Page 3 of 25
PA3.1-2 | Acute Inflammation — Vascular & Cellular Events, Mediators — SDL Guide (Part 3)
Vasoactive Amines: Histamine and Serotonin
Histamine and Serotonin in Early Acute Inflammation
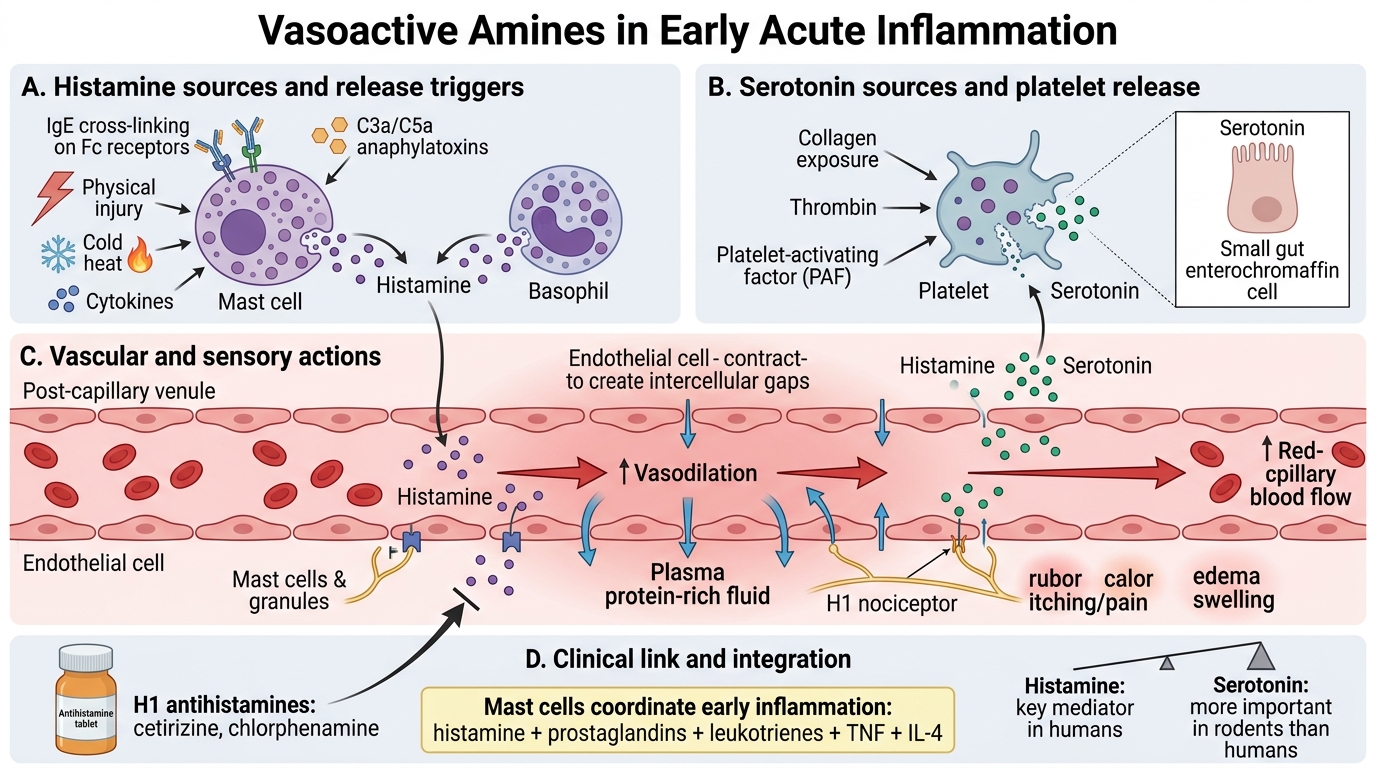
Histamine is the first mediator released in acute inflammation.
Source: Pre-formed, stored in mast cell and basophil granules. Also in platelets.
