Page 6 of 24
PA2.4-5 | Cell Death — Necrosis, Apoptosis, Gangrene & Calcification — SDL Guide (Part 2)
Apoptosis: Definition, Morphology, and Significance
Apoptosis: Morphology and Significance
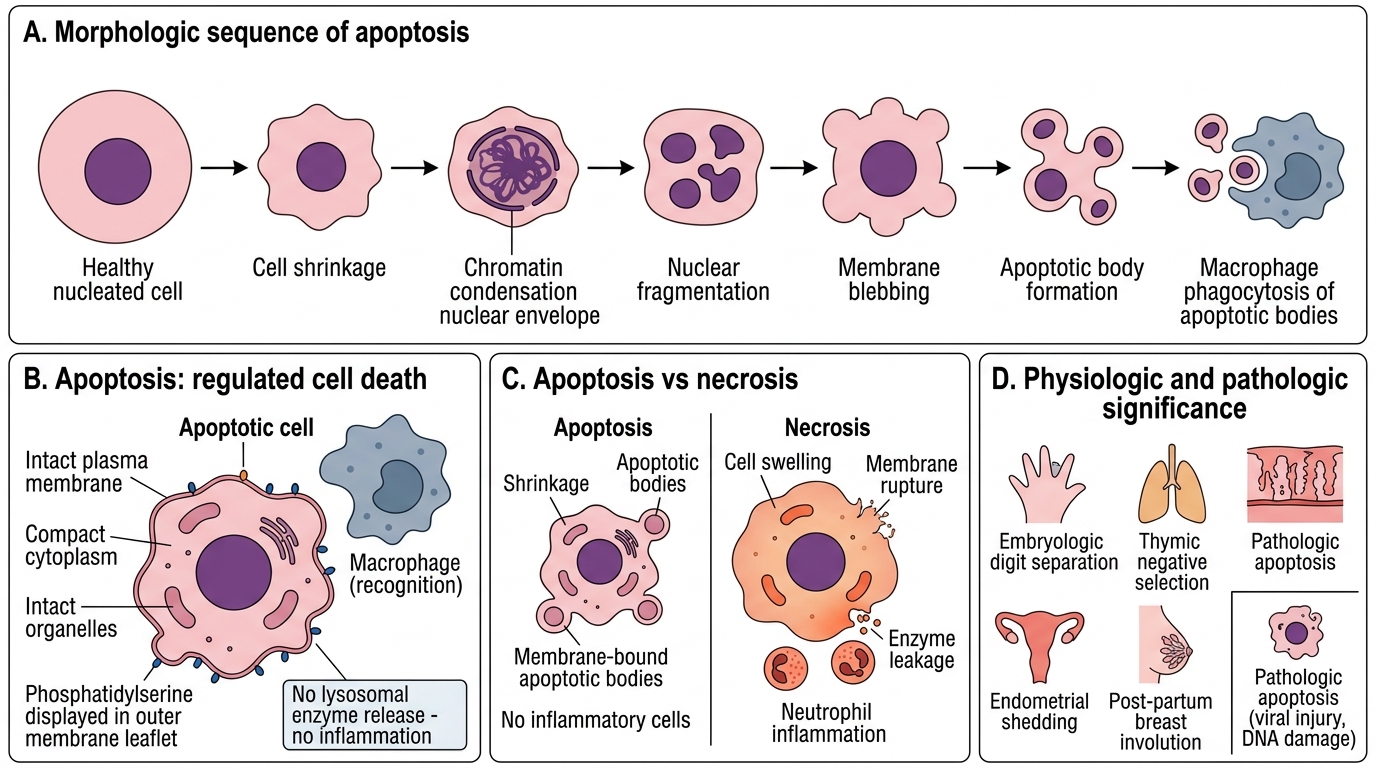
Apoptosis (Greek: apo = away, ptosis = falling — like leaves falling from a tree) is a form of programmed cell death in which the cell activates an intrinsic suicide programme. Unlike necrosis, apoptosis is highly regulated, energy-dependent, and does not elicit an inflammatory response.
