Page 14 of 24
PA2.8 | Cell Injury Morphology — Practical — SDL Guide
Learning Objectives
- Adopt a systematic low-to-high power approach for reading histological sections showing cell injury
- Identify the microscopic features of reversible injury: hydropic swelling and fatty change
- Distinguish coagulative, liquefactive, caseous and fat necrosis on H&E sections by their cardinal features
- Recognise gross patterns of infarction, gangrene and caseous lymph nodes
- Identify apoptotic bodies, dystrophic calcification and common pigment deposits on H&E
- Correlate each morphological pattern with its underlying pathophysiological mechanism and likely aetiology
INSTRUCTIONS
Practical pathology is a visual discipline — the diagnosis lives in what you see, not just what you memorise. This module trains the pattern-recognition skills you will use every time you pick up a microscope or handle a gross specimen. Work through each section actively: pause at every image, name the feature before reading the caption, and use the self-checks to test your call. By the end you will have a reliable, stepwise approach to any cell-injury slide or specimen.
References
- Robbins and Cotran Pathologic Basis of Disease, 10th ed., Ch 2 (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 2 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A prosector hands you a pale, wedge-shaped slice of kidney and a glass slide. No clinical history. No label beyond 'kidney, right, nephrectomy'. In the next ninety seconds you are expected to name the lesion, grade the severity and suggest the most likely cause. This module gives you the visual vocabulary and the method to do exactly that — reliably, every time.
WHY THIS MATTERS
PA2.8 is examined both in theory papers and in the spotting practical, where you identify gross and microscopic specimens under time pressure. Pattern recognition in cell injury also underpins almost every downstream chapter: ischaemia, inflammation, neoplasia, and organ-specific pathology all build on the morphological vocabulary established here. Getting these patterns right now saves you from confusion later.
RECALL
Before going further, recall from your Year-1 Cell Biology:
- ATP depletion — the universal trigger for reversible cell injury
- The point of no return — irreversible membrane injury leading to necrosis
- Apoptosis vs necrosis — programmed silent death vs accidental lytic death
- The four types of necrosis you named in theory: coagulative, liquefactive, caseous, fat necrosis
If any of these feel shaky, spend five minutes with Robbins Ch 2 theory sections before continuing.
The Systematic Approach: How to Read a Cell-Injury Section
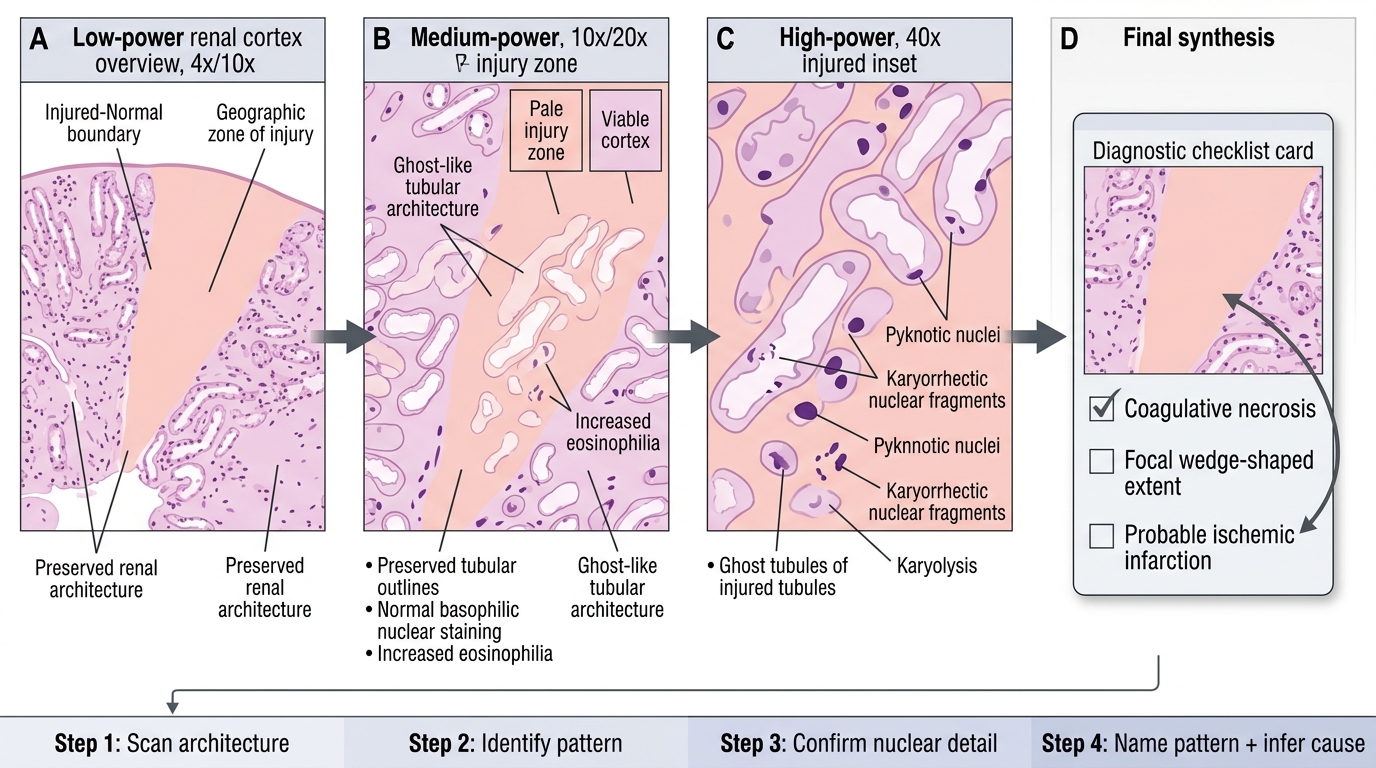
Systematic Reading of a Cell-Injury Section
A structured approach prevents the most common practical error — jumping to a diagnosis before surveying the whole slide.