Release triggers: IgE cross-linking (allergy), C3a/C5a, physical injury, cold, heat, cytokines.
Actions: Vasodilation (↑blood flow → rubor, calor); ↑Vascular permeability by endothelial contraction (venules); Itching/pain via H₁ receptors on nociceptors.
Clinical link: Antihistamines (cetirizine, chlorphenamine) block H₁ receptors — used for urticaria, anaphylaxis, rhinitis.
Serotonin (5-hydroxytryptamine):
Source: Pre-formed in platelet dense granules. Also enterochromaffin cells (gut).
Actions: Similar to histamine — vasoactive; more important in rodents than humans.
Release: Platelet activation by collagen, thrombin, PAF.
> Mast cells are the master coordinators of early acute inflammation: they store histamine AND produce prostaglandins, leukotrienes, TNF, and IL-4 — connecting immediate and acquired immunity.
Arachidonic Acid Metabolites: Prostaglandins and Leukotrienes
Arachidonic Acid Metabolites in Inflammation
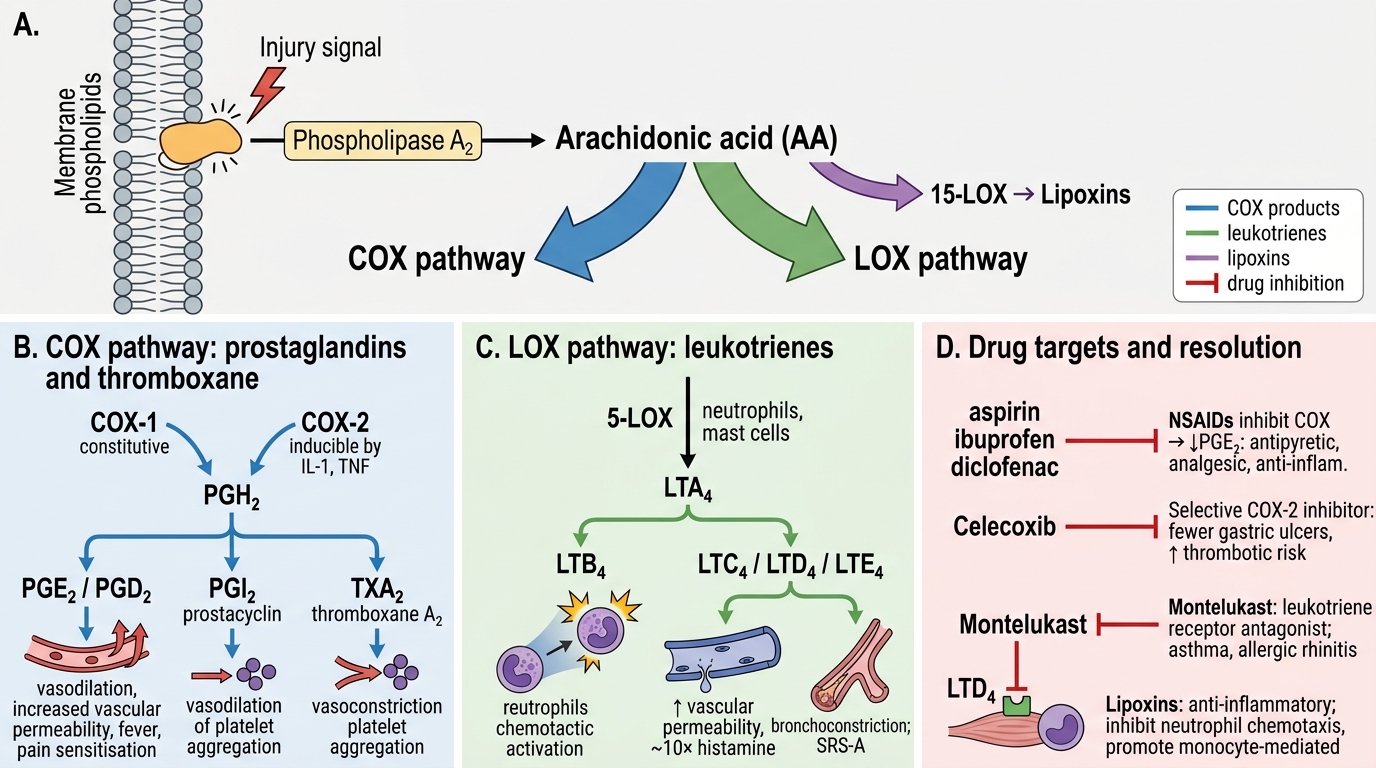
Arachidonic acid (AA) is released from membrane phospholipids by phospholipase A₂ (activated by injury signals). It is then metabolised by two divergent enzyme pathways:
COX (cyclooxygenase) pathway → prostaglandins and thromboxane:
• COX-1 (constitutive) + COX-2 (inducible, induced by IL-1, TNF) → PGH₂ → tissue-specific isomerases:
- PGE₂, PGD₂: vasodilation, ↑permeability, fever (hypothalamic action), pain sensitisation (hyperalgesia).
