Page 8 of 25
PA3.3 | Chronic & Granulomatous Inflammation — SDL Guide (Part 3)
Granuloma Formation Mechanism
Granuloma Formation and Maintenance
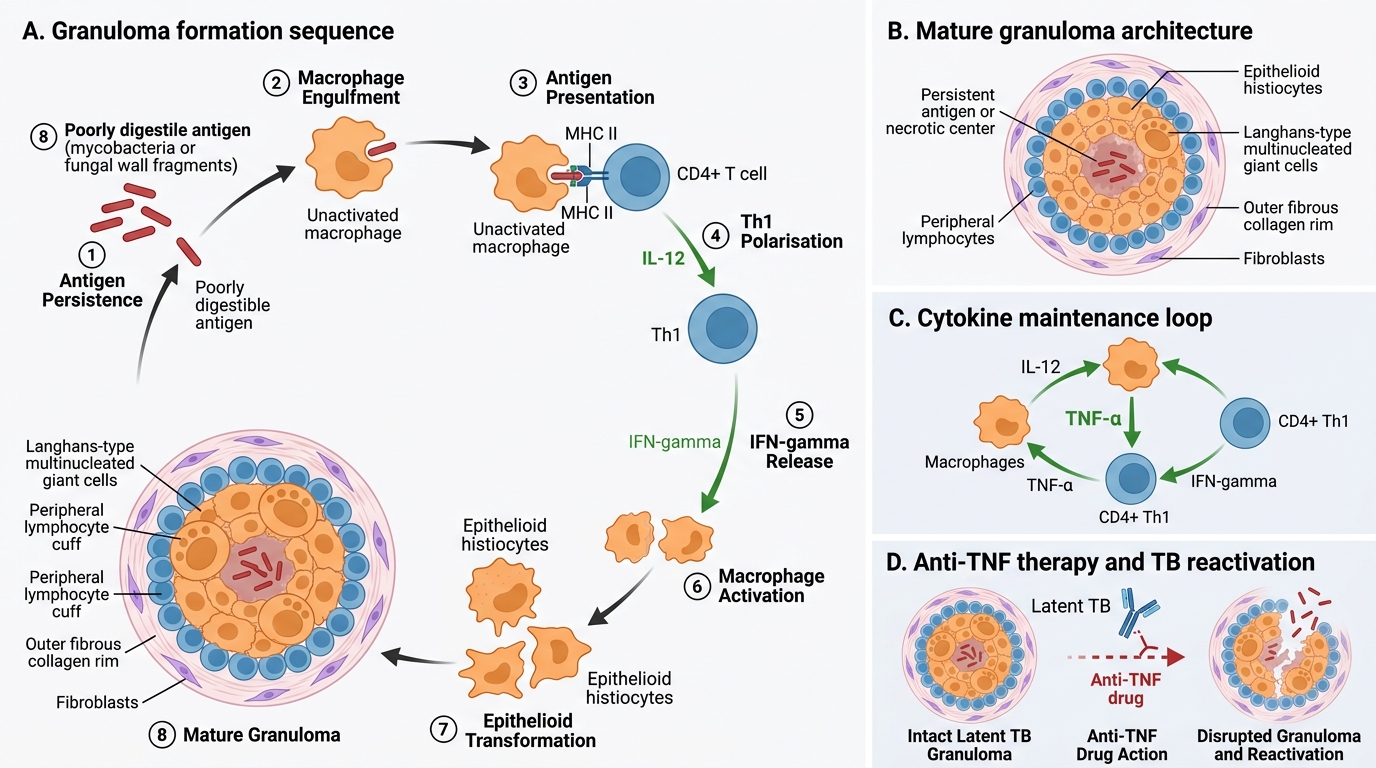
Granulomas form when the immune system cannot eliminate an antigen — instead, it attempts to contain or wall it off.
Step-by-step sequence:
- Macrophages engulf the poorly digestible agent (mycobacterium, fungal cell wall, foreign particle).
- Macrophages present antigen to CD4+ T cells via MHC II.
