Page 7 of 24
PA2.4-5 | Cell Death — Necrosis, Apoptosis, Gangrene & Calcification — SDL Guide (Part 3)
Necroptosis and Pyroptosis — Emerging Cell Death Modes
Necroptosis and Pyroptosis: Inflammatory Programmed Cell Death
Two additional death programmes have clinical relevance in Year-2 pathology:
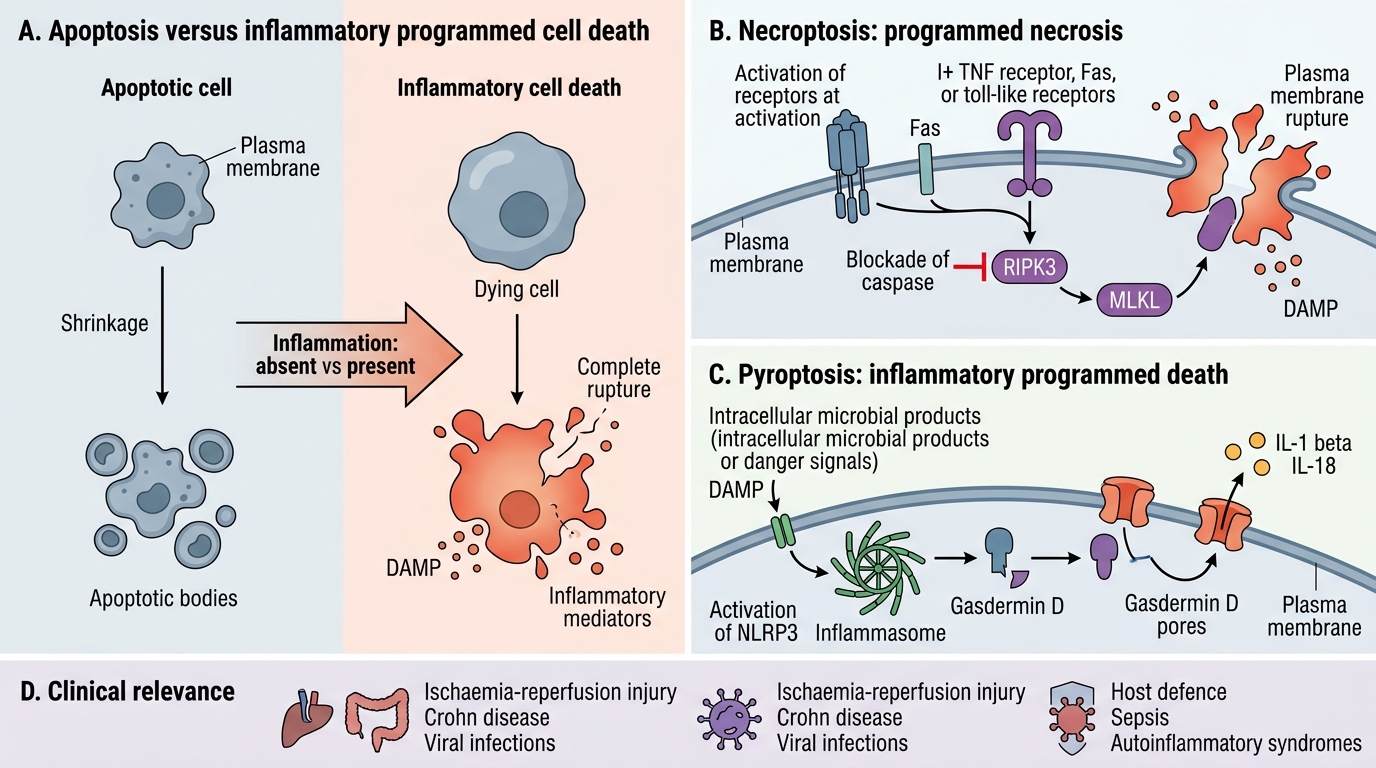
Necroptosis (programmed necrosis):
• Triggered by TNF receptor, Fas, or toll-like receptors when caspases are blocked (e.g., viral inhibition of caspases).
• Mediated by RIPK3 and MLKL (mixed-lineage kinase domain–like protein), which disrupt the plasma membrane.
• Morphology: necrosis-like (cell swelling, membrane rupture) but genetically regulated.
• Significance: contributes to inflammation in ischaemia-reperfusion injury, Crohn's disease, and some viral infections.
