Page 1 of 25
PA3.1-2 | Acute Inflammation — Vascular & Cellular Events, Mediators — SDL Guide
Learning Objectives
- Define acute inflammation and describe its biological purpose.
- Identify the five cardinal signs of acute inflammation and explain their cellular and vascular basis.
- Outline the sequence of vascular events: vasoconstriction, vasodilation, increased permeability, stasis, and exudate formation.
- Describe the leucocyte recruitment cascade — margination, rolling, adhesion, transmigration, and chemotaxis.
- Explain the mechanisms of phagocytosis including opsonisation, engulfment, and microbicidal killing (oxygen-dependent and -independent).
- Identify the major chemical mediators of acute inflammation and link each to its source and primary action.
- Classify the morphological patterns of acute inflammation (serous, fibrinous, suppurative, ulcerative) with clinical examples.
- List the possible outcomes of acute inflammation.
INSTRUCTIONS
Inflammation is the body's first line of defence — understanding it explains fever, wound healing, pus formation, and the mechanism of virtually every anti-inflammatory drug. This module builds a mechanistic map of acute inflammation from the first vascular twitch to the fate of the exudate. By the end, the cardinal signs, leucocyte trafficking cascade, and mediator pharmacology will form an integrated picture you can apply to any inflammatory condition.
References
- Robbins & Kumar: Basic Pathology, 11th ed., Ch 2 (Acute and Chronic Inflammation) (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 5 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You stub your toe. Within seconds the area turns red, swells, feels hot, throbs with pain, and you limp. Five ancient Latin words capture this perfectly. What is the molecular storm behind those five seconds — and why does your body trigger it at all?