- PGI₂ (prostacyclin): vasodilation, inhibits platelet aggregation.
- Thromboxane A₂: vasoconstriction, platelet aggregation (from platelets).
• Pharmacology: NSAIDs (aspirin, ibuprofen, diclofenac) inhibit COX → ↓PGE₂ → antipyretic + analgesic + anti-inflammatory. Selective COX-2 inhibitors (celecoxib) spare gastric PGE₂ (↓ulcers) but ↑thrombotic risk (↓PGI₂ without ↓TXA₂).
LOX (lipoxygenase) pathway → leukotrienes:
• 5-LOX (neutrophils, mast cells) → LTA₄ → LTB₄ or cysteinyl leukotrienes (LTC₄, LTD₄, LTE₄).
• LTB₄: powerful chemotactic agent for neutrophils; also activates neutrophils.
• LTC₄/LTD₄/LTE₄: ↑Vascular permeability (10× more potent than histamine); bronchoconstriction — the principal mediators of slow-reacting substance of anaphylaxis (SRS-A).
• Pharmacology: Montelukast (leukotriene receptor antagonist) blocks LTD₄ receptor → used in asthma, allergic rhinitis.
Lipoxins (from AA, via 15-LOX): anti-inflammatory — inhibit neutrophil chemotaxis, promote monocyte recruitment → resolution signal.
Platelet-Activating Factor, Cytokines, Nitric Oxide
Key Chemical Mediators: PAF, Cytokines, Chemokines and NO
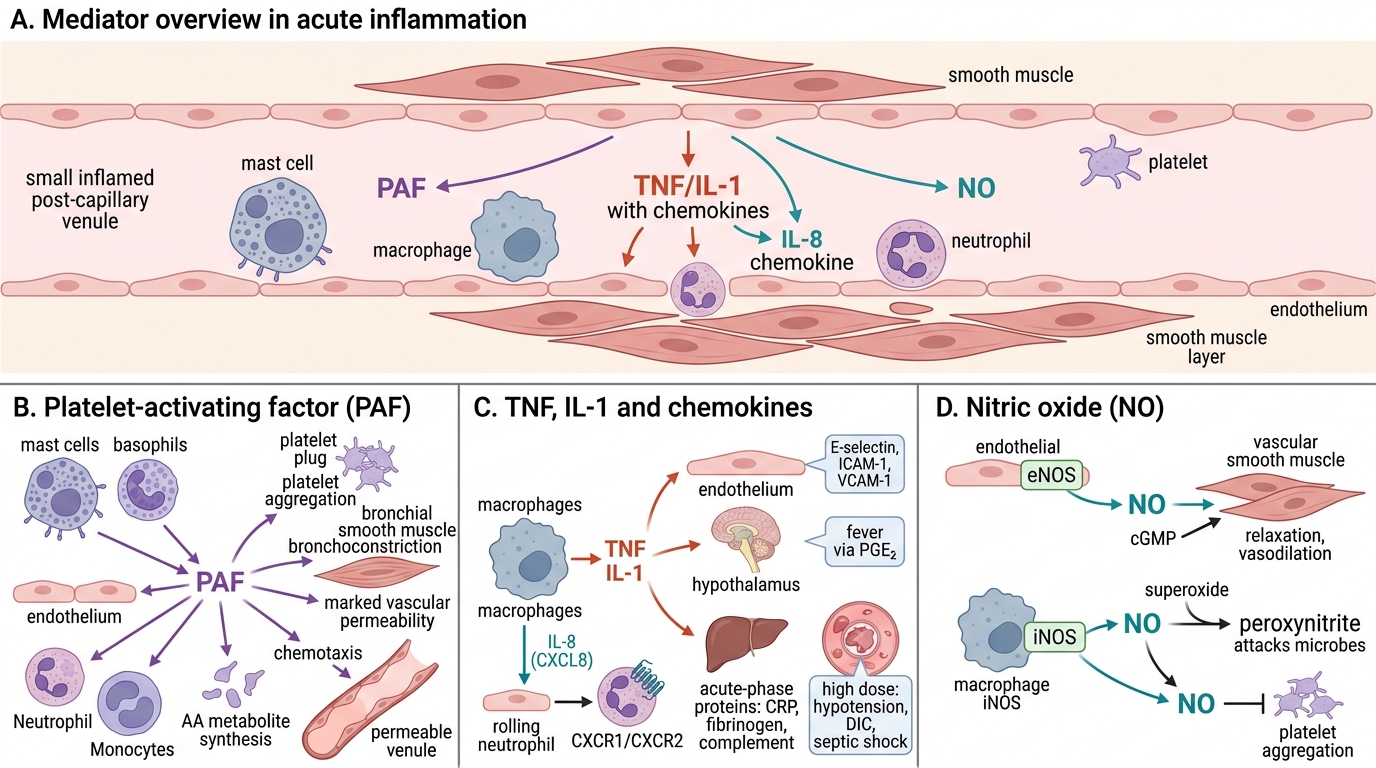
Platelet-activating factor (PAF):
Source: Mast cells, basophils, endothelium, neutrophils, monocytes.
