Page 1 of 24
PA1.1-3,PA2.1-2 | Introduction to Pathology & Mechanisms of Cell Injury — SDL Guide
Learning Objectives
- Define pathology and describe its four core aspects: etiology, pathogenesis, morphologic changes, and clinical significance.
- Differentiate the roles of anatomic and clinical pathology; explain the pathologist's contribution to patient care.
- Recall key terms in the history and evolution of pathology from Virchow's era to molecular diagnostics.
- Describe cell-cycle phases and classify tissues by proliferative capacity (labile, stable, permanent).
- List the major causes and common biochemical mechanisms of cell injury.
- Distinguish reversible from irreversible cell injury on morphological and functional grounds.
- Explain ischaemia-reperfusion injury and its clinical relevance.
INSTRUCTIONS
Pathology is the scientific bridge between basic sciences and clinical medicine — it explains why and how diseases happen. In Year 2 you will use these principles daily: every biopsy report, every autopsy finding, every lab value links back to the concepts in this module. Work through each section actively; the micro-quizzes and reflection prompts are checkpoints, not optional extras.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 1–2 (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 1 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
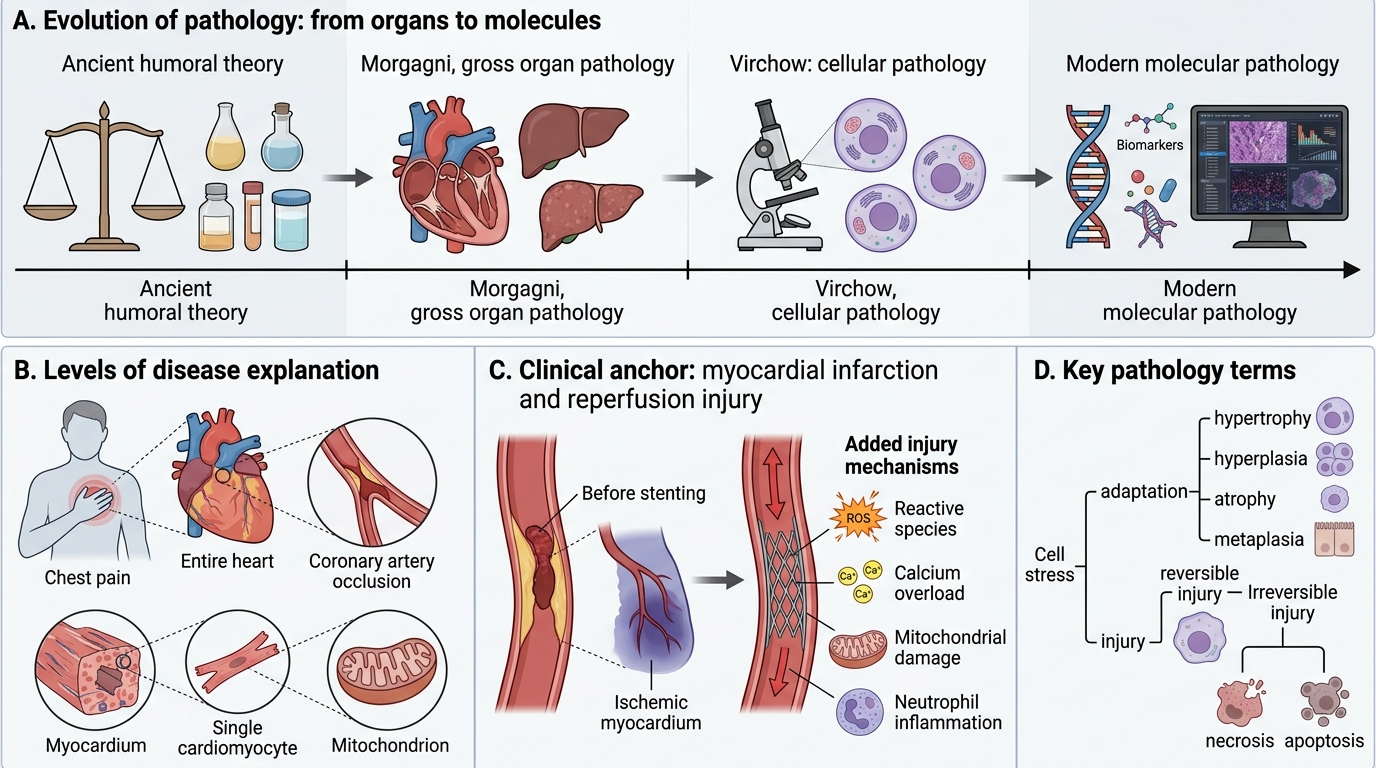
A 52-year-old man is rushed to the emergency department with crushing chest pain. His ECG shows ST elevation. Cardiology opens the blocked coronary artery with a stent — but 48 hours later, imaging reveals a zone of dead myocardium larger than expected. The cardiologist asks: Why did more muscle die after blood flow was restored?