WHY THIS MATTERS
Acute inflammation underpins the pathogenesis of infections, surgical wounds, myocardial infarction, appendicitis, and allergic reactions. NSAIDs, corticosteroids, and antihistamines — the most-prescribed drug classes in clinical practice — all target mediators you will map in this module. Understanding this cascade lets you reason about drug mechanisms, predict complications like abscess or chronic inflammation, and interpret histopathology reports.
RECALL
Before proceeding, recall from Year-1:
• Cells of the innate immune system (neutrophils, macrophages, mast cells, eosinophils).
• Basic structure of blood vessels (endothelium, basement membrane).
• Complement system: classical vs. alternative pathway, and the terminal membrane-attack complex.
• Arachidonic acid as a membrane phospholipid precursor.
This module builds directly on those foundations.
Definition and Purpose of Inflammation
Definition and Purpose of Inflammation
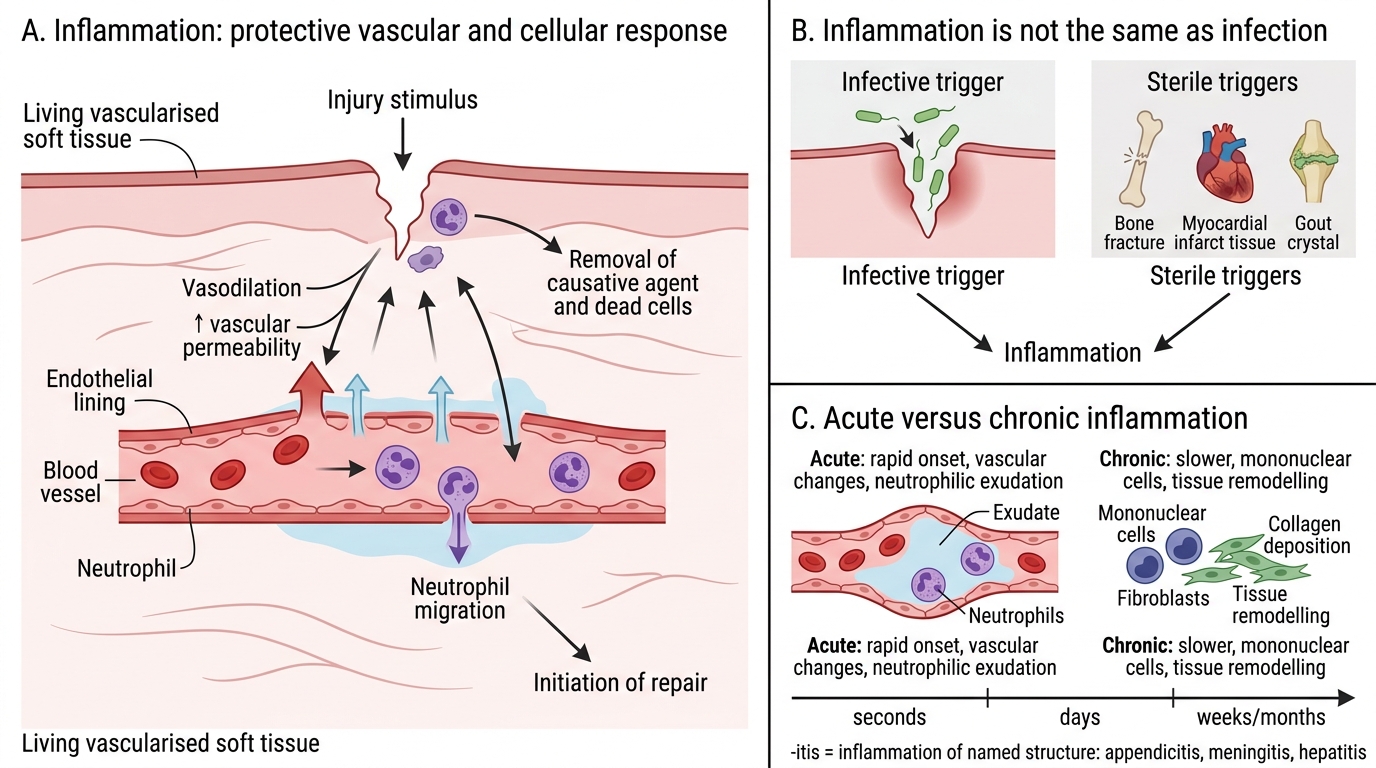
Inflammation is a protective vascular and cellular response of living vascularised tissue to injury, infection, or abnormal stimuli, aimed at eliminating the causative agent, clearing dead cells, and initiating repair.
It is not synonymous with infection — sterile injury (e.g., a bone fracture, myocardial infarct, gout crystals) triggers identical mechanisms. The suffix -itis denotes inflammation of the named structure (appendicitis, meningitis, hepatitis).
