Page 9 of 25
PA3.3 | Chronic & Granulomatous Inflammation — SDL Guide (Part 4)
Systemic Effects of Inflammation
Systemic Effects of Inflammation
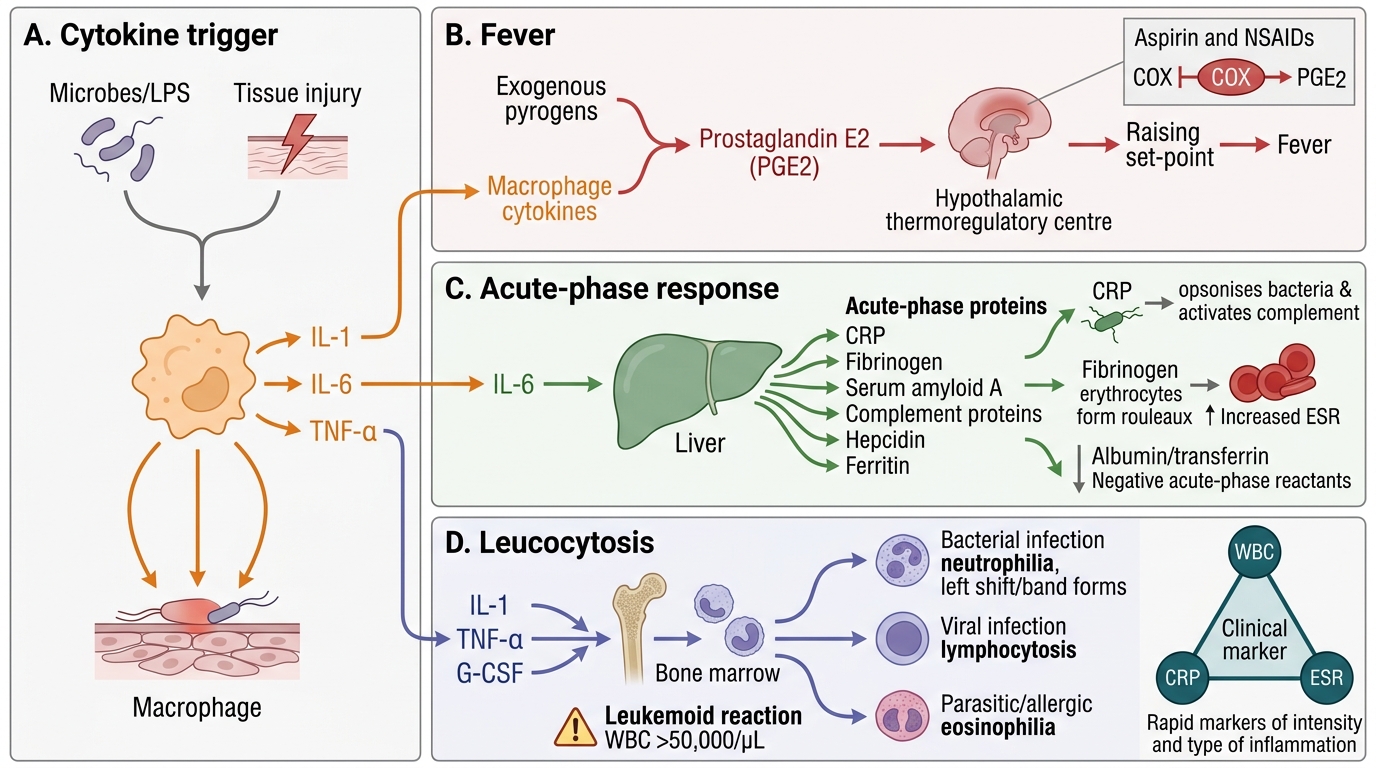
Both acute and chronic inflammation trigger a systemic response via cytokines (mainly IL-1, IL-6, TNF-α) released by activated macrophages.
1. Fever:
• Exogenous pyrogens (LPS, microbial products) → stimulate macrophages → endogenous pyrogens (IL-1, IL-6, TNF-α, prostaglandin E2)
• Prostaglandin E2 acts on the hypothalamic thermoregulatory centre → raises the thermostat set-point → fever
• Aspirin/NSAIDs reduce fever by inhibiting cyclooxygenase (COX) → reduced PGE2 synthesis
2. Acute-phase response:
• IL-6 stimulates the liver to produce acute-phase proteins: C-reactive protein (CRP), fibrinogen, serum amyloid A, complement proteins, hepcidin, ferritin
• CRP: Opsonises bacteria and activates complement; clinical marker of inflammation/infection
• Fibrinogen: Coats erythrocytes → increased rouleaux formation → elevated erythrocyte sedimentation rate (ESR)
• Albumin and transferrin are negative acute-phase reactants (decrease during inflammation)
3. Leucocytosis:
• IL-1, TNF-α, G-CSF → mobilise neutrophils from bone marrow
• Bacterial infections → neutrophilia (with left shift — band forms)
• Viral infections → lymphocytosis
• Parasitic/allergic conditions → eosinophilia
• Severe infections → leukemoid reaction (WBC >50,000/µL)
Clinical marker triangle: WBC count + CRP + ESR together give you a rapid, inexpensive window into the intensity and type of inflammation.