Morphological hallmarks of apoptosis:
• Cell shrinkage — cytoplasm condenses; organelles remain intact but are compacted.
• Chromatin condensation (pyknosis) — chromatin aggregates beneath the nuclear envelope in a crescent or cap pattern; unlike necrotic pyknosis, the nuclear membrane remains intact initially.
• Nuclear fragmentation — condensed chromatin breaks into discrete fragments (compare: karyorrhexis in necrosis is random fragmentation).
• Formation of apoptotic bodies — the cell blebs and fragments into membrane-bound vesicles containing intact organelles and nuclear fragments.
• Phagocytosis by neighbouring cells or macrophages — apoptotic bodies are rapidly recognised (by phosphatidylserine flipped to the outer leaflet) and engulfed. No lysosomal enzyme release → no inflammation.
Physiologic apoptosis (normal, essential):
• Embryological morphogenesis (digit separation, neural tube closure)
• Thymic negative selection (deletion of autoreactive T cells)
• Endometrial shedding (menstruation)
• Regression of lactating breast post-partum
Pathologic apoptosis:
• Viral hepatitis (Councilman / acidophil bodies — apoptotic hepatocytes)
• Radiation and chemotherapy-induced tumour cell death (desired)
• Excessive apoptosis in neurodegenerative disease (Parkinson's, Alzheimer's)
• Deficient apoptosis in cancer (BCL-2 overexpression in follicular lymphoma)
Apoptosis Pathways — Intrinsic and Extrinsic
Intrinsic and Extrinsic Apoptosis Pathways
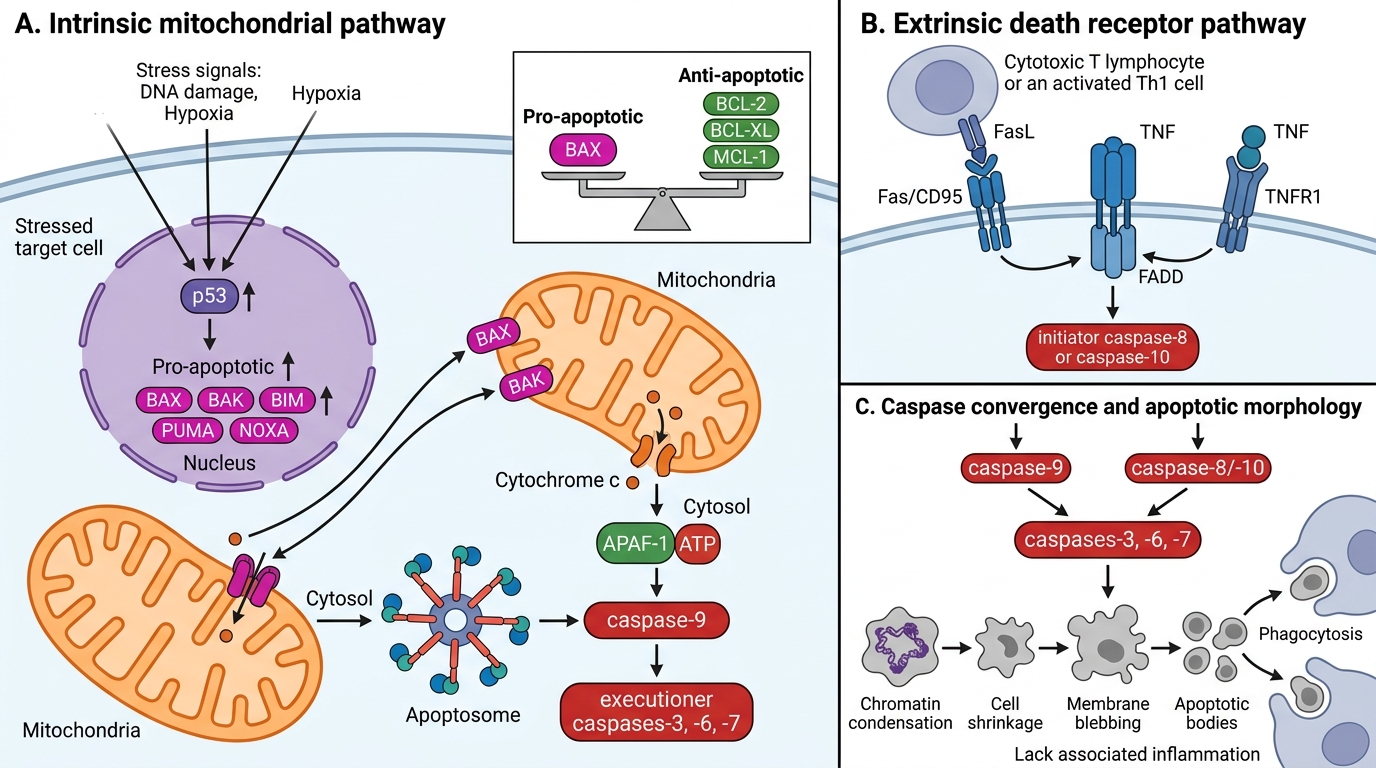
Both pathways converge on activation of caspases — a family of cysteine proteases that execute the cell death programme. Caspases exist as inactive pro-caspases; their sequential activation forms a cascade.
