Page 16 of 24
PA2.8 | Cell Injury Morphology — Practical — SDL Guide (Part 3)
The 2×2 Comparison Grid: Four Necrosis Patterns at a Glance
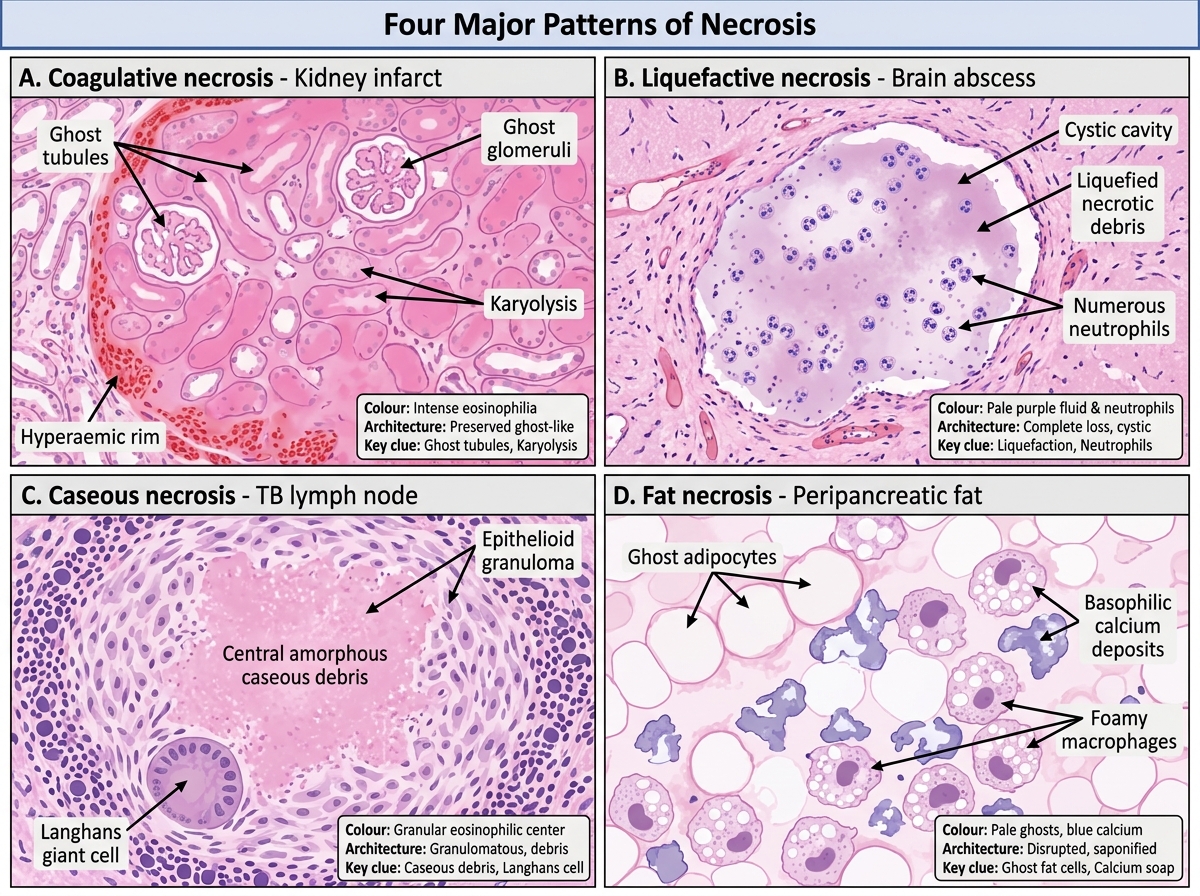
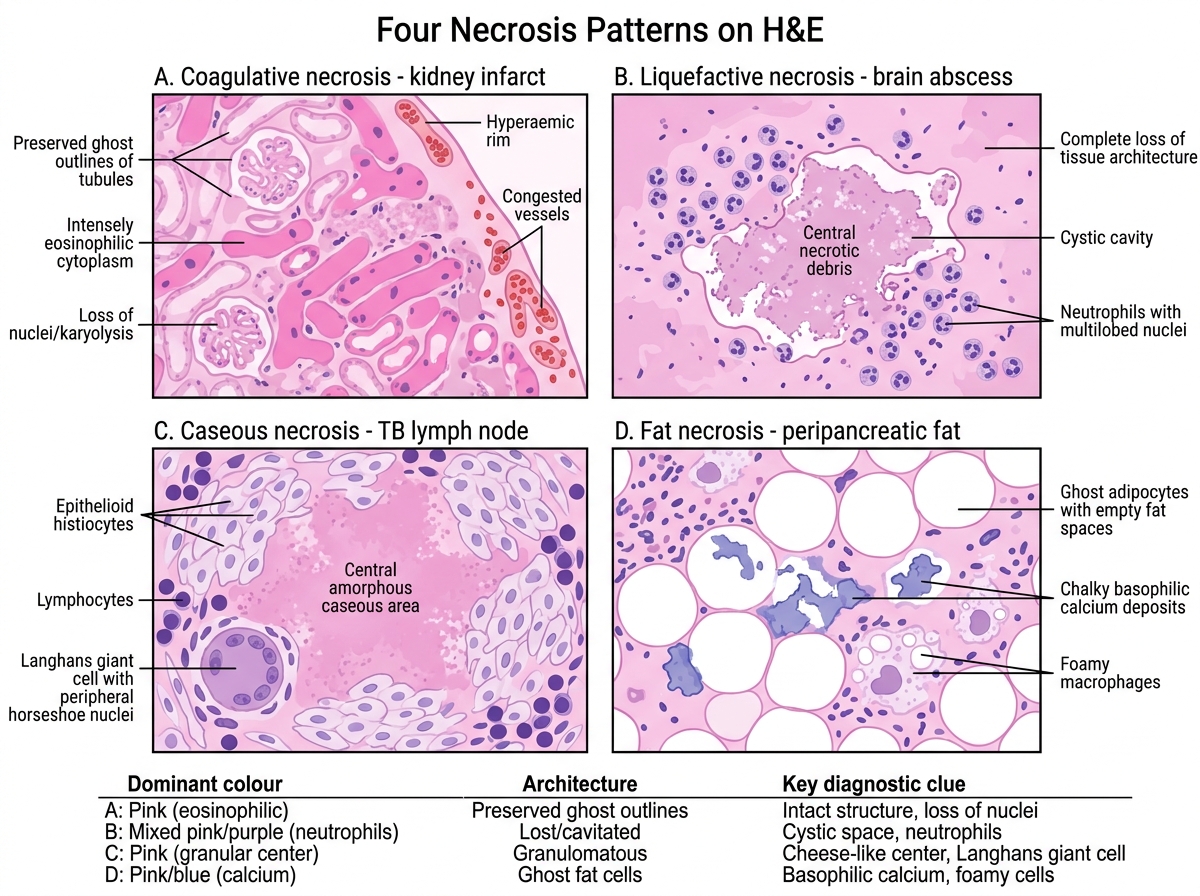
The four main necrosis patterns are best learned side-by-side. The following composite photomicrograph (H&E, all panels at equivalent magnification ~10×) displays one pattern per panel:
- Panel A — Coagulative necrosis (kidney infarct): ghost tubular outlines, eosinophilic, karyolysis, hyperaemic rim
- Panel B — Liquefactive necrosis (brain abscess): cystic cavity, neutrophils, no residual architecture
- Panel C — Caseous necrosis (TB lymph node): amorphous eosinophilic debris, epithelioid granuloma, Langhans cell
- Panel D — Fat necrosis (peripancreatic fat): ghost adipocytes, basophilic Ca²⁺ deposits, foam cells
For each panel: (1) name the dominant staining colour; (2) state whether architecture is preserved or destroyed; (3) name the key diagnostic cell or structure.
Four Major Patterns of Necrosis
SELF-CHECK
In the 2×2 grid above, Panel D (fat necrosis) differs from all three other panels in one specific staining characteristic. What is it?
A. It is the only panel showing predominantly basophilic (blue) deposits rather than eosinophilic material
B. It is the only panel with nuclear pyknosis rather than karyolysis
C. It is the only panel that retains recognisable tissue architecture with ghost outlines
D. It is the only panel that shows infiltrating neutrophils as the primary cell
Reveal Answer
Answer: A. It is the only panel showing predominantly basophilic (blue) deposits rather than eosinophilic material
Calcium soaps formed by saponification stain basophilic (blue/purple) on H&E — the only necrosis pattern where basophilia is a primary diagnostic feature. All other types produce eosinophilic debris. Ghost adipocyte outlines are present but the key staining signature is the basophilic calcification, not the outlines.