The answer lies in the biology of cell injury. By the end of this module, you will understand exactly what happened to those heart-muscle cells — and why timing matters more than almost anything else in medicine.
WHY THIS MATTERS
Every clinical decision in medicine — ordering a biopsy, interpreting a blood count, staging a cancer, choosing a drug — rests on an understanding of how cells respond to injury. Pathology is not a laboratory discipline detached from the ward: the pathologist who reads the frozen section during your surgical procedure, the haematologist who examines the peripheral smear, the microbiologist who identifies the organism — all practise pathology in real time. Understanding the mechanisms of cell injury is also directly assessed in University and MCI/NMC licensing examinations.
RECALL
Before continuing, briefly revisit the following Year-1 concepts:
- ATP synthesis — glycolysis vs. oxidative phosphorylation; the role of mitochondria.
- Membrane lipid bilayer — phospholipids, cholesterol, membrane protein channels (especially Ca²⁺ and Na⁺/K⁺-ATPase).
- Free radicals — from biochemistry: what makes a molecule a radical, and why superoxide dismutase matters.
- Cell cycle checkpoints — G1/S and G2/M restriction points; cyclins and CDKs.
If any of these feel uncertain, a 5-minute review of your Year-1 biochemistry notes now will make the rest of this module much clearer.
What Is Pathology? The Four Aspects of Disease
Four Aspects of Disease in Pathology
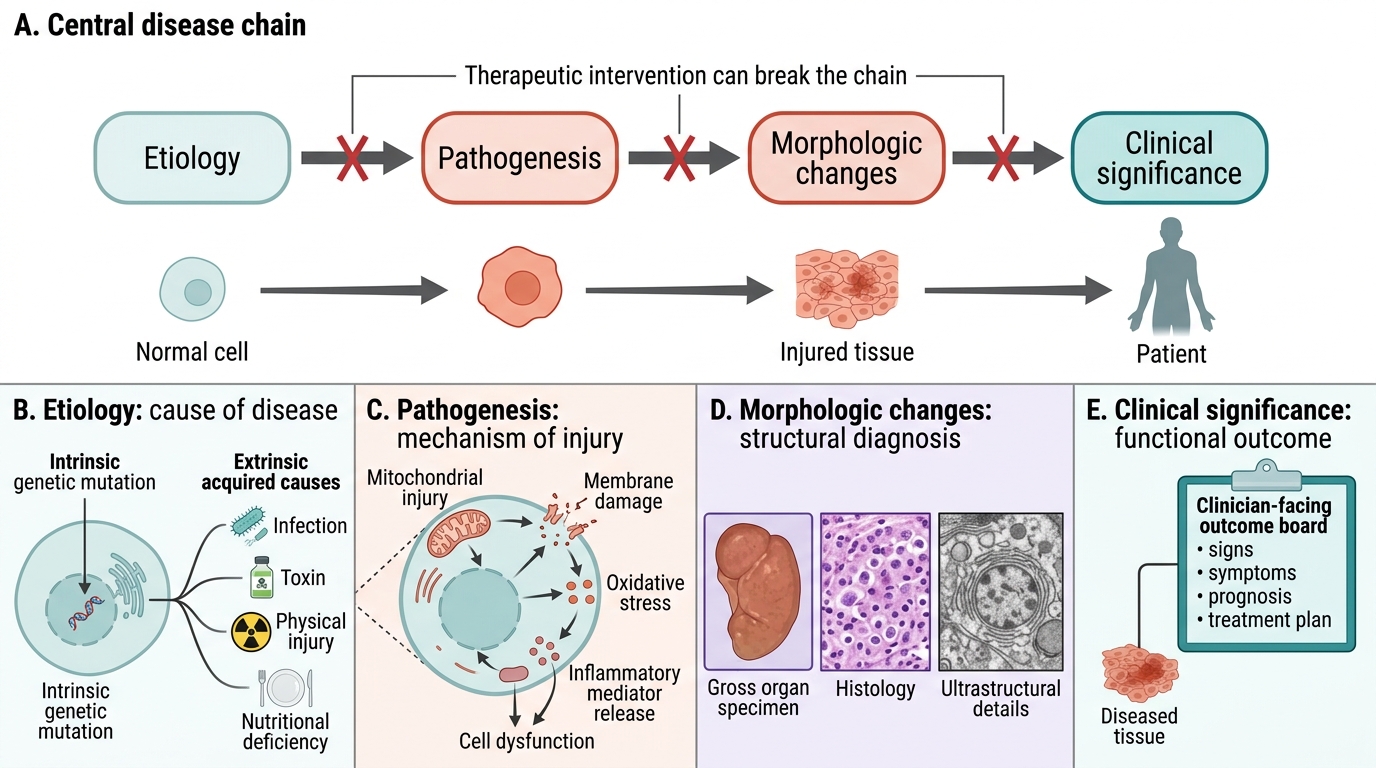
Pathology (Greek pathos — suffering; logos — study) is the scientific study of the structural, biochemical, and functional changes in cells, tissues, and organs that underlie disease. Every disease can be understood through four interconnected aspects:
- Etiology — the cause of disease. Causes may be genetic (intrinsic) or acquired (extrinsic: infections, toxins, physical agents, nutritional deficiencies).