Pyroptosis (inflammatory programmed death):
• Triggered by intracellular pattern recognition (NLRP3 inflammasome) detecting microbial products or danger signals.
• Mediated by gasdermin D — forms pores in the plasma membrane.
• Releases large amounts of IL-1β and IL-18 — highly pro-inflammatory.
• Morphology: cell swelling, pore formation, DAMP and cytokine release.
• Significance: critical in host defence against intracellular pathogens; dysregulated in sepsis and autoinflammatory syndromes.
For Year-2 exams: you are expected to name and briefly define necroptosis and pyroptosis and state they cause inflammation (contrast with apoptosis). The mechanistic detail above is for understanding, not memorisation.
SELF-CHECK
Which of the following is the MOST accurate feature that distinguishes apoptosis from necrosis in a tissue section?
A. Presence of nuclear fragmentation
B. Increased eosinophilia of the cytoplasm
C. Loss of nuclear basophilia (karyolysis)
D. Absence of inflammatory infiltrate with single-cell death
Reveal Answer
Answer: D. Absence of inflammatory infiltrate with single-cell death
The combination of single-cell death WITHOUT an inflammatory response is the hallmark of apoptosis. Nuclear fragmentation (A) occurs in both processes — karyorrhexis in necrosis and internucleosomal fragmentation in apoptosis. Increased eosinophilia (B) and karyolysis (C) are features of necrosis. The key distinguishing point is that apoptotic bodies are cleared by phagocytosis before inflammation is triggered — hence the 'clean' microscopic appearance of apoptosis.
Pathological Calcification — Dystrophic and Metastatic
Pathological Calcification: Dystrophic vs Metastatic
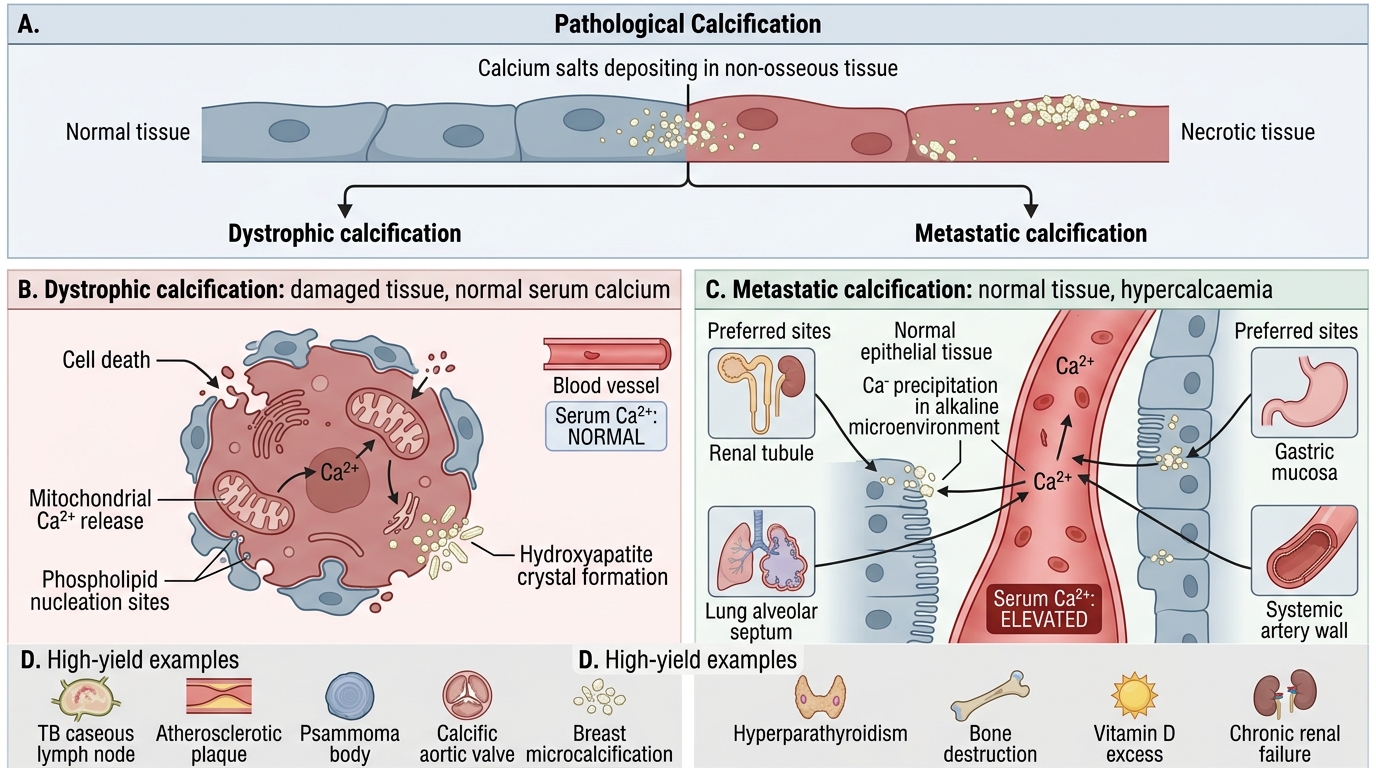
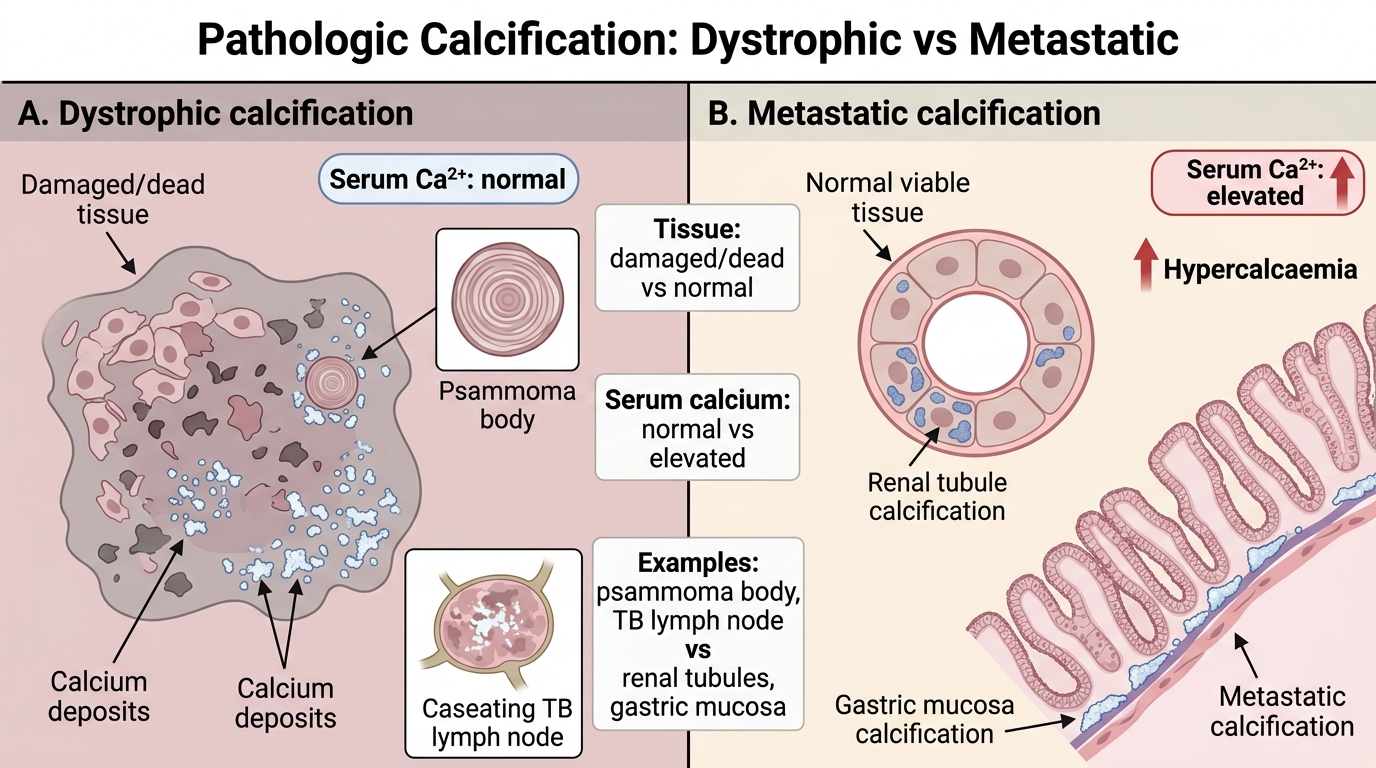
Pathological calcification is the deposition of calcium salts in non-osseous tissues. It is classified as dystrophic or metastatic based on the status of systemic calcium metabolism.
