Page 4 of 25
PA3.1-2 | Acute Inflammation — Vascular & Cellular Events, Mediators — SDL Guide (Part 4)
Complement Fragments and the Kinin System
Complement Fragments and the Kinin System
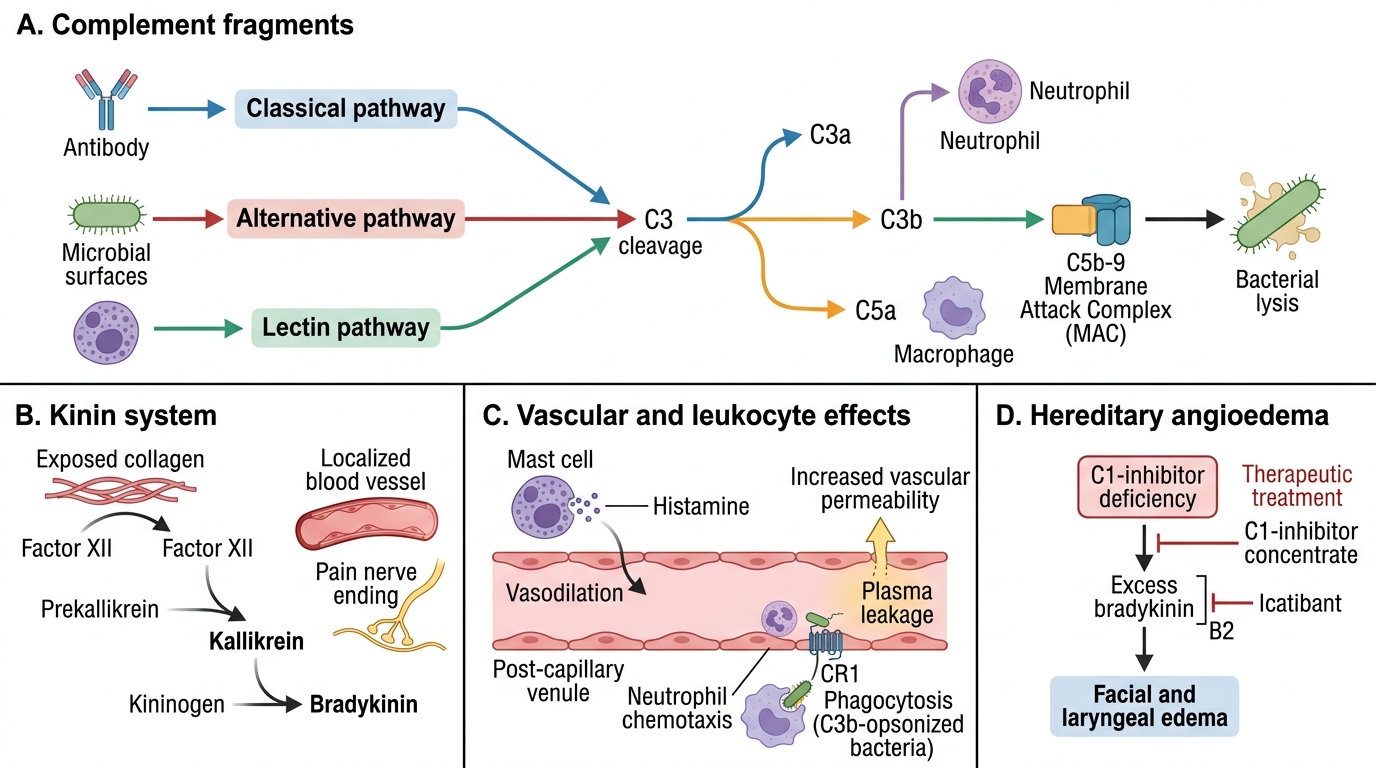
Complement system:
Activated via classical (antibody), alternative (microbial surfaces), or lectin pathways → converge at C3 cleavage:
- C3a and C5a (anaphylatoxins): bind mast cell/basophil receptors → histamine release → vasodilation + ↑permeability.
- C5a (more potent): also a chemotactic agent for neutrophils; activates neutrophils (↑adhesion, respiratory burst).