- Pathogenesis — the mechanism by which the etiological agent produces disease; the sequence of cellular and molecular events from stimulus to the final expression of illness.
- Morphologic changes — the structural alterations in cells and tissues visible at gross, histological, or ultrastructural level; these are the diagnostic signatures of disease.
- Clinical significance — the functional consequences: signs, symptoms, prognosis, and the basis for treatment.
Think of these four aspects as a chain: etiology triggers pathogenesis, which produces morphologic changes, which generate clinical disease. Breaking any link breaks the disease process — and that is the rationale for every therapeutic intervention.
The Pathologist: Anatomic vs. Clinical Pathology
The Pathologist: Anatomic vs Clinical Pathology
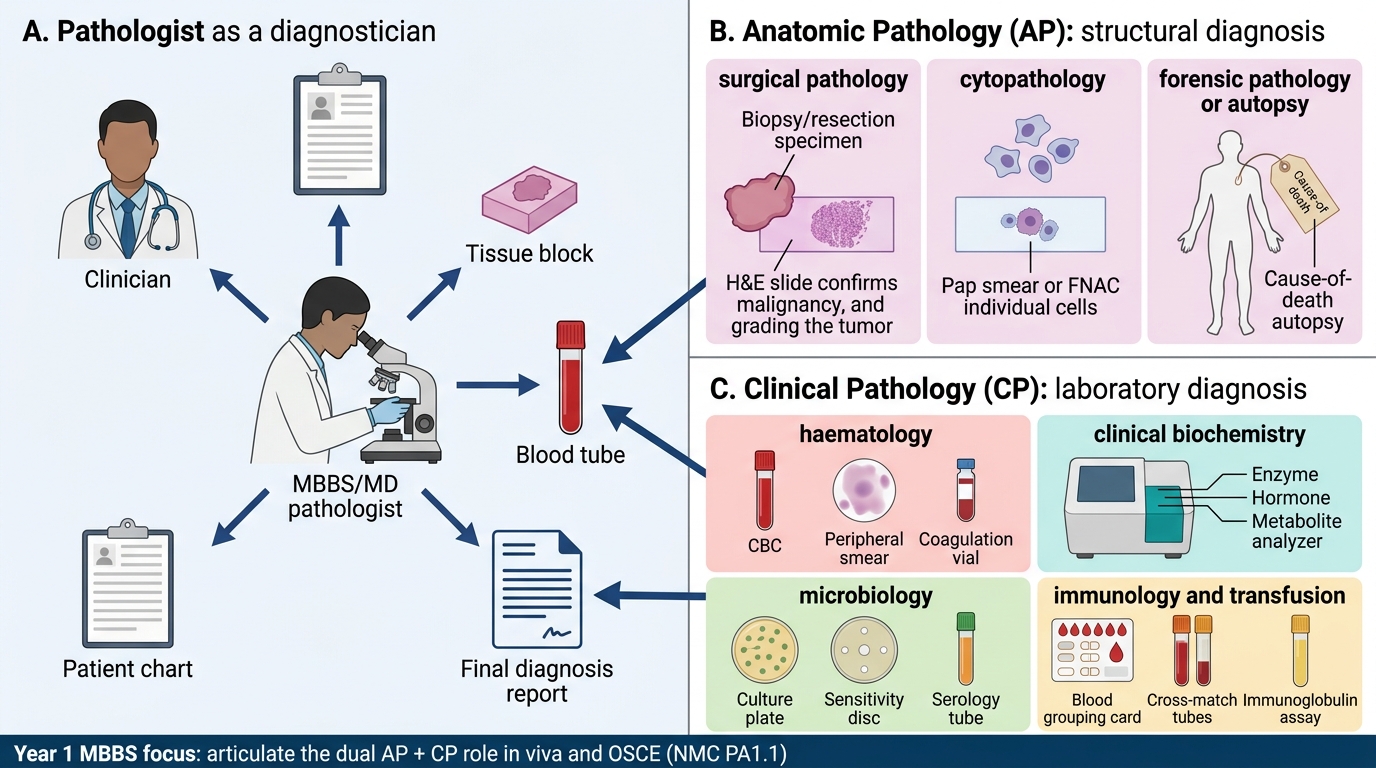
The pathologist occupies a unique position in the healthcare system: they are diagnosticians who work primarily with tissues and fluids, providing the definitive diagnosis that guides clinical management.
Anatomic pathology (AP) deals with structural examination:
- Surgical pathology — biopsy, resection specimen analysis (e.g., confirming malignancy, grading tumours).
- Cytopathology — examination of individual cells (Pap smear, FNAC, sputum cytology).
- Forensic pathology / autopsy — cause-of-death determination; quality control for clinical diagnosis.
Clinical pathology (CP) encompasses laboratory-based disciplines:
- Haematology — CBC, peripheral smear, coagulation studies.
- Clinical biochemistry — enzymes, hormones, metabolites.
- Microbiology — culture, sensitivity, serology.
- Immunology / transfusion medicine — blood grouping, cross-matching, immunoglobulin assays.
In India, the MBBS graduate rotates through both AP and CP during Year 2; the MD Pathology specialist integrates both. The NMC CBUC (PA1.1) expects you to articulate this dual role clearly in clinical viva and OSCEs.