Dystrophic calcification:
• Definition: calcium deposition in dead or damaged tissue with normal serum calcium and phosphate.
• Mechanism: cell death → mitochondria release calcium (they normally sequester it) + phospholipid breakdown exposes nucleation sites → hydroxyapatite (Ca₁₀(PO₄)₆(OH)₂) crystals form in situ.
• Serum calcium: NORMAL.
• Tissue: dead/necrotic/damaged.
• Examples:
— Caseous necrosis of TB lymph node (the chalky-white deposit in the hook scenario)
— Atherosclerotic plaques (Mönckeberg's medial sclerosis is a variant)
— Old infarcts, dead parasites (Schistosoma, Echinococcus — "encysted" calcification)
— Psammoma bodies in papillary thyroid carcinoma, meningioma, ovarian serous carcinoma
— Calcific aortic stenosis (degenerative calcification of valve)
— Breast microcalcification on mammography (benign sclerosing adenosis or DCIS)
Metastatic calcification:
• Definition: calcium deposition in normal viable tissue due to hypercalcaemia.
• Mechanism: elevated serum calcium precipitates in tissues that normally maintain an alkaline pH (sites of acid secretion) or have high metabolic activity.
• Serum calcium: ELEVATED (hypercalcaemia).
• Tissue: normal (viable).
• Preferred sites (alkaline microenvironment): renal tubules (nephrocalcinosis), gastric mucosa, pulmonary alveolar walls, systemic blood vessel media, cornea (band keratopathy).
• Causes of hypercalcaemia: primary hyperparathyroidism, malignancy (PTHrP, lytic bone mets), sarcoidosis (↑vitamin D activation), vitamin D toxicity, milk-alkali syndrome, immobilisation.
Dystrophic vs Metastatic Calcification
CLINICAL PEARL
Psammoma bodies — the concentric, laminated calcific spherules seen in papillary thyroid carcinoma, papillary serous ovarian carcinoma, and meningioma — are a classic exam spotter for dystrophic calcification. Their presence does NOT indicate metastatic spread (despite the name); they represent focal dystrophic calcification within tumour papillae. However, their presence in a lymph node cytology sample can indicate metastatic papillary thyroid carcinoma even when no tumour cells are identified — the calcium is a diagnostic footprint of the primary tumour.
SELF-CHECK
A 45-year-old woman has chronic renal failure with a serum calcium of 3.1 mmol/L (elevated). Imaging shows calcium deposits in the lungs and gastric mucosa. Her renal biopsy shows calcium in tubular cells. The most likely diagnosis is:
A. Dystrophic calcification due to renal tubular necrosis
B. Psammoma body formation due to malignancy
C. Fat necrosis secondary to elevated lipase
D. Metastatic calcification due to hypercalcaemia
Reveal Answer
Answer: D. Metastatic calcification due to hypercalcaemia
This is metastatic calcification. The defining features are: (1) elevated serum calcium (3.1 mmol/L), (2) calcium depositing in normal viable tissues — lungs, gastric mucosa, renal tubules — all sites of alkaline pH that favour precipitation. Dystrophic calcification (A) requires dead/damaged tissue with normal serum calcium. Psammoma bodies (B) are a histological pattern of dystrophic calcification associated with specific tumours, not a cause. Fat necrosis (C) is unrelated to hypercalcaemia and affects adipose tissue via lipase action.