Step 1 — Scan at low power (4× or 10×): Map the architecture. Is the tissue preserved or destroyed? Is there a geographic zone of injury? Where is the boundary between injured and normal?
Step 2 — Identify the pattern at medium power (10–20×): Is the overall staining pale or eosinophilic? Are there cystic spaces? Is there a granuloma? A ghost outline with no nuclei?
Step 3 — Confirm at high power (40×): Examine nuclear details — karyolysis (nuclear dissolution), karyorrhexis (nuclear fragmentation), pyknosis (nuclear condensation). Identify cell type and any infiltrate.
Step 4 — Name the pattern and infer the cause: Match features to the checklist in this module. Ask: which process produces this combination of findings?
Always annotate your answer: type of injury + extent + probable aetiology.
SELF-CHECK
On a 4× scan of a renal cortex section you notice a pale, wedge-shaped zone with preserved tubular outlines but no visible nuclei. Which step of the systematic approach gives you this information?
A. Step 1 — low-power architecture scan
B. Step 3 — high-power nuclear detail
C. Step 4 — aetiological inference
D. Step 2 — medium-power pattern identification
Reveal Answer
Answer: A. Step 1 — low-power architecture scan
The geographic wedge shape and overall zone of pallor are low-power (4–10×) architectural features identified in Step 1. Nuclear detail (karyolysis, etc.) is a Step 3 finding confirmed at high power.
Reversible Injury: Hydropic Swelling and Fatty Change
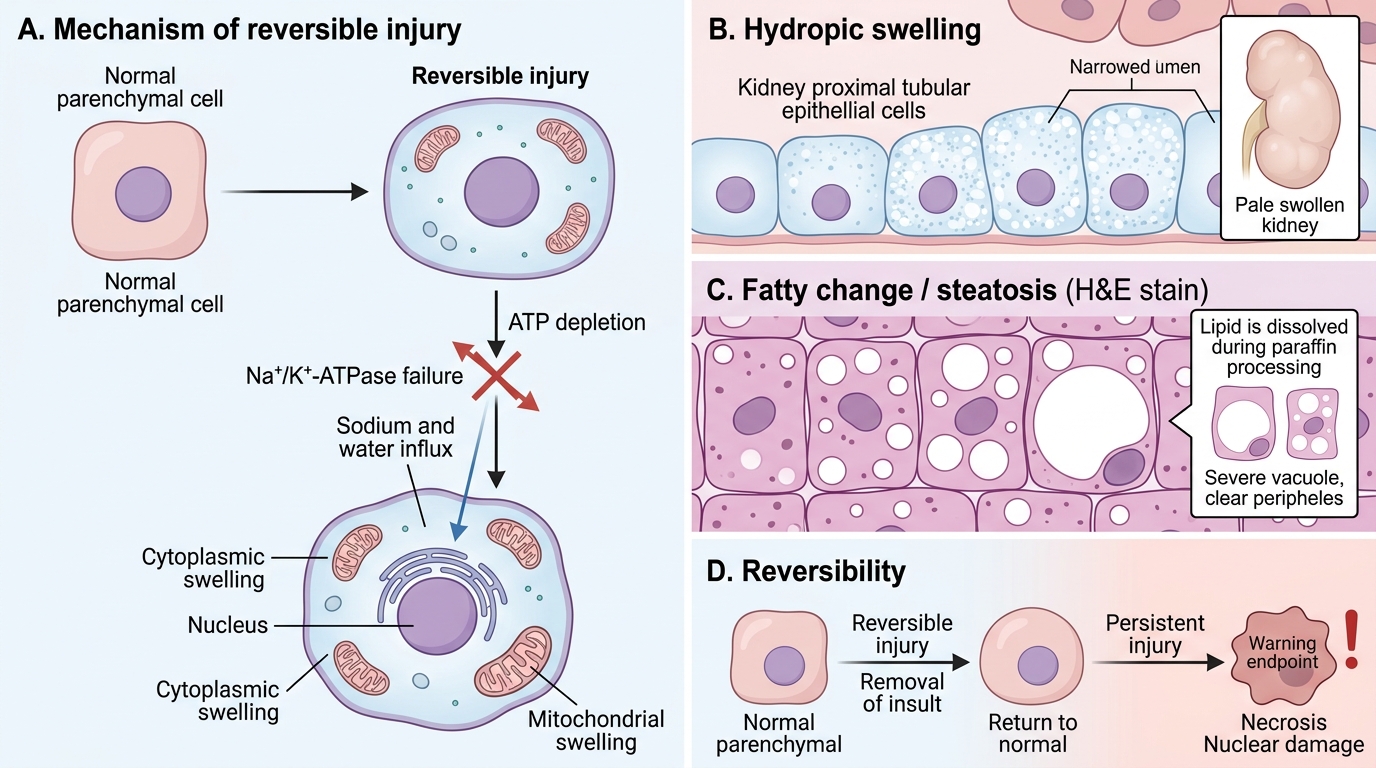
Reversible injury produces two classic microscopic patterns, both encountered in the practical.
Hydropic (cellular) swelling — the earliest and most common form:
- Cells appear enlarged, with pale, finely vacuolated or 'watery' cytoplasm
- Nucleus remains intact (key distinction from necrosis)