- C3b: opsonin — coats bacteria for enhanced phagocytosis via CR1.
- Membrane-attack complex (C5b-9, MAC): direct lysis of bacteria; also activates endothelium/platelets (↑mediator release).
Kinin system:
• Hageman factor (Factor XII) activated by exposed collagen → activates prekallikrein → kallikrein → cleaves kininogen → bradykinin.
• Bradykinin: ↑Vascular permeability; vasodilation; pain (acts on B₂ receptors on nociceptors — a major mediator of inflammatory pain).
• Short-lived: rapidly inactivated by kininases.
• Kallikrein also activates complement and plasmin.
> Hereditary angioedema is caused by C1-inhibitor deficiency → uncontrolled bradykinin generation → recurrent episodes of oedema, laryngeal swelling (potentially fatal). Treatment: C1-inhibitor concentrate or icatibant (B₂ receptor antagonist).
SELF-CHECK
A patient with asthma receives montelukast. Which inflammatory mediator action does this drug primarily block?
A. Histamine-induced endothelial contraction
B. LTD₄-mediated bronchoconstriction and increased permeability
C. PGE₂-induced fever and hyperalgesia
D. TNF-mediated upregulation of endothelial adhesion molecules
Reveal Answer
Answer: B. LTD₄-mediated bronchoconstriction and increased permeability
Montelukast is a cysteinyl leukotriene receptor (CysLT1) antagonist. Cysteinyl leukotrienes (LTC₄, LTD₄, LTE₄) — formed via the 5-LOX pathway from arachidonic acid — are potent bronchoconstrictors and increase vascular permeability. They constitute the slow-reacting substance of anaphylaxis. Montelukast blocks LTD₄ binding at its receptor. COX inhibitors block PGE₂. Antihistamines block histamine. Anti-TNF biologics block TNF.
Morphological Patterns of Acute Inflammation
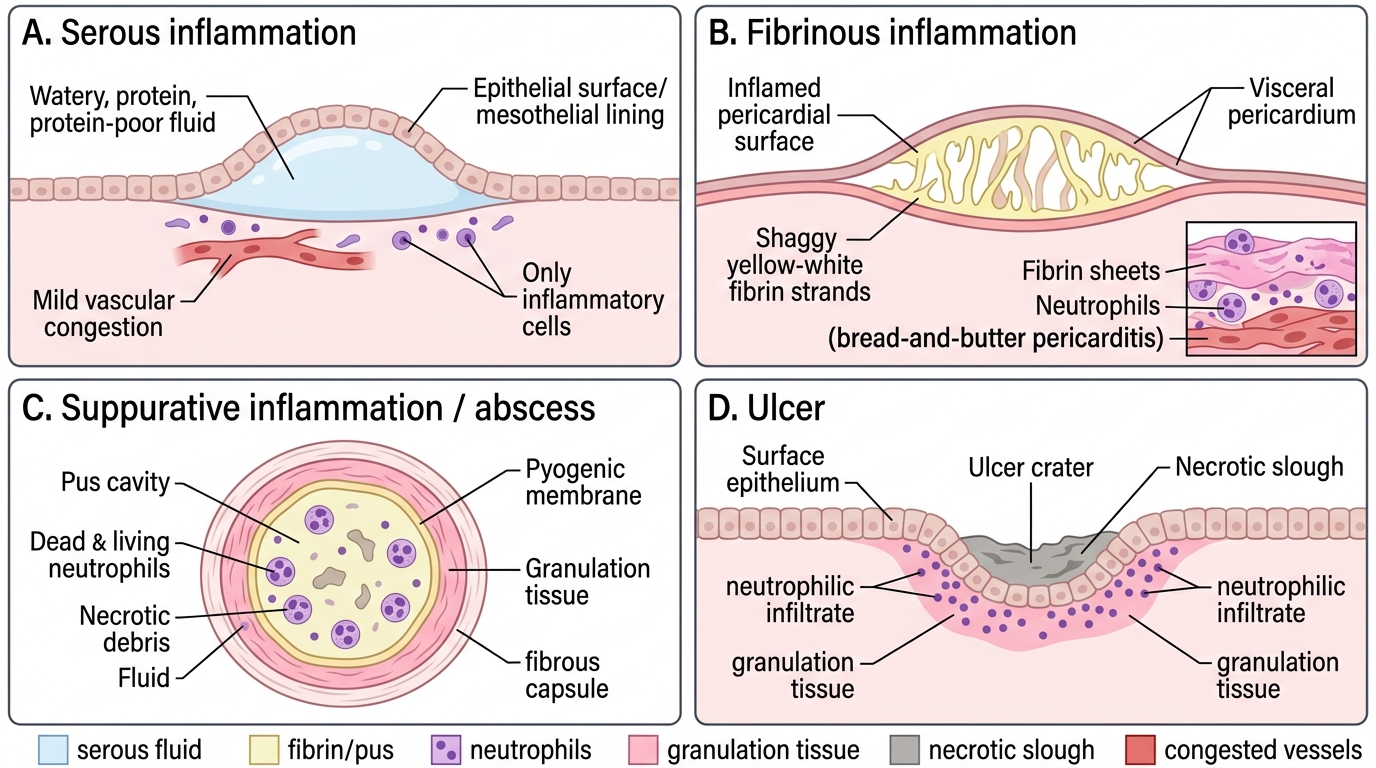
The histological appearance varies with the tissue and injurious agent:
1. Serous inflammation:
• Exudate: watery, protein-poor (3 g/dL).
