Page 12 of 24
PA2.{3,6-7} | Cellular Adaptations, Accumulations & Aging — SDL Guide (Part 4)
Apoptosis in Context — Programmed Cell Death vs Pathological Death
Apoptosis in Context: Programmed Cell Death vs Necrosis
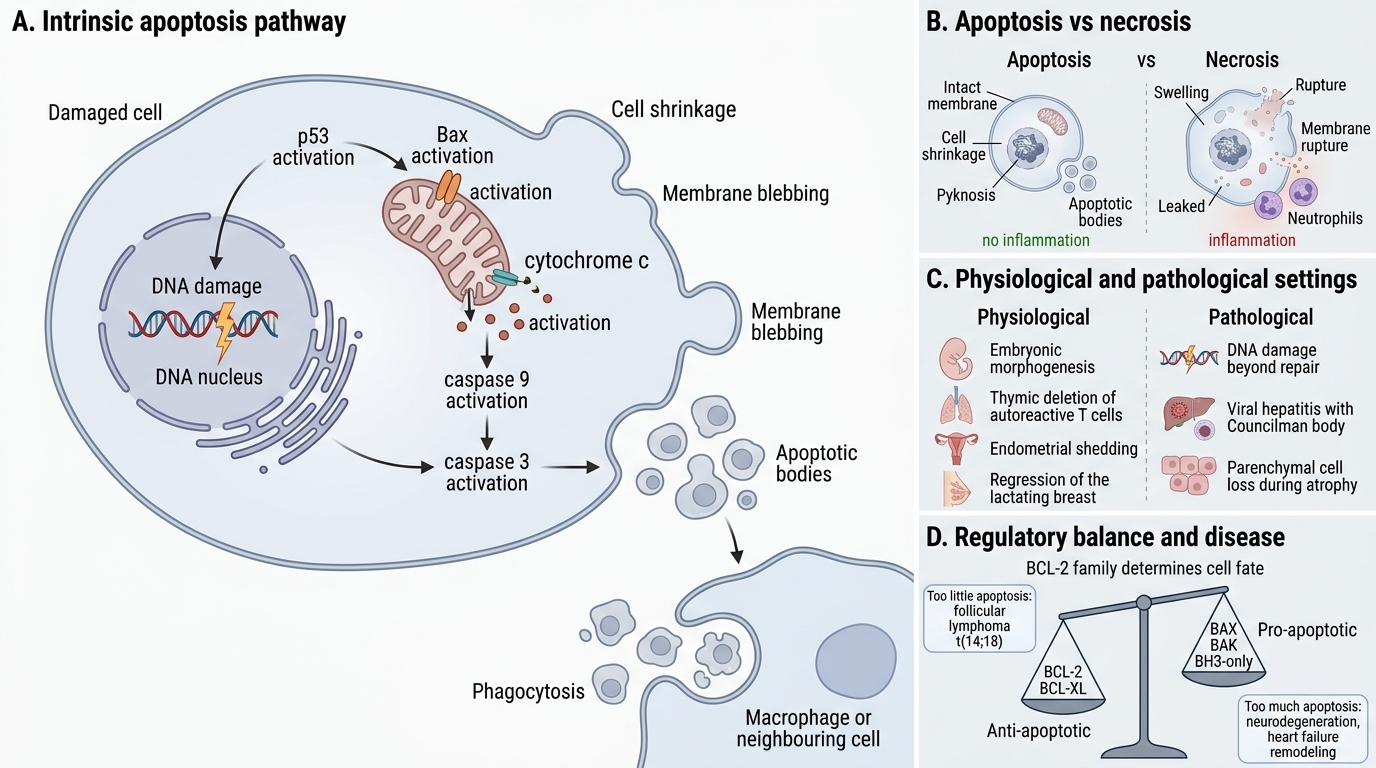
Apoptosis (PA2.7) is programmed cell death — an active, energy-requiring, genetically directed process eliminating unwanted or damaged cells without inflammation.
Physiological apoptosis: embryonic morphogenesis, deletion of autoreactive T cells in thymus, endometrial shedding in menstruation, regression of the lactating breast.
Pathological apoptosis: DNA damage beyond repair (p53 activates Bax → cytochrome c release → caspase 9 → caspase 3 cascade), viral infection (e.g., Councilman bodies in yellow fever hepatitis), parenchymal cell loss in atrophy.
Morphology: Cell shrinkage, chromatin condensation (pyknosis) and margination, cytoplasmic blebbing → formation of apoptotic bodies (membrane-bound fragments phagocytosed by neighbours and macrophages). No inflammation because membrane remains intact — contrast with necrosis.
Key regulators: Anti-apoptotic (BCL-2, BCL-XL) vs pro-apoptotic (BAX, BAK, BH3-only proteins). The ratio determines the cell's fate.
Dysregulation: Too little apoptosis → cancer (BCL-2 overexpression in follicular lymphoma t(14;18)). Too much apoptosis → neurodegeneration, cardiac remodelling in heart failure.
SELF-CHECK
Which of the following correctly distinguishes apoptosis from necrosis?
A. Apoptosis involves membrane rupture and inflammatory cell infiltration
B. Necrosis is an active, ATP-dependent, genetically programmed process
C. Necrosis causes chromatin condensation and cell shrinkage as early features
D. Apoptosis produces membrane-bound apoptotic bodies phagocytosed without inflammation
Reveal Answer
Answer: D. Apoptosis produces membrane-bound apoptotic bodies phagocytosed without inflammation
Apoptosis produces membrane-bound apoptotic bodies that are phagocytosed by adjacent cells and macrophages. Because the plasma membrane remains intact until phagocytosis, lysosomal contents are never released into the ECM, so there is no inflammatory response. Necrosis involves membrane rupture, lysosomal enzyme release, and a florid neutrophilic inflammation. Chromatin condensation (pyknosis) is a feature of apoptosis, not necrosis.
CLINICAL PEARL
Telomere biology connects ageing, cancer, and bone marrow failure syndromes. In dyskeratosis congenita (mutant dyskerin → short telomeres), patients develop bone marrow failure, oral leukoplakia, and nail dystrophy in the second or third decade — premature ageing of rapidly dividing tissues. Conversely, cancer cells reactivate telomerase to escape senescence, achieving replicative immortality. This is why anti-telomerase strategies are being explored as cancer therapeutics.