History & Key Terms in the Evolution of Pathology
Pathology: From Organ Lesions to Cell Injury Mechanisms
Understanding how pathology evolved helps contextualise its current molecular focus.
| Era | Milestone | Significance |
|---|---|---|
| Ancient–Renaissance | Gross anatomy (Vesalius, 1543) | Structural descriptions; disease = humoral imbalance |
| 18th c. | Morgagni De Sedibus (1761) | Disease linked to organ lesions (organ pathology) |
| 19th c. | Rudolf Virchow (1858): Omnis cellula e cellula | Cell = unit of disease; birth of cellular pathology |
| Late 19th c. | Koch, Pasteur | Germ theory; infectious etiology |
| 20th c. | Electron microscopy, immunohistochemistry | Ultrastructural and antigen-based diagnosis |
| 21st c. | Genomics, proteomics, liquid biopsy | Molecular and precision pathology |
Key terms you must define fluently:
- Lesion — any pathological change in a tissue.
- Aetiology vs. pathogenesis — cause vs. mechanism (distinct concepts, often confused in exams).
- Morbidity — extent or burden of disease.
- Mortality — death rate.
- Sequela — a condition that is a consequence of a disease or injury.
- Iatrogenic disease — disease caused by medical treatment.
SELF-CHECK
Virchow's principle Omnis cellula e cellula established which foundational concept in pathology?
A. Disease originates from imbalance of the four humours
B. The cell is the basic unit of life and the seat of disease
C. Microorganisms are the primary cause of all disease
D. Morphological changes always precede biochemical changes
Reveal Answer
Answer: B. The cell is the basic unit of life and the seat of disease
Virchow's 1858 doctrine — 'every cell from a pre-existing cell' — shifted pathological thinking from organ-level descriptions (Morgagni) to cellular pathology, establishing the cell as the fundamental unit in which disease originates. Options A (humoral theory) predates Virchow; C (germ theory) is Koch/Pasteur; D inverts the actual sequence.