• Histology: sheets of fibrin; few cells in fluid but underlying tissue shows vascular congestion + neutrophils.
• Examples: fibrinous pericarditis ('bread-and-butter' pattern), fibrinous pleuritis, rheumatic carditis (MacCallum's plaques in mitral valve).
• Outcome: if thin — resolves; if thick — organisation → fibrous adhesions (pericardial, pleural).
3. Suppurative (purulent) inflammation / abscess:
• Exudate: pus = dead/living neutrophils + necrotic tissue + fluid.
• Abscess = localised collection of pus in a cavity formed by liquefactive necrosis.
• Structure: Central pus + pyogenic membrane (inner granulation tissue layer) + outer fibrous capsule.
• Examples: staphylococcal skin abscess, lung abscess, brain abscess.
• Outcome: drain and heal or encapsulate (if not drained).
4. Ulcer:
• Local defect/excavation of surface epithelium following necrosis + sloughing.
• Acute stage: neutrophilic infiltrate at base and edges.
• Examples: peptic ulcer (stomach/duodenum), aphthous ulcer, amoebic intestinal ulcer.
Morphological Patterns of Acute Inflammation
SELF-CHECK
A 45-year-old man develops fever and pleuritic chest pain. Chest X-ray shows pleural effusion. Thoracocentesis yields cloudy fluid with protein 5.2 g/dL, LDH 400 U/L, and abundant neutrophils. What type of inflammation does this represent?
A. Transudate due to cardiac failure
B. Serous inflammation
C. Suppurative (purulent) inflammation
D. Fibrinous inflammation
Reveal Answer
Answer: C. Suppurative (purulent) inflammation
Cloudy fluid with high protein (>3 g/dL), elevated LDH, and abundant neutrophils defines an exudate — specifically suppurative (purulent) inflammation. This is empyema thoracis. Transudates have low protein (<2 g/dL) and form due to haemodynamic imbalance. Serous exudates are clear and watery. Fibrinous inflammation produces a fibrin-rich exudate — typically seen over pericardium/pleura as a rub, before effusion develops.