Integration: Linking Cell Death to Disease
Cell Death Patterns and Disease Links
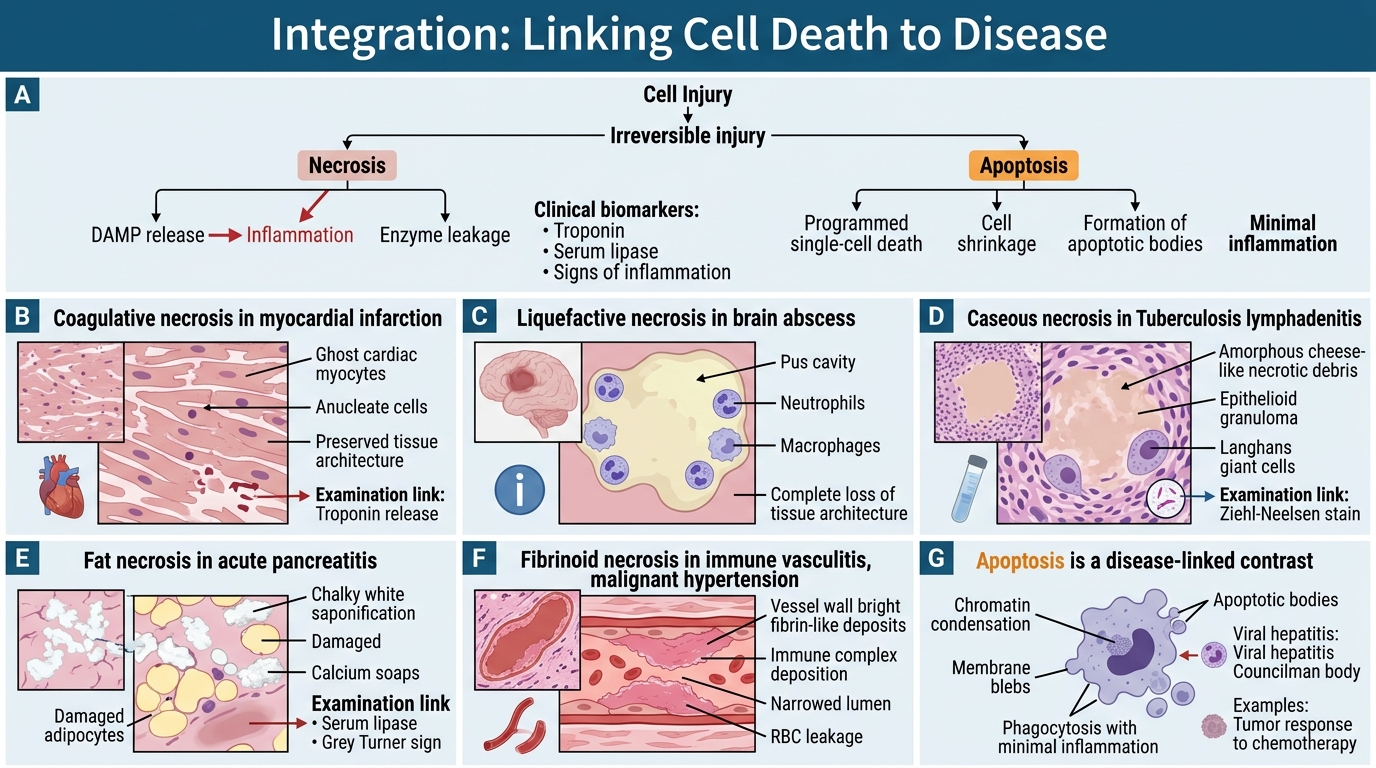
The table below consolidates the clinico-pathological links — this is the Year-2 synthesis level.
| Cell death type | Canonical clinical example | Key morphology on slide | Examination link |
|---|---|---|---|
| Coagulative necrosis | Myocardial infarction | Ghost cells, anucleate, intact architecture | MI staging, troponin release (DAMPs) |
| Liquefactive necrosis | Brain abscess | Pus cavity, neutrophils, no architecture | Bacterial meningitis → abscess |
| Caseous necrosis | TB lymphadenitis | Cheese-like debris, granuloma wall | ZN stain, caseation in primary complex |
| Fat necrosis | Acute pancreatitis | Chalky deposits, saponification | Serum lipase, Grey Turner sign |
| Fibrinoid necrosis | SLE vasculitis | Vessel wall smudgy pink | ANCA vasculitis, immune complex disease |
| Dry gangrene | Diabetic foot (PVD) | Mummification, line of demarcation | Buerger's, arterial Doppler |
| Wet gangrene | Strangulated bowel | Rapid spread, no demarcation | Emergency laparotomy |
| Gas gangrene | Trauma + Clostridium | Gas in soft tissue on X-ray | Crepitus, alpha-toxin (lecithinase) |
| Apoptosis (physiologic) | Thymic negative selection | Single cells, no inflammation | Immune tolerance |
| Apoptosis (pathologic) | Viral hepatitis | Councilman bodies in liver | Hepatitis B/C, ALT elevation |
| Dystrophic calcification | TB, atherosclerosis | Basophilic deposits, normal Ca | Psammoma bodies, valve calcification |
| Metastatic calcification | Hyperparathyroidism | Basophilic deposits, viable tissue, ↑Ca | Nephrocalcinosis, band keratopathy |