Page 15 of 24
PA2.8 | Cell Injury Morphology — Practical — SDL Guide (Part 2)
Liquefactive Necrosis: The Dissolved Core Pattern
Liquefactive Necrosis: The Dissolved Core Pattern
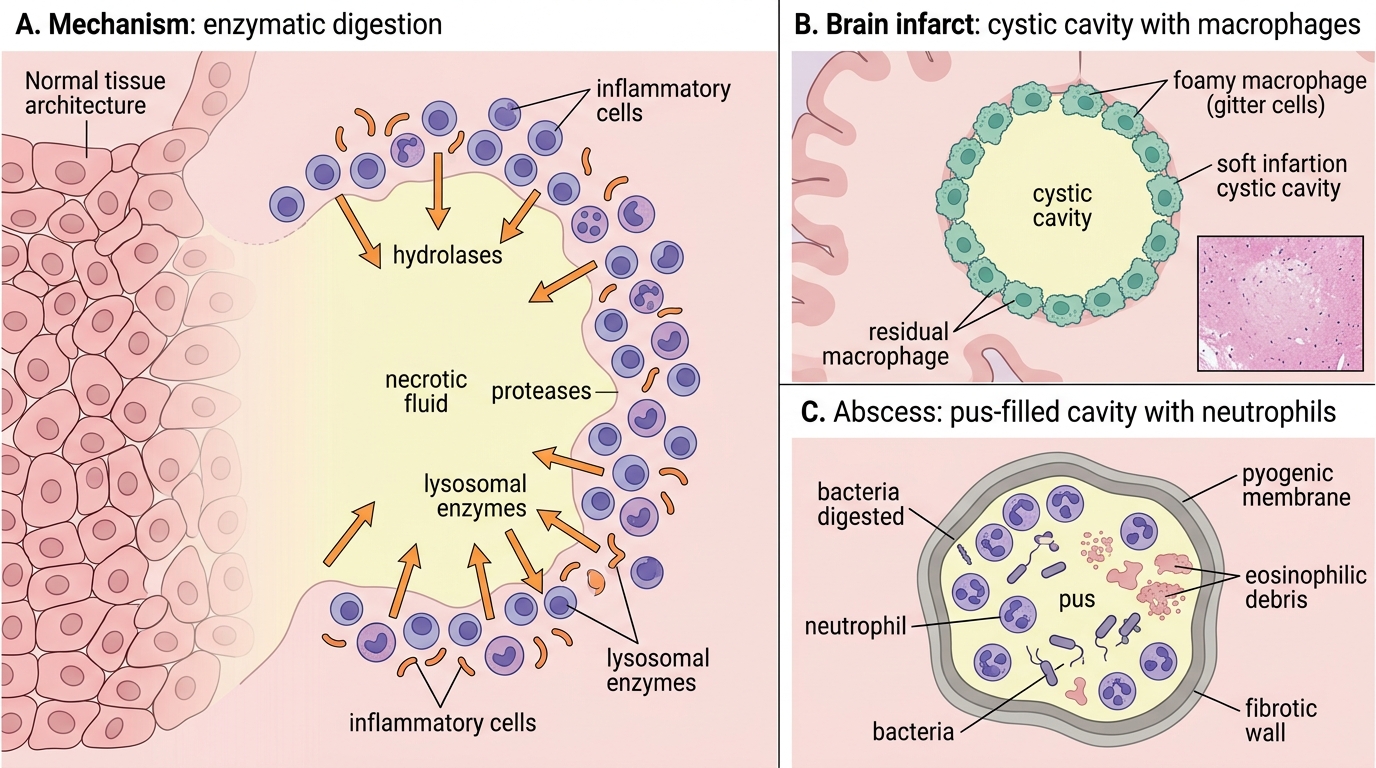
Liquefactive necrosis results from enzymatic digestion of dead cells, converting the tissue to liquid pus or cystic fluid.
Two distinct settings:
- Brain infarction — neurons lack the structural protein reserve to coagulate; their own hydrolases liquefy the zone. Result: a cystic cavity lined by macrophages, no architecture.