Actions: Platelet aggregation; bronchoconstriction; 100–1,000× more potent than histamine in increasing vascular permeability; chemotaxis; synthesis of other mediators (AA metabolites).
Cytokines — TNF and IL-1:
Source: Primarily macrophages (also mast cells, endothelium, T cells).
Actions: Both are pleiotropic — multiple targets:
• Endothelium: ↑adhesion molecule expression (E-selectin, ICAM-1, VCAM-1), ↑procoagulant activity.
• Hypothalamus: fever (via PGE₂ induction by COX-2).
• Liver: acute-phase protein synthesis (CRP, fibrinogen, complement) — the acute-phase response.
• Systemic (high dose): hypotension, DIC — septic shock.
• TNF also promotes cachexia (muscle wasting in chronic inflammation/cancer).
Chemokines:
• Family of ~40 proteins; primary function: leucocyte chemotaxis and activation.
• IL-8 (CXCL8): secreted by macrophages, endothelium → strong neutrophil chemoattractant; presented on endothelial surface to activate rolling neutrophils.
• CXCR1/CXCR2 are the receptors on neutrophils.
Nitric oxide (NO):
Source: Endothelial cells (eNOS, constitutive); macrophages (iNOS, inducible by LPS/cytokines).
Actions:
• Vasodilation: relaxes vascular smooth muscle (↑cGMP).
• Antimicrobial: reacts with O₂•⁻ → peroxynitrite (ONOO⁻), toxic to microbes.
• Anti-platelet: inhibits aggregation.
• Regulates leucocyte recruitment (inhibits excessive rolling/adhesion at low concentrations).