Gross Specimen Recognition: Infarcts and Gangrene
Gross Recognition of Infarcts and Gangrene
Gross pattern recognition is tested in the spotting practical and in viva. Know these cold:
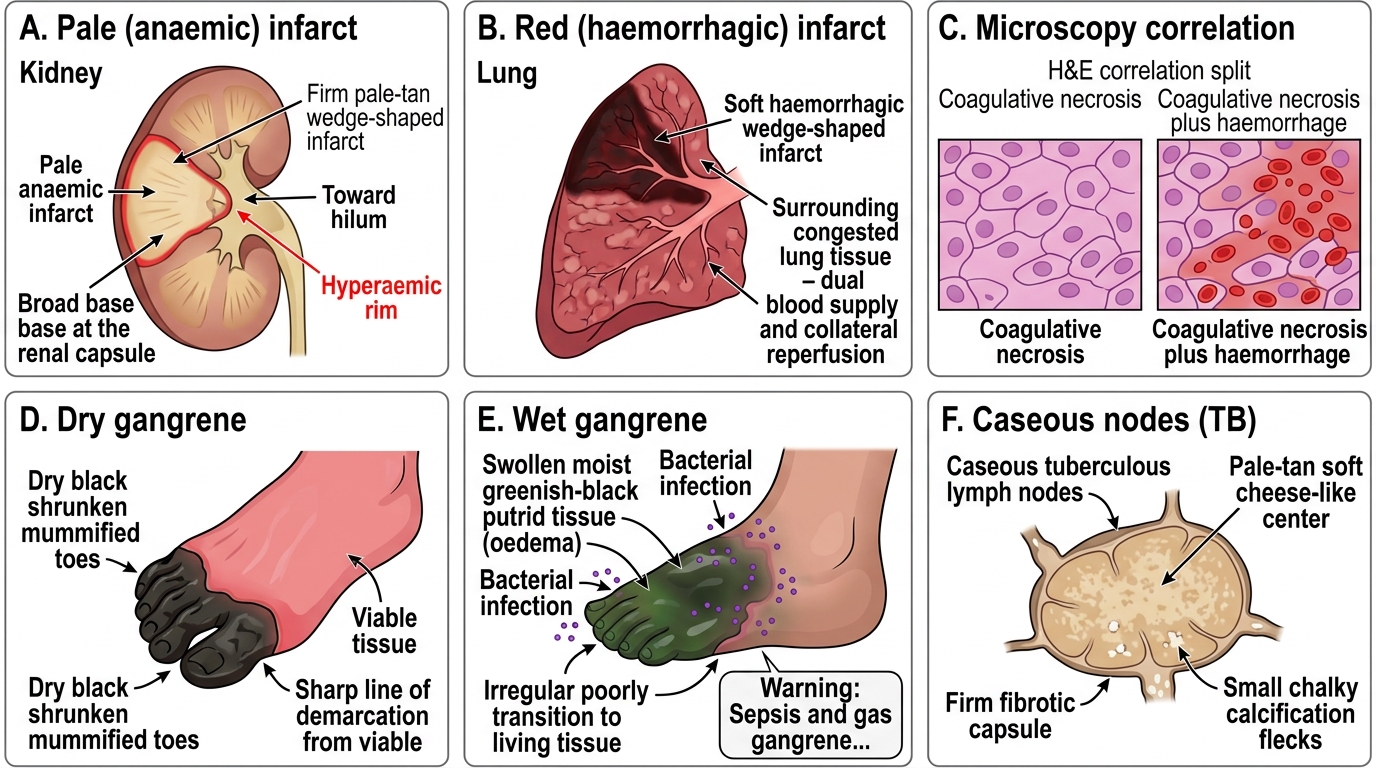
Pale (anaemic) infarct:
• Organs: kidney, heart, spleen (solid, end-arterial)
• Gross: firm, pale-tan or yellow-white, wedge-shaped with apex toward the hilum, base toward capsule
• Hyperaemic rim at boundary (reactive vasodilation)
• Correlates with: coagulative necrosis on H&E
Red (haemorrhagic) infarct:
• Organs: lung (dual blood supply), bowel (reperfusion), testis (loose parenchyma)
• Gross: dark red-black, soft, haemorrhagic, wedge-shaped
• Mechanism: blood re-enters necrotic zone from collateral or dual supply
• Correlates with: coagulative necrosis + haemorrhage on H&E
Dry gangrene:
• Ischaemic coagulative + mummification; toes/foot in diabetic/atherosclerotic ischaemia
• Gross: dry, black, shrunken, sharply demarcated line of separation from living tissue
Wet gangrene:
• Superimposed bacterial infection → liquefactive component
• Gross: swollen, moist, putrid, greenish-black, foul-smelling, no clear line
• Emergency: risk of sepsis, gas gangrene (Clostridium)
Caseous nodes (TB):
• Matted lymph nodes, pale-tan soft cheese-like centre, firm fibrotic capsule, may be calcified
SELF-CHECK
A surgeon excises a gangrenous toe from a 68-year-old with longstanding type 2 diabetes and peripheral artery disease. The amputated toe is dry, black, shrunken, with a sharply demarcated line of separation. What is the MOST accurate pathological classification?