Acute inflammation is rapid in onset (seconds to days), characterised by vascular changes and neutrophilic exudation. Chronic inflammation is slower, dominated by mononuclear cells and tissue remodelling — covered in a subsequent module (PA3.1, chronic portion).
> Clinical pearl link: Recognising that inflammation can be sterile is essential when reading postoperative or post-infarction histology reports that describe 'inflammation' without implying infection.
The Five Cardinal Signs and Their Basis
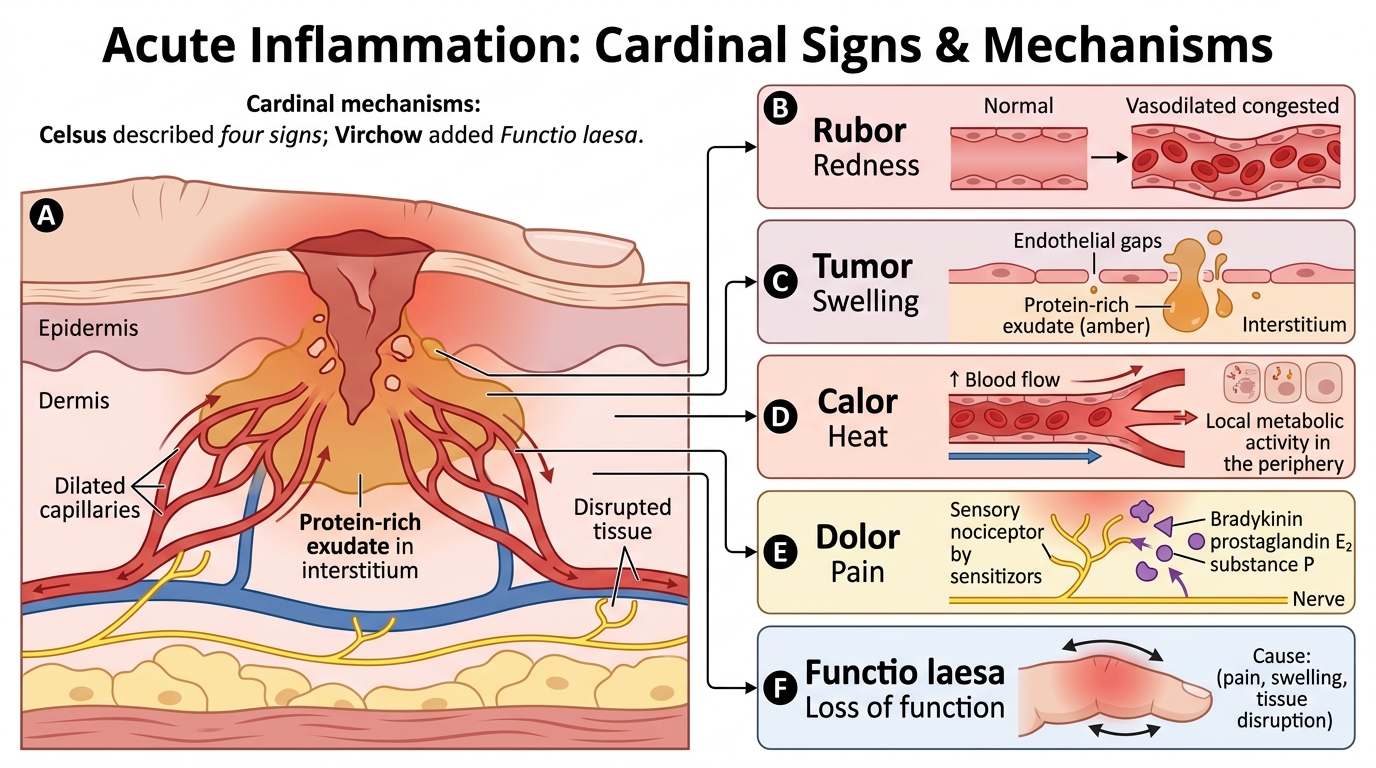
Celsus (1st century CE) described four signs; Virchow added a fifth:
| Latin term | English | Mechanism |
|---|---|---|
| Rubor | Redness | Vasodilation → ↑blood flow → congestion |
| Tumor | Swelling | ↑Vascular permeability → protein-rich exudate in interstitium |
| Calor | Heat | ↑Blood flow (systemic temp. blood to periphery) + local metabolic activity |
| Dolor | Pain | Bradykinin, prostaglandin E₂, and substance P sensitise nociceptors |
| Functio laesa | Loss of function | Combined effect of pain, swelling, and tissue disruption |
Each sign maps to a specific vascular or mediator event explored in the blocks below.
Five Cardinal Signs of Inflammation
SELF-CHECK
Which cardinal sign of acute inflammation is PRIMARILY explained by increased vascular permeability rather than vasodilation?
A. Rubor (redness)
B. Calor (heat)
C. Tumor (swelling)
D. Dolor (pain)
Reveal Answer
Answer: C. Tumor (swelling)
Tumor (swelling) results from protein-rich fluid (exudate) leaking into the interstitium due to increased vascular permeability. Rubor and calor are primarily due to vasodilation increasing blood flow. Dolor involves sensitisation of nociceptors by prostaglandins and bradykinin.
