaries, intact capsule |
| Ic | Ia/Ib + capsule rupture or surface tumor or positive peritoneal cytology |
| II | Pelvic extension (uterus, tubes, other pelvic organs) |
| III | Peritoneal/omental metastasis beyond pelvis, or retroperitoneal lymph nodes |
| IIIc | Peritoneal metastases >2 cm; or pelvic/para-aortic nodes |
| IV | Distant metastasis (pleural effusion with positive cytology; liver/spleen parenchyma) |
Why 75% present at Stage III–IV:
• The ovary is intraperitoneal — shed cells immediately encounter the peritoneal surface
• Early disease is asymptomatic; by the time symptoms appear (bloating, early satiety, pelvic pressure, altered bowel habits), transcoelomic spread has usually occurred
• Screening with CA-125 + transvaginal ultrasound has NOT proven mortality benefit in general population (UKCTOCS trial, 2016)
Tumor Markers — Summary Table:
| Marker | Primary Tumor |
|---|---|
| CA-125 | Serous carcinoma (>80%); also endometrioid, clear cell |
| AFP (alpha-fetoprotein) | Yolk sac tumor; immature teratoma (component) |
| hCG (beta) | Choriocarcinoma; dysgerminoma (if syncytiotrophoblastic cells) |
| Inhibin | Granulosa cell tumor; thecoma |
| PLAP + LDH | Dysgerminoma |
| CEA / CA19-9 | Mucinous carcinoma; metastatic GI tumor |
Transcoelomic Spread of Ovarian Carcinoma
Complications of Ovarian Tumors
Ovarian tumors — benign or malignant — can produce several acute and chronic complications that require rapid recognition.
1. Torsion (Ovarian Torsion):
• Most common complication of benign cystic tumors, particularly mature cystic teratoma and paraovarian cysts
• The ovarian pedicle (containing ovarian vessels and fallopian tube) twists, causing venous congestion → arterial compromise → ischemia → infarction
• Clinical: sudden onset severe lower abdominal pain, often with nausea/vomiting, in a reproductive-age woman
• Ultrasound: absent Doppler flow to the ovary
• Treatment: surgical untwisting (detorsion) ± oophorectomy; can recur if underlying tumor not removed
2. Rupture:
• Dermoid cysts: rupture releases sebaceous material → chemical (granulomatous) peritonitis with severe pain
• Serous cystadenoma: rupture releases watery fluid — less inflammatory
• Malignant tumors: rupture upstages the tumor from Ia to Ic (FIGO)
3. Ascites:
• Malignant tumors: from transcoelomic seeding → lymphatic obstruction + tumor fluid secretion
• Meigs syndrome: benign ovarian fibroma with ascites + pleural effusion (resolves with tumor removal)
• Pseudo-Meigs syndrome: any benign pelvic tumor (not just fibroma) with ascites + pleural effusion
4. Infection (Dermoid cyst):
• Secondary infection of dermoid cysts → abscess; rare
5. Malignant transformation:
• Mature teratoma → squamous cell carcinoma (<1%)
• Borderline tumor → invasive carcinoma (rare; years later)
6. Paraneoplastic syndromes:
• Hypercalcemia: clear cell carcinoma (PTHrP), immature teratoma
• Subacute cerebellar degeneration: anti-Yo antibodies in HGSC (paraneoplastic neurological syndrome)
• Endometrial hyperplasia/carcinoma: from estrogen secretion by granulosa cell tumor / thecoma
7. Hormonal effects:
• Virilization: Sertoli-Leydig cell tumor, Leydig cell tumor
• Pseudo-precocious puberty in girls: granulosa cell tumor (juvenile type), choriocarcinoma (hCG)
• Isosexual pseudo-precocity: hCG-secreting tumors
SELF-CHECK
A 16-year-old girl presents with rapidly progressive abdominal distension and pain. Ultrasound shows a 12 cm solid unilateral right ovarian mass. Serum AFP is 2,400 ng/mL. Histology of the resected tumor shows glomeruloid vascular structures surrounded by tumor cells within a myxoid stroma, and eosinophilic hyaline globules. Which structure is pathognomonic of this tumor?
A. Psammoma body
B. Call-Exner body
C. Schiller-Duval body
D. Rokitansky protuberance
Reveal Answer
Answer: C. Schiller-Duval body
The described structure — a glomeruloid vascular tuft surrounded by tumor cells in a loose myxoid stroma — is a Schiller-Duval body, pathognomonic of yolk sac tumor (endodermal sinus tumor). The dramatically elevated AFP confirms the diagnosis. Psammoma bodies are concentric laminated calcifications in serous carcinoma. Call-Exner bodies are small follicle-like spaces in granulosa cell tumor. The Rokitansky protuberance is the solid nodule within a mature cystic teratoma (dermoid cyst).