A. Wet gangrene with superimposed Clostridium infection
B. Dry gangrene — ischaemic coagulative necrosis with mummification, no secondary infection
C. Liquefactive necrosis following arterial embolism
D. Caseous necrosis due to atypical mycobacterial infection in a diabetic
Reveal Answer
Answer: B. Dry gangrene — ischaemic coagulative necrosis with mummification, no secondary infection
Dry gangrene is coagulative necrosis caused by gradual ischaemia (atherosclerosis, diabetes) without superimposed infection. The tissue mummifies — loses moisture, shrivels, turns black due to haemoglobin breakdown products. The sharp line of demarcation is characteristic. Wet gangrene is moist, swollen, malodorous and lacks a clear margin because of bacterial invasion.
Apoptotic Bodies, Pigments and Dystrophic Calcification on H&E
Three additional H&E findings complete the practical checklist for cell injury:
Apoptotic bodies:
• Small, round, deeply eosinophilic cytoplasmic fragments with condensed nuclear material (pyknotic fragments)
• Scattered individually — no surrounding inflammatory response (key distinction from necrosis)
• Membrane-bound: content is phagocytosed by neighbouring cells → no 'leakage'
• Seen in: viral hepatitis (Councilman bodies = apoptotic hepatocytes), graft rejection, ischaemia
Common pigments on H&E:
• Haemosiderin — golden-brown granular intracellular pigment; Perls' Prussian Blue stain confirms iron
• Lipofuscin — yellow-brown granular 'wear-and-tear' pigment; perinuclear in cardiac/liver cells
• Melanin — brown-black, in melanocytes and melanophages
• Bile (bilirubin) — green-brown intracanalicular or intracytoplasmic plugs in cholestasis
Dystrophic calcification:
• Basophilic (blue/purple) granular or laminated deposits in areas of necrosis or old inflammatory foci
• Occurs in dead or dying tissue at normal serum calcium levels
• Examples: TB caseous foci, atherosclerotic plaques, old infarcts, psammoma bodies in papillary carcinoma
• Distinguish from metastatic calcification (same appearance, but in viable tissue, due to hypercalcaemia)
Four Necrosis Patterns at a Glance
CLINICAL PEARL
'No inflammation' is the clinical and microscopic signature of apoptosis. When you see an isolated eosinophilic body with no surrounding neutrophils or macrophages, think apoptosis — not necrosis. This distinction matters in practice: necrosis triggers inflammation (and fever, raised CRP); apoptosis does not. In viral hepatitis, you may see both: scattered Councilman bodies (apoptosis) alongside focal necrosis and portal inflammation. Reporting both accurately changes the grade of hepatitis.
SELF-CHECK
A liver biopsy from a patient with acute hepatitis B shows scattered small, round, deeply eosinophilic bodies in the sinusoids with no surrounding inflammatory infiltrate. Nearby hepatocytes appear intact. These bodies are BEST described as:
A. Mallory-Denk bodies — indicative of alcoholic liver disease
B. Lipofuscin granules — age-related wear-and-tear pigment
C. Councilman bodies — apoptotic hepatocytes, confirmed by absence of perilesional inflammation
D. Haemosiderin deposits — iron overload from haemochromatosis
Reveal Answer
Answer: C. Councilman bodies — apoptotic hepatocytes, confirmed by absence of perilesional inflammation
Councilman (acidophil) bodies are the classical term for apoptotic hepatocytes seen in viral hepatitis. They are small, round, densely eosinophilic, membrane-bound fragments with condensed nuclear debris. The defining feature is the absence of surrounding inflammatory cells — because apoptotic contents do not 'leak' and do not trigger the DAMP/PAMP pattern-recognition cascade. Mallory-Denk bodies are irregular eosinophilic cytoplasmic inclusions in alcoholic hepatocytes, not rounded isolated fragments.