Intrinsic (mitochondrial) pathway:
• Triggers: DNA damage (radiation, chemotherapy), hypoxia, growth factor withdrawal, oncogene activation, oxidative stress.
• Sensors: tumour suppressor p53 senses DNA damage → transcribes pro-apoptotic BCL-2 family members (BAX, BAK, BIM, PUMA, NOXA).
• BCL-2 family balance (master regulator):
— Pro-apoptotic: BAX, BAK (form mitochondrial pores)
— Anti-apoptotic: BCL-2, BCL-XL, MCL-1 (block pore formation)
— BH3-only sensors: BIM, PUMA, NOXA (neutralise anti-apoptotic members when the cell is stressed)
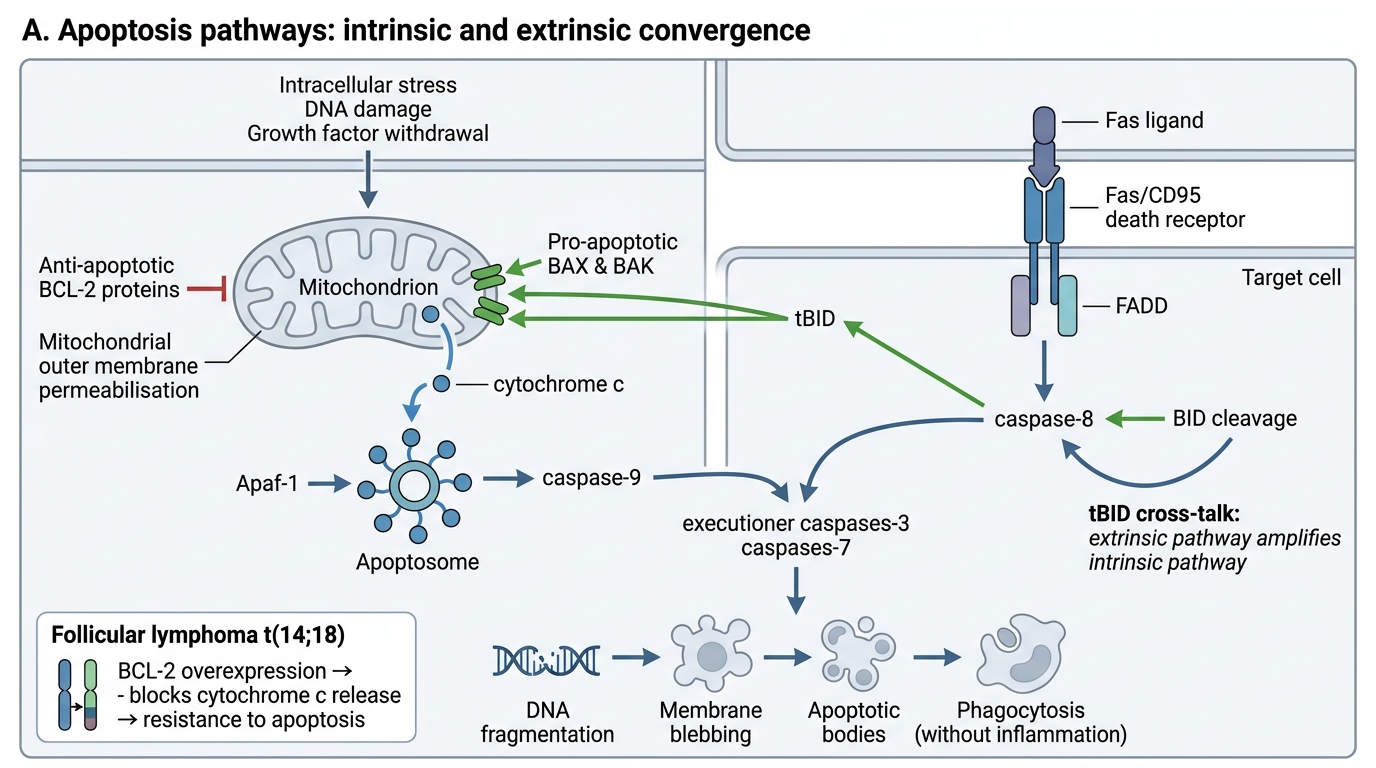
• When BAX/BAK exceed BCL-2/BCL-XL: outer mitochondrial membrane permeabilisation → release of cytochrome c into cytosol.
• Cytochrome c + APAF-1 + ATP → apoptosome → activates initiator caspase-9 → cleaves and activates executioner caspases-3/6/7.
Extrinsic (death receptor) pathway:
• Triggers: immune surveillance; physiological deletion of lymphocytes; cytotoxic T-lymphocyte killing.
• Key receptor: Fas (CD95) on target cell surface; ligand: FasL on cytotoxic T cell or activated Th1 cell.
• Also: TNF receptor 1 (TNFR1) bound by TNF.
• Receptor trimerisation → recruitment of FADD (Fas-associated death domain) → recruitment and auto-activation of initiator caspase-8 (or -10) → activates executioner caspases-3/7.
• In some cells (Type II, e.g. hepatocytes): caspase-8 also cleaves BID → truncated BID (tBID) amplifies signal through the intrinsic pathway.
Executioner phase (shared):