- Bacterial/fungal abscess — polymorphonuclear neutrophils (PMNs) release proteases and lysosomal enzymes that digest both bacteria and surrounding tissue.
H&E features:
• Complete loss of tissue architecture — no ghost outlines
• A cystic space or irregular cavity
• Abundant neutrophils (in abscess) OR macrophages (late brain infarct)
• Granular eosinophilic debris (pus) in bacterial abscesses
• Fibrotic wall around an old abscess
Gross: brain infarct appears as a soft, gelatinous, then cystic pale area; abscess as pus-filled cavity with thick pyogenic membrane.
SELF-CHECK
A section from a cerebral infarct (3-week-old lesion) shows a cystic cavity with foamy macrophages ('gitter cells') at the margins and no residual neuronal outlines. This is best classified as:
A. Caseous necrosis, because of the granular debris
B. Fat necrosis, because of the foamy macrophages
C. Liquefactive necrosis, because of complete architectural dissolution and macrophagic cleanup
D. Coagulative necrosis with secondary autolysis
Reveal Answer
Answer: C. Liquefactive necrosis, because of complete architectural dissolution and macrophagic cleanup
Liquefactive necrosis in the brain produces complete tissue dissolution → cystic cavity. Foamy macrophages ('gitter cells' or microglia) are the cleanup crew, phagocytosing lipid-rich myelin debris. This is a cardinal feature of subacute/resolving brain infarct, not fat necrosis. Fat necrosis occurs in adipose tissue, not brain parenchyma.
Caseous Necrosis: The Granuloma Pattern
Caseous necrosis is pathognomonic of tuberculosis (and a few other granulomatous diseases: histoplasmosis, sarcoidosis rarely).
Gross appearance:
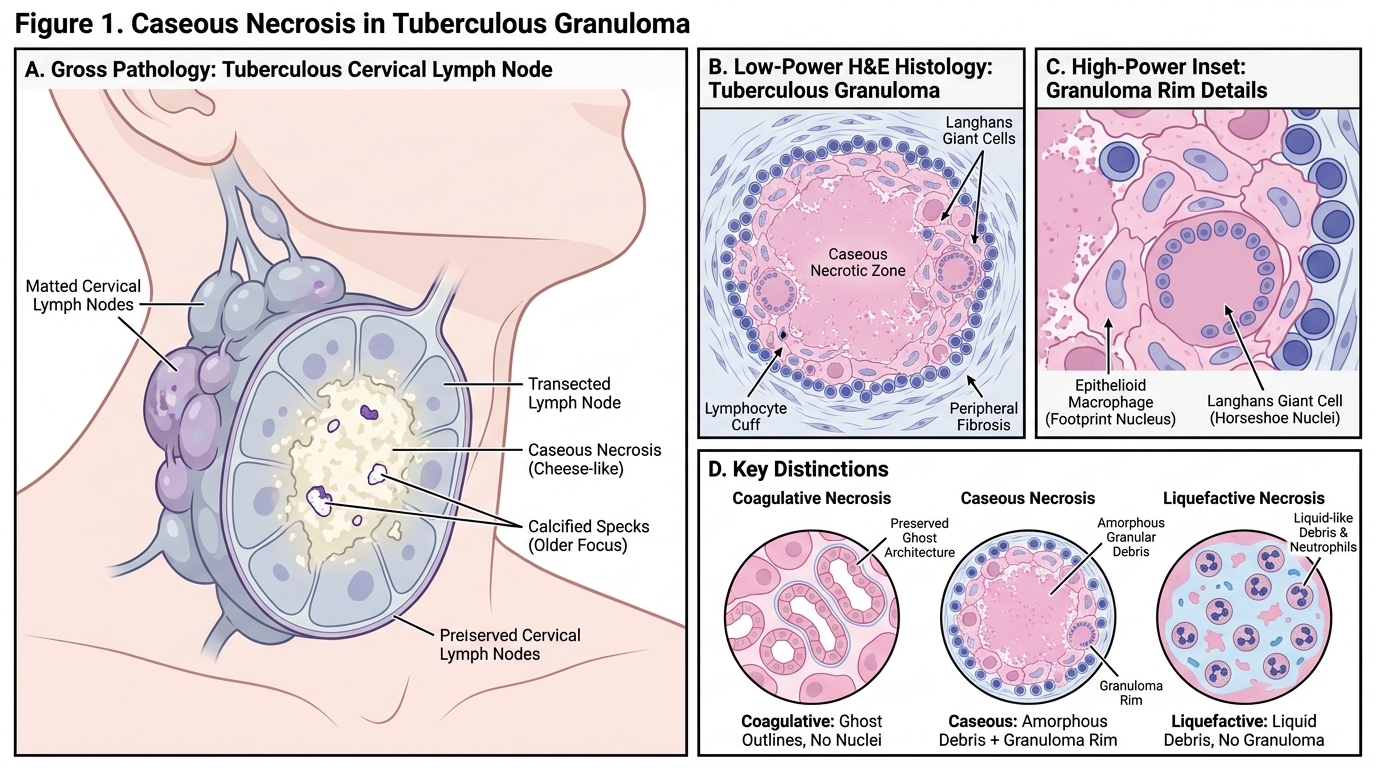
• Soft, crumbling, cheese-like pale material — hence 'caseous' (Latin: caseus = cheese)