SELF-CHECK
A 60-year-old man with longstanding rheumatoid arthritis has a serum CRP of 85 mg/L, ESR of 110 mm/hr, and haemoglobin of 9.2 g/dL. Which acute-phase protein is MOST responsible for the elevated ESR?
A. C-reactive protein (CRP)
B. Serum amyloid A (SAA)
C. Fibrinogen
D. Albumin
Reveal Answer
Answer: C. Fibrinogen
Fibrinogen (elevated during inflammation under IL-6 stimulation) coats red blood cells, promoting rouleaux formation and increasing the rate at which they sediment — directly elevating ESR. CRP is an opsonin and clinical inflammation marker but does not directly affect ESR. Albumin is a negative acute-phase reactant.
Comparing Acute vs Chronic — A Clinico-Pathological Summary
Acute vs Chronic Inflammation: Clinical and Pathological Summary
Synthesising both G1 and G2, the following framework anchors chronic inflammation in clinical practice:
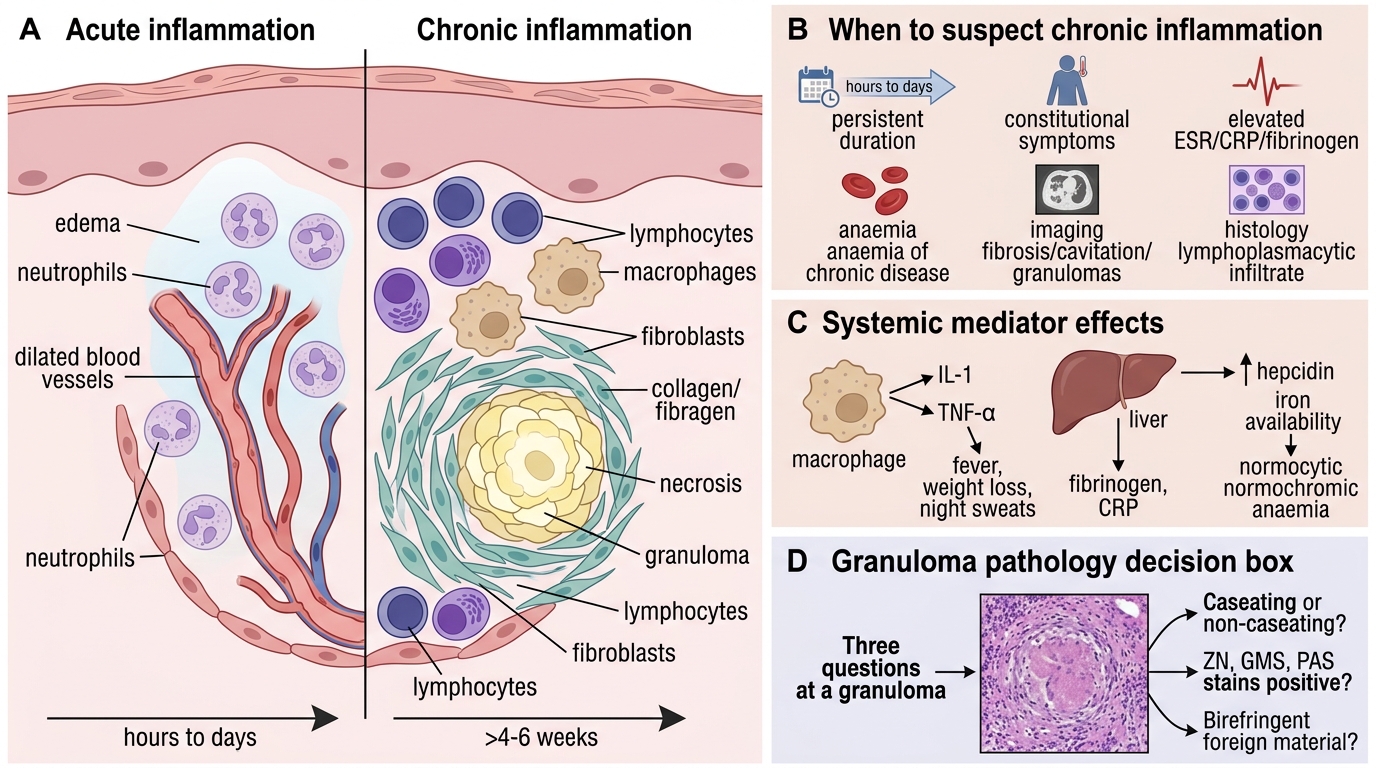
When to suspect chronic (rather than acute) inflammation:
• Duration >4–6 weeks without resolution
• Constitutional symptoms dominate (low-grade fever, weight loss, night sweats) — driven by sustained IL-1/TNF-α
• Laboratory: elevated ESR, CRP, fibrinogen; normocytic normochromic anaemia (anaemia of chronic disease via hepcidin↑ + erythropoietin responsiveness↓)
• Imaging: fibrosis, cavitation, granulomas (CT/PET)
• Histology: lymphoplasmacytic infiltrate ± granulomas ± fibrosis
The three questions a pathologist asks at a granuloma:
1. Is it caseating or non-caseating?
2. Are special stains (ZN, GMS, PAS) positive?
3. Is there birefringent foreign material?
Answering these three questions narrows a granuloma differential from 30 diagnoses to 2–3.