Caspases-3/6/7 activate:
• CAD (caspase-activated DNase) → internucleosomal DNA fragmentation (ladder on gel)
• Cytoskeletal/nuclear protein cleavage → blebbing, condensation
• Flippase inhibition → phosphatidylserine externalisation → eat-me signal
Intrinsic and Extrinsic Apoptosis Pathways
SELF-CHECK
In follicular lymphoma, the t(14;18) translocation juxtaposes BCL-2 to the immunoglobulin heavy-chain locus, causing BCL-2 overexpression. What is the direct consequence for the lymphoma cells?
A. Increased mitosis — cells divide faster
B. Activation of caspase-9 — cells undergo spontaneous apoptosis
C. Resistance to apoptosis — cells accumulate because they cannot die
D. Loss of phosphatidylserine — cells evade phagocytosis
Reveal Answer
Answer: C. Resistance to apoptosis — cells accumulate because they cannot die
BCL-2 is an anti-apoptotic protein that blocks mitochondrial outer membrane permeabilisation and cytochrome c release. Overexpression suppresses the intrinsic pathway even when pro-apoptotic signals are present — the lymphoma cells simply accumulate rather than proliferating rapidly (BCL-2 does not drive proliferation). Option A is wrong: BCL-2 overexpression confers survival, not proliferative drive. Option B is the opposite: BCL-2 overexpression blocks, not activates, caspase-9. This is the classic teaching point: BCL-2-positive follicular lymphoma is typically slow-growing but incurable because normal cell turnover is abolished.