- Cytoplasmic pallor results from dilution of proteins by inflowing water (Na⁺/K⁺-ATPase fails)
- Seen in kidney proximal tubules (most sensitive), hepatocytes, myocardial fibres
- On gross: organ is swollen, pale, weight increased, capsule tense
Fatty change (steatosis) — accumulation of triglyceride within parenchymal cells:
- Clear cytoplasmic vacuoles of varying size; in severe cases the nucleus is displaced to the periphery ('signet-ring' hepatocyte)
- Vacuoles appear empty on H&E because lipid is dissolved during paraffin processing
- Confirm with Oil Red O on frozen sections (not available in routine H&E)
- Liver is the principal site; also heart ('tigroid heart' in severe anaemia/diphtheria)
- Causes: alcohol, protein malnutrition, diabetes, drug toxicity, hypoxia
IMPORTE: both patterns are potentially reversible — restore the insult and the cell recovers.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Reversible Cell Injury: Hydropic Swelling and Fatty Change
SELF-CHECK
On a liver biopsy H&E section, many hepatocytes contain large clear cytoplasmic vacuoles with the nucleus pushed to the cell periphery. What does this most likely represent, and why are the vacuoles clear?
A. Glycogen accumulation; glycogen is leached during dehydration steps
B. Fatty change (steatosis); lipid is dissolved by organic solvents during paraffin processing
C. Hydropic swelling; excess water evaporates during mounting
D. Liquefactive necrosis; the cytoplasm has been digested
Reveal Answer
Answer: B. Fatty change (steatosis); lipid is dissolved by organic solvents during paraffin processing
The signet-ring appearance (peripheral nucleus, large clear vacuole) is classic fatty change. Lipid dissolves in the xylene/alcohol steps of paraffin processing, leaving an empty space. Glycogen vacuoles are smaller and PAS-positive. Hydropic swelling produces fine granular pallor, not large discrete vacuoles.