Prognosis and an Integrated Approach to Ovarian Tumors
Prognostic factors for ovarian carcinoma:
| Factor | Better Prognosis | Worse Prognosis |
|---|---|---|
| Stage | I–II | III–IV |
| Histological type | Endometrioid, clear cell (Stage I) | HGSC (usually late stage) |
| Residual disease | <1 cm (optimal cytoreduction) | >1 cm (suboptimal) |
| BRCA mutation | Better chemosensitivity (paradox) | Wild-type TP53 pathway |
| Differentiation | Well-differentiated | Poorly differentiated |
| Ascites volume | Absent/small | Large |
5-year survival by stage (HGSC):
• Stage I: ~90–92%
• Stage II: ~70–75%
• Stage III: ~25–35%
• Stage IV: ~15%
BRCA paradox in treatment: Although BRCA1/2 mutations increase cancer risk, once HGSC develops in a BRCA carrier, it is paradoxically more chemosensitive (platinum–taxane) because BRCA-deficient cells cannot repair platinum-induced DNA crosslinks. PARP inhibitors (olaparib, niraparib) exploit this "BRCAness" as maintenance therapy.
Integrated diagnostic approach — when you see an ovarian mass:
- Bilaterality → suggests epithelial (HGSC), Krukenberg, or borderline serous; not mature teratoma or sex cord–stromal
- Age → young = germ cell; peri/post-menopausal = epithelial or GCT adult type
- Hormonal features → virilization (Sertoli-Leydig), feminization/endometrial hyperplasia (granulosa cell, thecoma)
- Marker → AFP (yolk sac), CA-125 (serous), inhibin (GCT), hCG (choriocarcinoma), PLAP (dysgerminoma)
- Morphology → cystic + hair/teeth (dermoid), bilateral papillary-cystic (serous), solid kidney-shaped (Krukenberg), multiloculated mucinous (mucinous cystadenoma)
- Spread pattern → transcoelomic = malignant epithelial; no spread = benign; lymphatic = advanced malignant
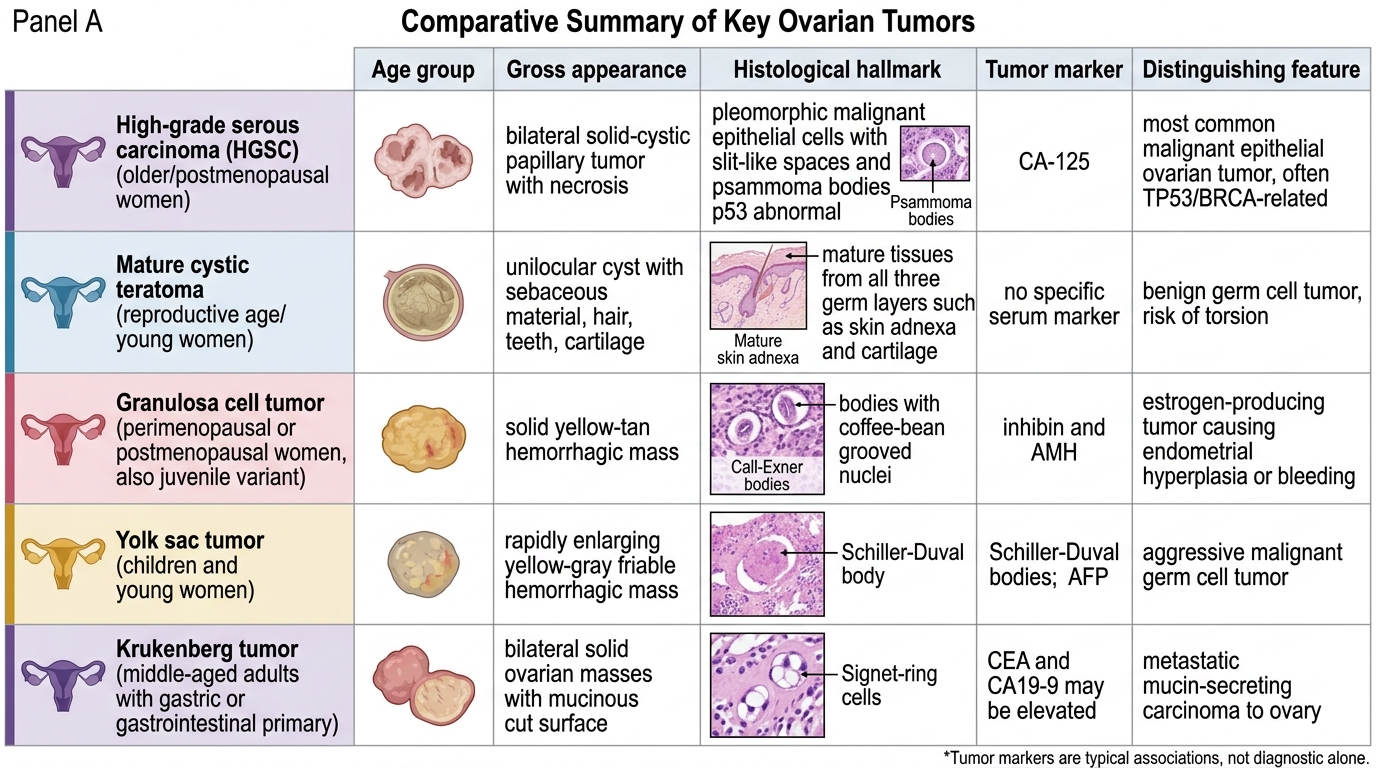
Comparative Summary of Key Ovarian Tumors