• Seen in TB lymph nodes (most common in India), TB lung (Ghon focus), miliary nodules
• Caseous lymph nodes: matted, firm, may show central softening or calcification
H&E microscopy:
• Central zone of amorphous granular eosinophilic debris — featureless, no ghost outlines, no nuclei
• Surrounded by a granuloma rim: epithelioid macrophages (elongated, pale 'footprint' nuclei) + Langhans giant cells (horseshoe peripheral nuclear arrangement) + lymphocytes
• Variable peripheral fibrosis in healing lesions
• Dystrophic calcification (basophilic granular deposits) in old caseous foci — 'Ranke complex'
Key distinction from coagulative: no ghost architecture; the central zone is completely unrecognisable. Key distinction from liquefactive: solid debris, not liquid; granuloma present.
Caseous Necrosis: Tuberculous Granuloma Pattern
SELF-CHECK
A cervical lymph node biopsy shows a central zone of structureless granular eosinophilic material surrounded by elongated pale macrophages and a multinucleated giant cell with nuclei arranged in a horseshoe pattern. Which stain should be ordered NEXT, and why?
A. Oil Red O; to confirm lipid accumulation in the macrophages
B. Ziehl-Neelsen (ZN) stain; to demonstrate acid-fast bacilli in the caseous debris or macrophages
C. PAS stain; to identify glycogen in the ghost cells
D. Masson trichrome; to quantify collagen in the granuloma
Reveal Answer
Answer: B. Ziehl-Neelsen (ZN) stain; to demonstrate acid-fast bacilli in the caseous debris or macrophages
The morphology — caseous debris + epithelioid granuloma + Langhans giant cells — is essentially diagnostic of tuberculosis. ZN stain identifies acid-fast mycobacteria and should be the immediate next step. Oil Red O requires frozen sections and detects fat, not mycobacteria. PAS detects fungi/glycogen but is not the priority here.