Vascular Events: The Haemodynamic Response
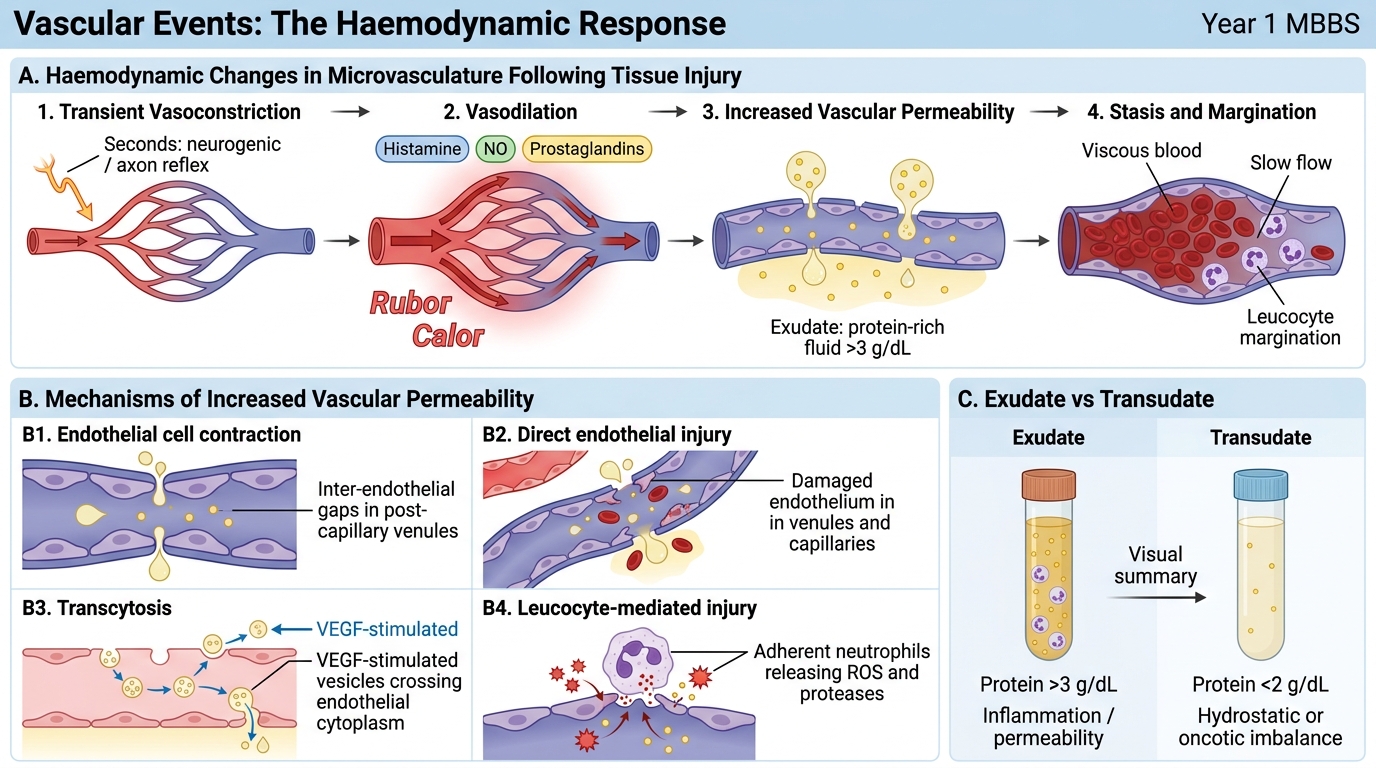
The vascular response unfolds in a precise sequence following injury:
1. Transient vasoconstriction (seconds): neurogenic reflex via axon reflex; very brief and clinically imperceptible.
2. Vasodilation (lasting): arterioles dilate first, then capillary bed opens. Mediators: histamine, nitric oxide (NO), and prostaglandins. Result: ↑blood flow → rubor + calor.
3. Increased vascular permeability: allows protein-rich fluid (>3 g/dL protein) to leak — forming exudate. Mechanisms:
• Endothelial cell contraction (most common) — histamine and leukotrienes cause cytoskeletal contraction, widening inter-endothelial gaps. Affects venules. Immediate, transient or delayed/prolonged.
• Direct endothelial injury — e.g., burns, caustic agents. Affects venules and capillaries. Immediate and sustained.
• Transcytosis — VEGF-stimulated vesicular transport through endothelial cytoplasm (important in tumours and chronic states).
• Leucocyte-mediated injury — ROS and proteases from adherent neutrophils damage endothelium.
4. Stasis: as fluid leaves the vessel, blood becomes viscous; flow slows. Leucocytes move to the vessel periphery (margination).
Exudate vs. transudate distinction (tested frequently):
| Exudate | Transudate | |
|---|---|---|
| Protein | >3 g/dL | <2 g/dL |
| Specific gravity | >1.020 | <1.012 |
| Mechanism | Active inflammation (↑permeability) | Hydrostatic/oncotic imbalance |
| Example | Pleural empyema | Cardiac failure effusion |
Haemodynamic Response in Acute Inflammation