- Th1 polarisation: IL-12 (from macrophages) + antigen → Th1 CD4+ cells → secrete IFN-γ.
- IFN-γ activates macrophages → epithelioid transformation.
- Activated macrophages secrete TNF-α — critical for granuloma maintenance (TNF-α blockade with anti-TNF biologics reactivates latent TB by disrupting this step).
- Epithelioid histiocytes fuse → multinucleate giant cells.
- Lymphocytes accumulate at periphery, sustaining IFN-γ production.
- Over weeks–months, fibroblasts deposit collagen → fibrous rim (walling-off).
Clinical implication: Patients on anti-TNF therapy (infliximab, adalimumab for rheumatoid arthritis/Crohn) must be screened for latent TB before treatment — TNF-α blockade can dissolve pre-existing granulomas and reactivate dormant bacilli.
Caseating vs Non-Caseating Granulomas
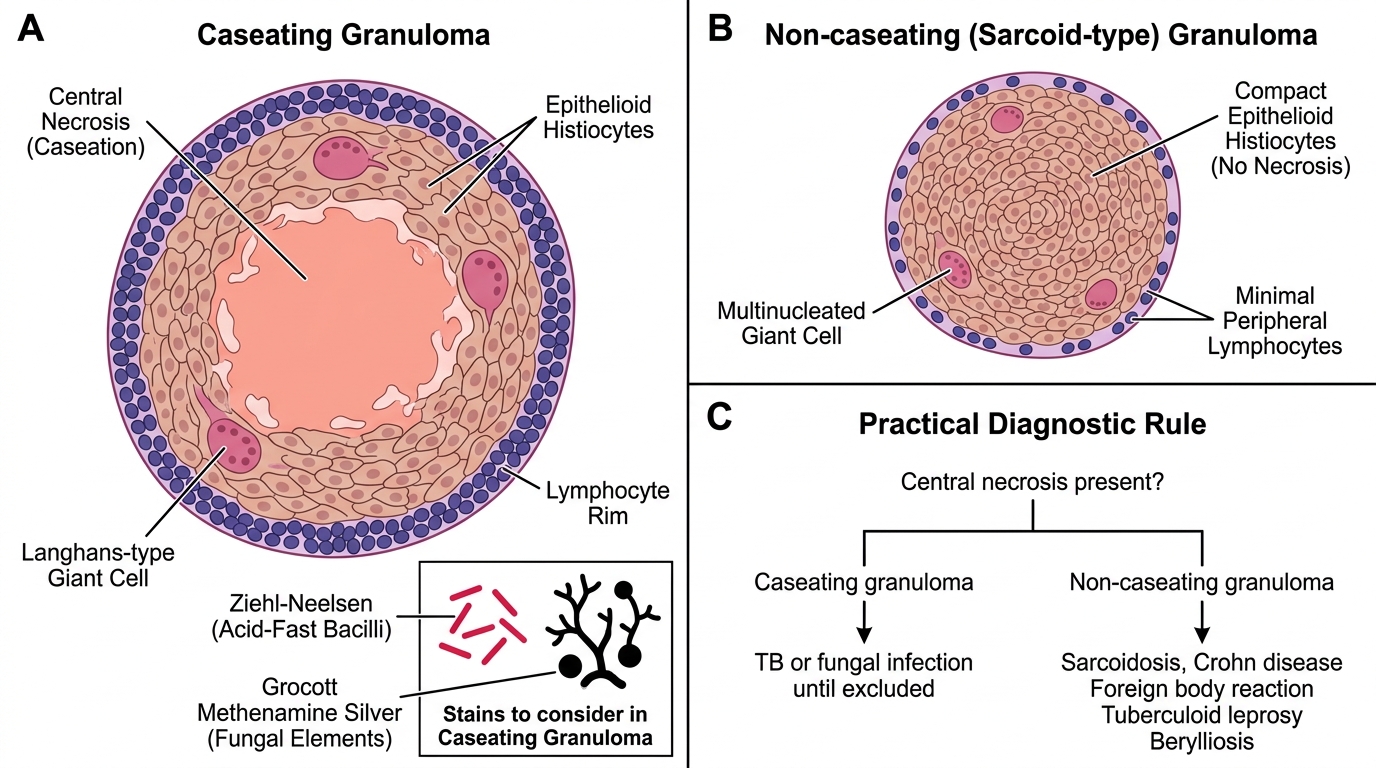
The presence or absence of central necrosis is the single most important distinguishing feature at histology.