Necrosis vs Apoptosis — The High-Yield Comparison
Necrosis vs Apoptosis: High-Yield Comparison
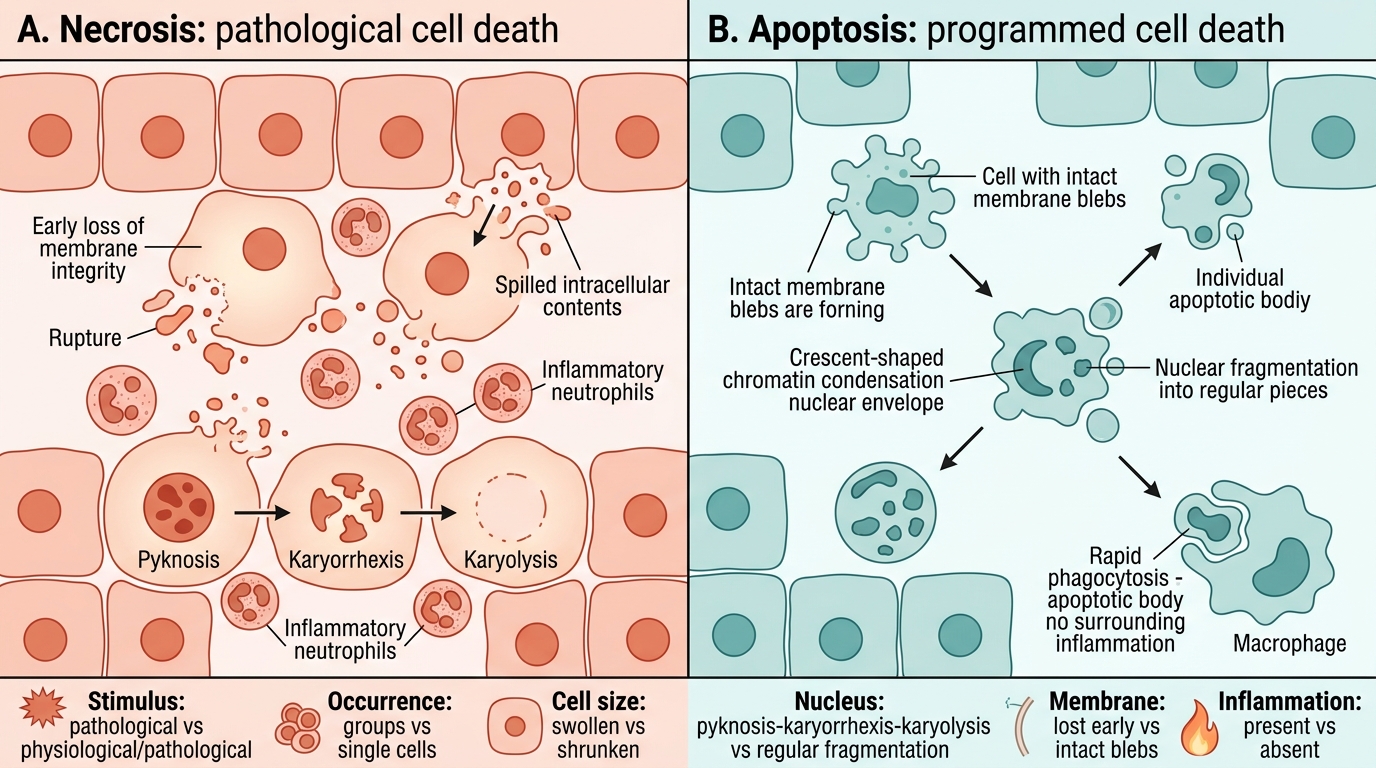
The necrosis–apoptosis distinction is a guaranteed exam question. Master this table.
| Feature | Necrosis | Apoptosis |
|---|---|---|
| Stimulus | Pathological (ischaemia, toxins, infection) | Physiological OR pathological |
| Occurrence | Groups of cells | Single cells or small clusters |
| Cell size | Swollen (oncosis) | Shrunken |
| Nucleus | Pyknosis → karyorrhexis → karyolysis | Fragmentation (regular pattern), crescent condensation |
| Membrane integrity | Lost early → contents leak | Maintained until apoptotic bodies form |
| Cytoplasm | Eosinophilic, vacuolated, dissolves | Condensed, intact organelles |
| Apoptotic bodies | Absent | Present (membrane-bound) |
| Inflammation | Prominent (DAMP release) | Absent (rapid phagocytosis, no DAMP release) |
| Energy requirement | Passive — no ATP needed | Active — requires ATP |
| Reversibility | Never once committed | Up to a late point (BCL-2 can block) |
| Clinical example | MI, infarct, abscess | Embryogenesis, thymic selection, viral hepatitis |
IMPORTANT: One reliable exam trick: the question describes "single cells surrounded by normal cells, no inflammation" → apoptosis. "Large zone of dead cells with neutrophil infiltrate" → necrosis.