Outcomes of Acute Inflammation
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Outcomes of Acute Inflammation
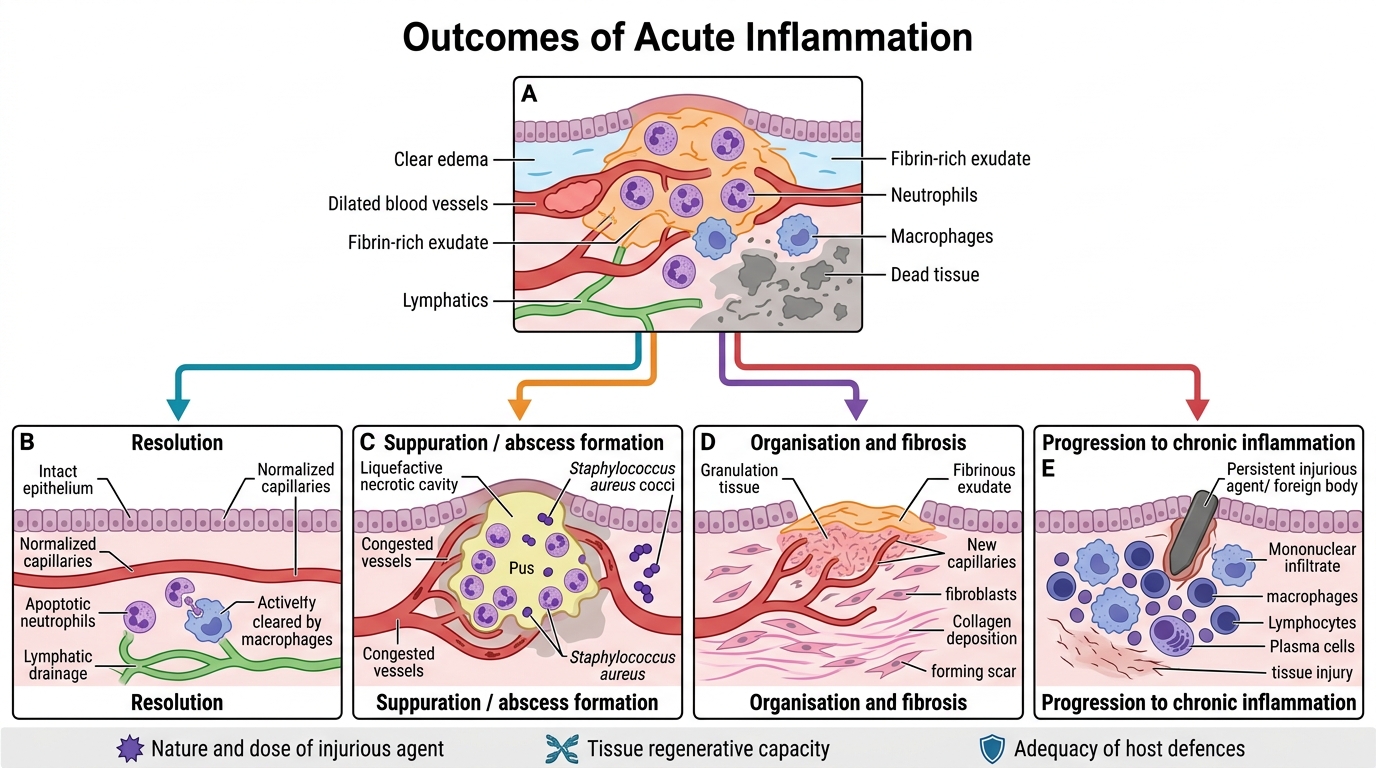
Depending on the balance between injury, mediator intensity, and host defence:
1. Resolution (ideal outcome):
• Complete restoration of normal tissue architecture.
• Conditions: brief injury, small amount of dead tissue, capable regenerating tissue (e.g., early pneumococcal pneumonia, common cold).
• Process: mediator inactivation → vascular normalisation → leucocyte apoptosis → macrophage clearance → exudate drainage via lymphatics.
2. Suppuration (abscess formation):
• When organism produces extensive necrosis (e.g., Staphylococcus aureus).
• Abscess may spontaneously discharge or require surgical drainage.
3. Organisation and fibrosis:
• Large areas of necrosis, fibrinous exudates, or dense suppuration that cannot be reabsorbed.
• Granulation tissue grows in → replaced by collagen → scar (e.g., organised haemothorax → fibrous pleural peel).
4. Progression to chronic inflammation:
• Persistent agent (intracellular pathogens, foreign body, autoimmune stimulus) → shift from neutrophilic to mononuclear infiltrate.
• May occur de novo or after acute phase.
> The outcome depends critically on three factors: (i) nature and dose of injurious agent, (ii) tissue regenerative capacity, and (iii) adequacy of host defences.