Coagulative Necrosis: The Ghost Town Pattern
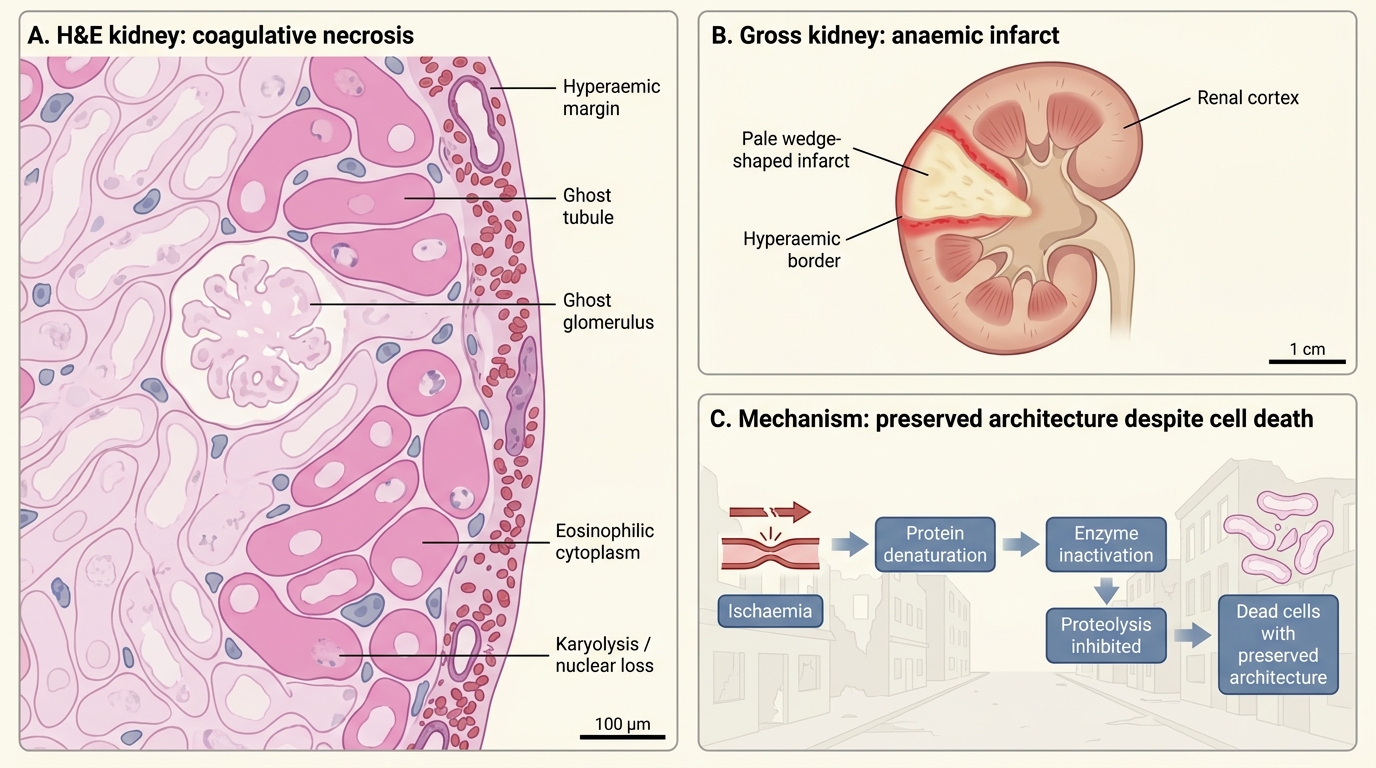
Coagulative necrosis is the most common form of necrosis and the type you will see most often in the practical.
Mechanism: Denaturation of structural and enzymatic proteins; proteolysis is inhibited. Architecture is preserved but cells are dead.
Classic H&E features:
• Preserved tissue architecture — you can still identify glomeruli, tubules, or myofibres ('ghost outlines')
• Deeply eosinophilic (pink) cytoplasm — denatured proteins take up eosin avidly
• Nuclear loss — karyolysis is the dominant change; pyknosis and karyorrhexis in the transition zone
• No inflammatory infiltrate in the acute phase; macrophages appear by 48–72 hours
Gross correlate — pale (anaemic) infarct:
• Firm, pale-yellow or pale-tan wedge-shaped area with a hyperaemic border
• Seen in: kidney (most classic), heart (myocardial infarct), spleen
• Solid organs with end-arterial supply and no collaterals → coagulative pattern
Coagulative Necrosis: The Ghost Town Pattern
SELF-CHECK
A 55-year-old man dies 36 hours after an acute MI. The pathologist takes a section from the pale, firm, yellow-grey zone of the left ventricular wall. Which combination of H&E features is MOST expected?
A. Pale ghost myofibres with preserved cross-striations, nuclear loss by karyolysis, no neutrophils yet
B. Cystic space filled with neutrophils, complete loss of tissue architecture
C. Amorphous granular eosinophilic debris surrounded by palisading epithelioid cells
D. Saponified fat with basophilic calcium deposits and fat-laden macrophages
Reveal Answer
Answer: A. Pale ghost myofibres with preserved cross-striations, nuclear loss by karyolysis, no neutrophils yet
At 36 hours the heart shows early coagulative necrosis: preserved myofibre outlines ('ghost fibres'), deep eosinophilia, karyolysis. Neutrophils begin to appear at ~12–24 hours but peak at 1–3 days. Cystic destruction is liquefactive necrosis. Granulomatous debris is caseous. Saponification is fat necrosis.