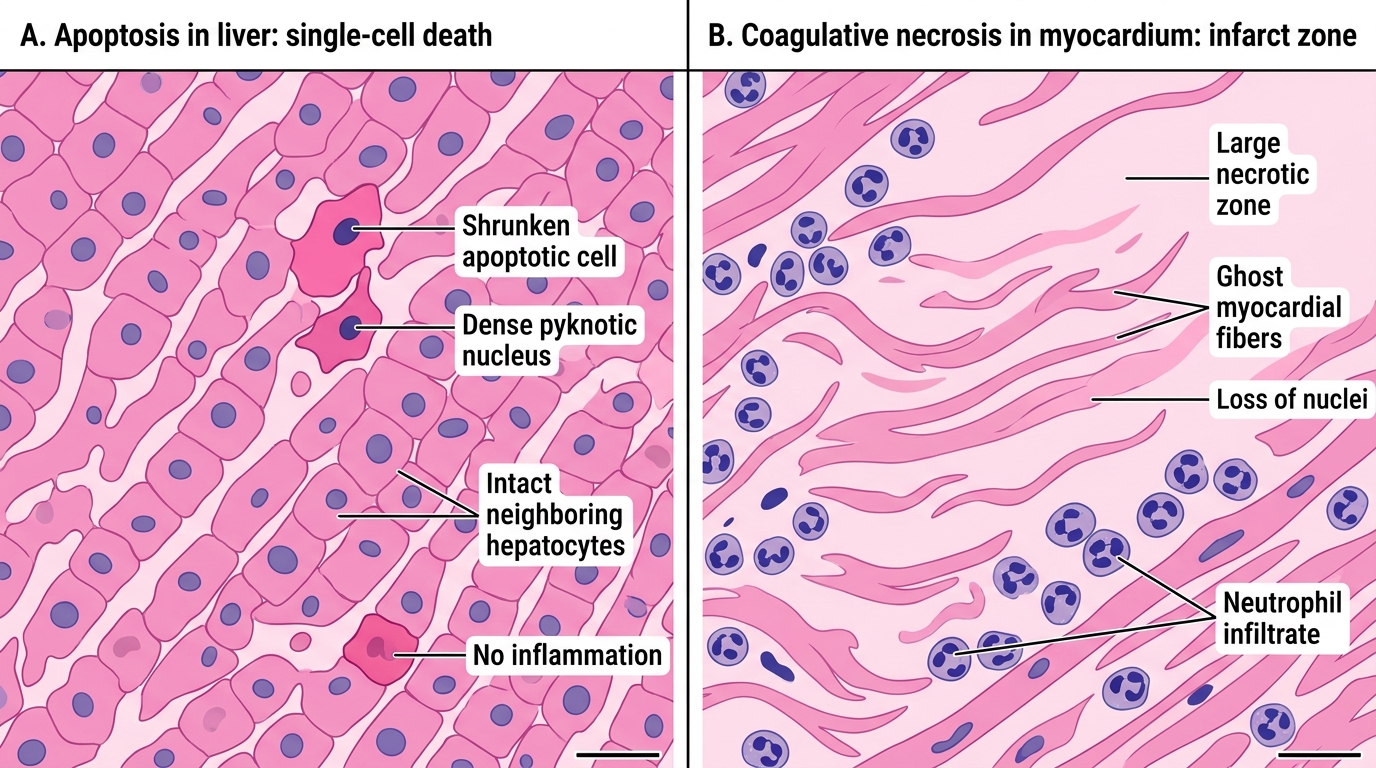
Apoptosis Versus Necrosis on H&E