Caseating (necrotising) granulomas:
• Central zone of coagulative necrosis with a cheese-like (caseous) gross appearance — pale, crumbling, dry
• Microscopically: amorphous eosinophilic debris, no surviving cell outlines (unlike liquefactive necrosis)
• Caused by: TB (most common), histoplasmosis, coccidioidomycosis, blastomycosis, occasionally cat-scratch disease
• Mechanism: Th1-mediated delayed hypersensitivity (Type IV) + direct cytotoxic killing → necrosis of macrophages and adjacent tissue
Non-caseating (non-necrotising) granulomas:
• No central necrosis — epithelioid histiocytes fill the granuloma to its centre
• Histologically "cleaner" — well-circumscribed aggregate with no debris
• Caused by: sarcoidosis (tight, "naked" granulomas), Crohn disease, foreign-body reactions, leprosy (tuberculoid type), berylliosis
Practical rule: Find acid-fast bacilli (Ziehl-Neelsen stain) or fungal elements (Grocott methenamine silver) in any caseating granuloma before labelling it sarcoidosis — sarcoidosis is a diagnosis of exclusion.
Caseating vs Non-Caseating Granulomas
SELF-CHECK
A 28-year-old woman has bilateral hilar lymphadenopathy and erythema nodosum. Lymph node biopsy shows tight clusters of epithelioid histiocytes WITHOUT central necrosis. AFB and fungal stains are negative. Which pattern best describes this granuloma?
A. Caseating granuloma — consistent with active TB
B. Non-caseating granuloma — consistent with sarcoidosis
C. Foreign-body granuloma — likely suture reaction
D. Suppurative granuloma — consistent with cat-scratch disease
Reveal Answer
Answer: B. Non-caseating granuloma — consistent with sarcoidosis
Tight non-caseating granulomas in bilateral hilar nodes with negative AFB/fungal stains in a young woman are the hallmark of sarcoidosis. TB (caseating) and cat-scratch disease (suppurative centre, Bartonella) have distinct patterns. Foreign-body granulomas require identifiable foreign material.
Classic Causes of Granulomatous Inflammation