Putting It Together: A Diagnostic Checklist
Diagnostic Checklist for Cell Injury Specimens
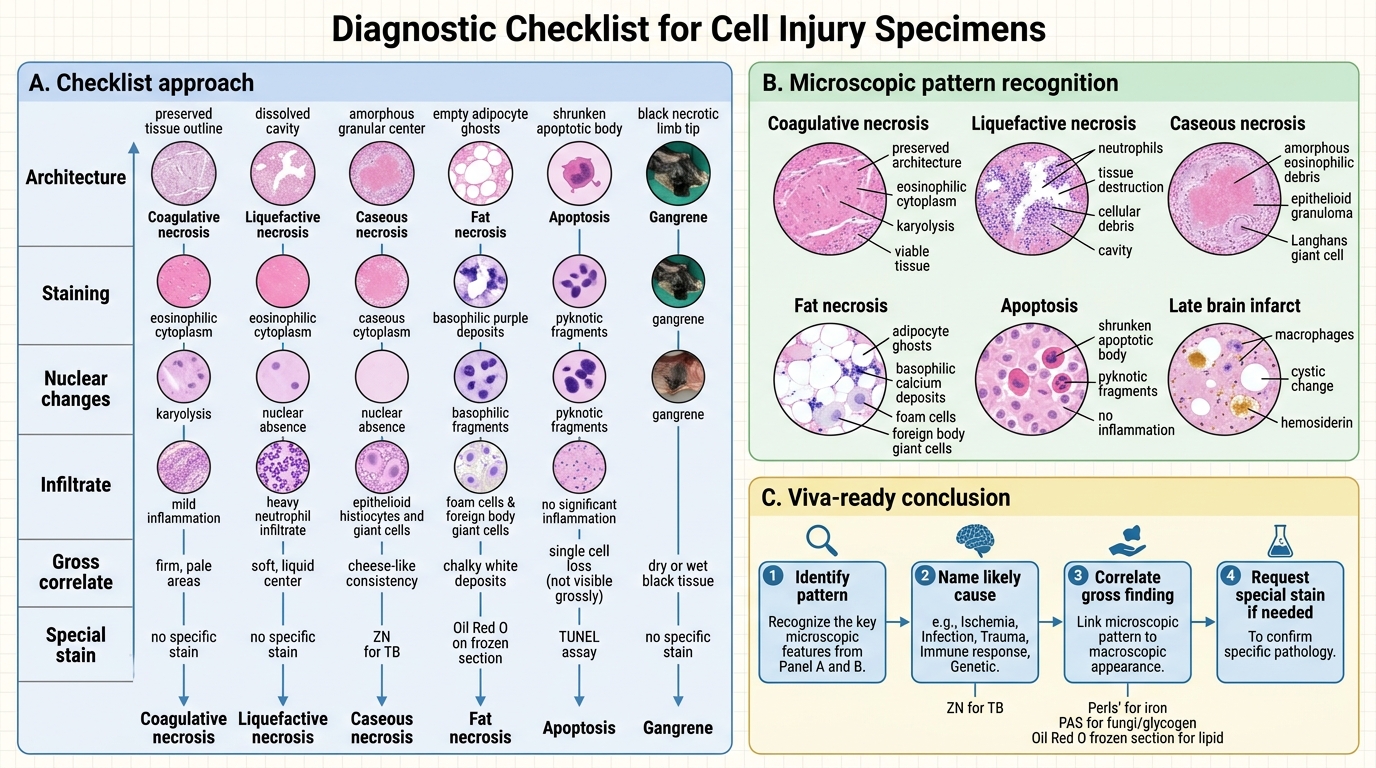
Use this checklist for any cell-injury specimen in the practical:
| Feature | Ask yourself |
|---|---|
| Architecture | Preserved (coagulative) / Destroyed (liquefactive, caseous) / Absent — adipocytes only (fat necrosis) |
| Staining | Eosinophilic debris (most) / Basophilic deposits (fat necrosis calcification, dystrophic Ca²⁺) |
| Nuclear changes | Karyolysis dominant (coagulative) / No nuclei (caseous, fat necrosis) / Pyknotic fragments (apoptosis) |
| Infiltrate | Neutrophils (bacterial liquefactive) / Epithelioid granuloma + Langhans cells (caseous) / Foam cells + giant cells (fat necrosis) / None (apoptosis) / Macrophages (late brain infarct) |
| Gross correlate | Pale wedge (coagulative infarct) / Cystic (liquefactive brain) / Cheese-like (caseous TB) / Chalk-marks (fat necrosis) / Black dry/wet (gangrene) |
| Special stain if needed | ZN (TB) / Perls' (iron) / PAS (fungi, glycogen) / Oil Red O frozen (lipid) |
In your write-up or viva: state (1) type of necrosis, (2) extent, (3) probable aetiology, (4) one special stain that would confirm.