Fat Necrosis: The Saponification Pattern
Fat Necrosis and Saponification
Fat necrosis occurs exclusively in adipose tissue and has two forms:
1. Enzymatic fat necrosis (pancreatic):
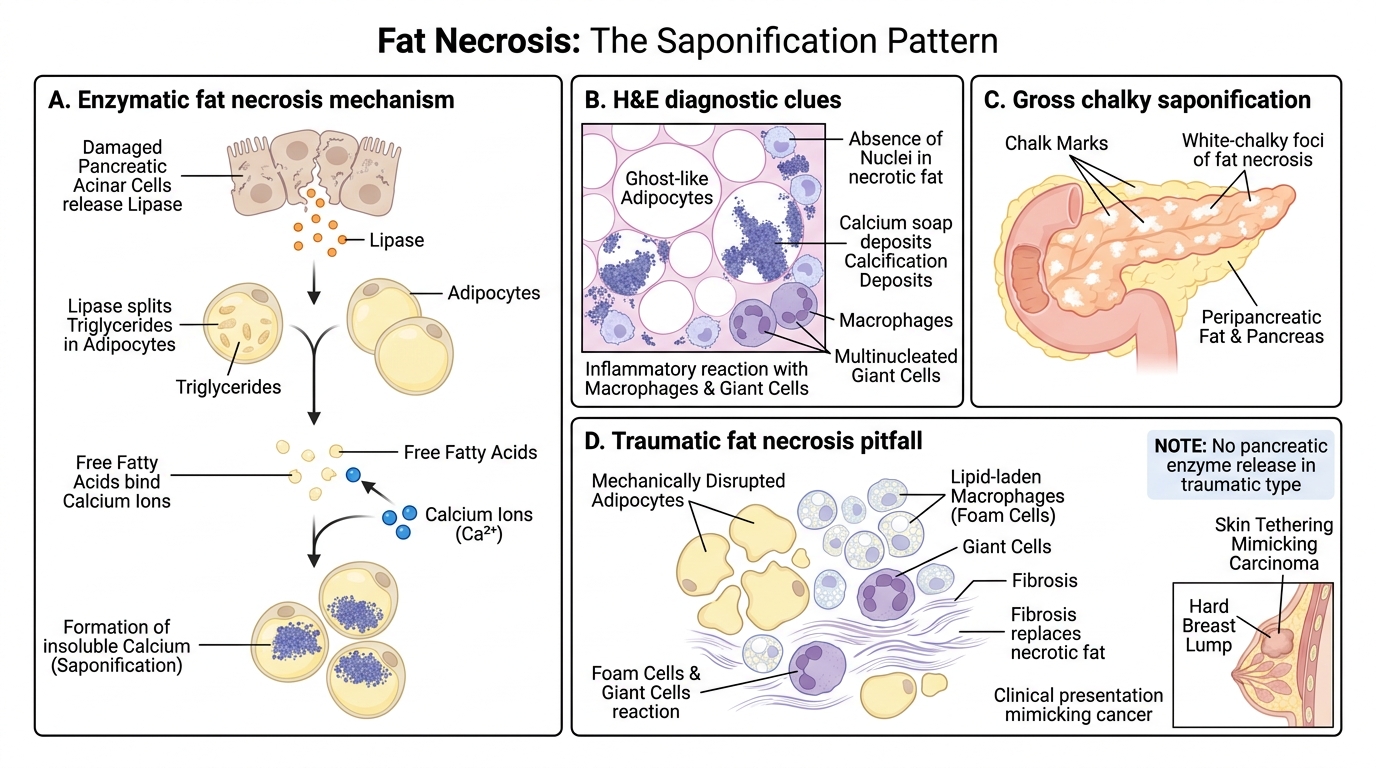
• Mechanism: lipases released from damaged acinar cells split triglycerides → free fatty acids
• Free fatty acids + calcium → calcium soaps (saponification)
• H&E: foci of ghost-like adipocytes with basophilic granular calcification deposits; surrounded by macrophages and giant cells
• Gross: white-chalky foci ('chalk marks') scattered in peripancreatic fat — palpable in acute pancreatitis
2. Traumatic fat necrosis (breast, subcutaneous):
• No enzyme release; mechanical disruption of fat cells → lipase liberation from dead cells
• Surrounded by lipid-laden macrophages (foam cells) + giant cells + fibrosis
• May mimic carcinoma clinically (hard lump with skin tethering) — important diagnostic pitfall!
H&E diagnostic clues for enzymatic fat:
• Basophilic (blue) deposits — the only necrosis type with primary basophilia
• Ghost adipocytes — empty membrane outlines
• Macrophage infiltration at the margin
• No nuclear debris, no tissue architecture