Classic Causes of Granulomatous Inflammation
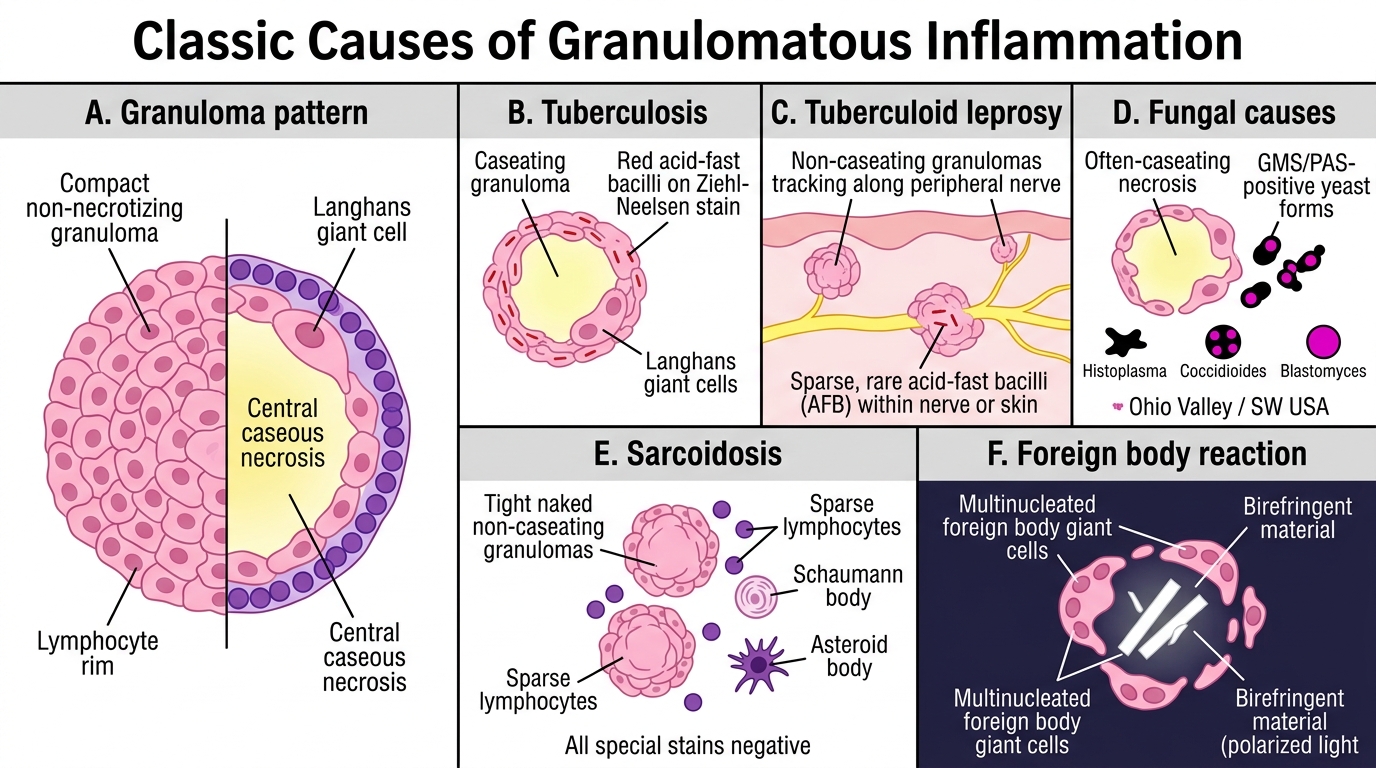
A structured differential for granulomas is a core clinical skill. Learn the distinguishing histological or microbiological clue for each:
| Cause | Caseating? | Distinguishing feature |
|---|---|---|
| Mycobacterium tuberculosis | Yes | AFB on ZN stain; Langhans giant cells |
| M. leprae (tuberculoid leprosy) | No | AFB in nerves/skin; granulomas track nerves |
| Fungal (Histoplasma, Coccidioides, Blastomyces) | Yes (often) | GMS/PAS stain — yeast forms; geography (Ohio valley, SW USA) |
| Sarcoidosis | No | Naked tight granulomas; Schaumann bodies, asteroid bodies; all stains negative |
| Foreign body | No | Birefringent material under polarised light; FBGCs |
| Crohn disease | No | Transmural inflammation; non-caseating micro-granulomas |
| Syphilis (T. pallidum) | No (gumma = coagulative) | Gumma (rubbery, not caseous); plasma cell rich; VDRL/TPHA positive |
| Cat-scratch disease (Bartonella) | No | Suppurative (stellate) centre; Warthin-Starry silver stain |
Memory framework: TB-FLOSS-C — TB, fungal, Leprosy, sarcOidosiS, Syphilis, Crohn, cat-scratch.
In India, prioritise TB and leprosy in your differential before considering sarcoidosis.
CLINICAL PEARL
The anti-TNF trap in clinical practice:
Before starting any biologic that blocks TNF-α (infliximab, adalimumab, etanercept) — used in rheumatoid arthritis, Crohn disease, psoriasis, ankylosing spondylitis — you must screen the patient for latent tuberculosis (tuberculin skin test or IGRA + chest X-ray).
Why? TNF-α is essential for granuloma integrity. Its blockade causes "granuloma dissolution" — previously walled-off dormant mycobacteria are released into the circulation. The resulting reactivation TB can be miliary (disseminated), rapidly fatal, and is notoriously difficult to diagnose in immunosuppressed patients.
In high-burden countries like India, this screening is non-negotiable before every biologic prescription.