Page 11 of 25
PA4.1 | Healing & Repair — Regeneration, Granulation Tissue, Wound Healing — SDL Guide
Learning Objectives
- Distinguish regeneration from repair by connective tissue (fibrosis/scar) and state when each occurs
- Classify cells by proliferative capacity (labile, stable, permanent) and predict healing potential
- Describe the sequential steps of repair: haemostasis → granulation tissue formation → proliferation → maturation/remodelling
- Identify the key growth factors (VEGF, PDGF, FGF, TGF-β) and ECM components that orchestrate each step
- Compare primary intention with secondary intention wound healing, including the role of myofibroblasts
- List local and systemic factors that impair healing and explain their mechanisms
- Recognise complications of healing: dehiscence, chronic ulceration, hypertrophic scar, keloid, and contracture
- Briefly describe healing in bone (fracture callus), liver, and CNS (gliosis)
INSTRUCTIONS
Every wound you will manage as a clinician heals through the same molecular ballet. Understanding the cellular actors, the growth-factor choreography, and the critical checkpoints of repair will let you predict which wounds will heal cleanly, which will fail, and which will overshoot into pathological scarring. This module builds directly on your inflammation knowledge from SDL-2 and prepares you for the surgical and wound-care decisions you will face from Year 3 onward.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 3 (Tissue Renewal, Regeneration, and Repair) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 6 (Healing and Repair) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 28-year-old construction worker lacerates his palm on a rusty metal edge. The wound is cleaned and sutured the same evening. Eight days later the sutures are removed — the scar is a thin white line, barely visible.
A month later, his co-worker suffers a degloving injury of the same hand. Left to heal without skin grafting, the wound fills with pink fleshy tissue, contracts, and leaves a broad, firm scar that limits finger extension.
Same organ, same tissue — yet dramatically different outcomes. Why?
RECALL
Before continuing, spend 60 seconds recalling:
- What are the four cardinal signs of acute inflammation?
- What is the difference between exudate and transudate?
- Name two pro-inflammatory cytokines released by macrophages.
These answers matter: healing begins where inflammation leaves off, and macrophages are the conductors of the entire repair orchestra.
Regeneration vs Repair — Two Paths After Injury
Regeneration vs Repair After Injury
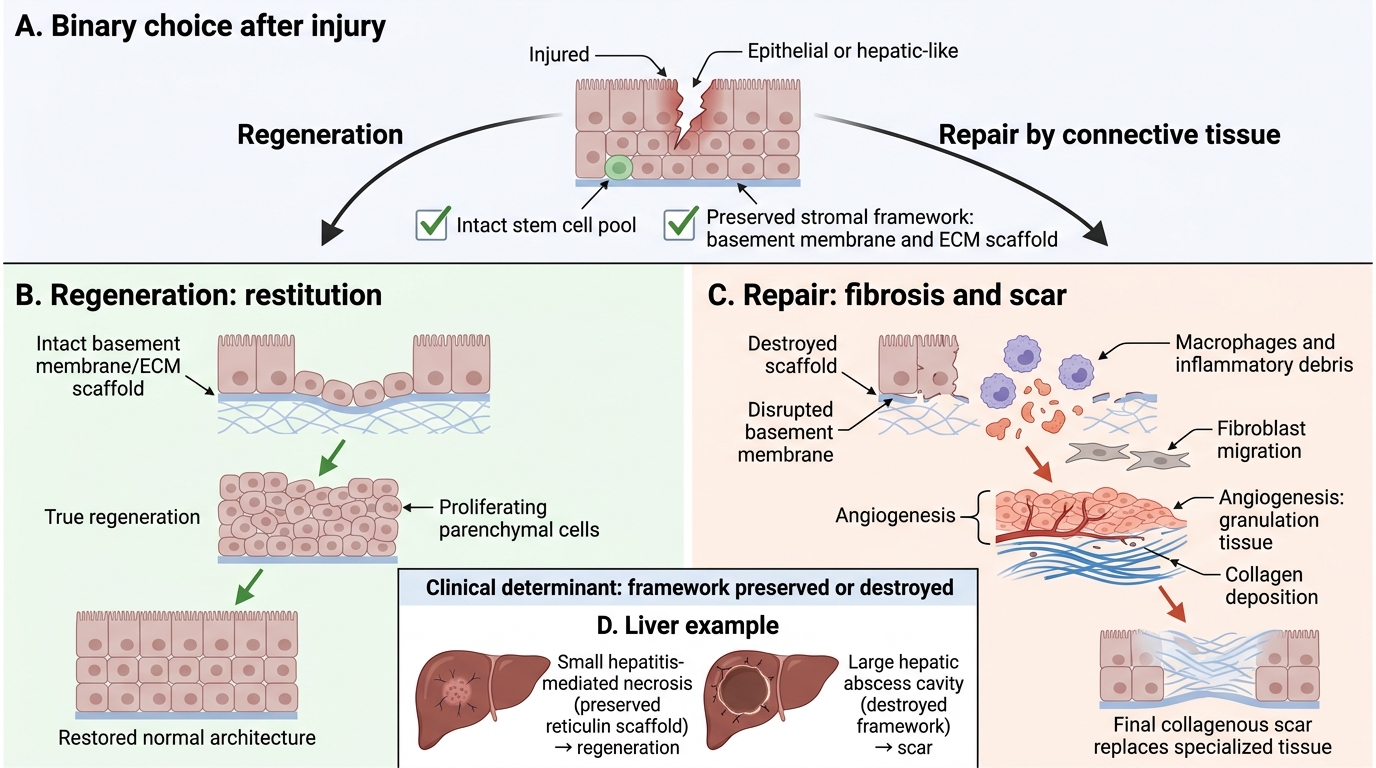
When tissue is injured, the body faces a binary choice: regeneration (replacing lost cells with identical new cells, restoring normal architecture) or repair by connective tissue (filling the defect with scar, permanently altering architecture).
Regeneration is restitution — parenchymal cells proliferate and reconstitute the lost tissue. It requires two conditions to succeed:
1. The stem cell pool must be intact (capable of producing replacement parenchymal cells).
2. The stromal framework — the extracellular scaffold (basement membrane, ECM) — must be preserved as a template.
If the framework is destroyed (e.g., a large hepatic abscess versus a small hepatitis-mediated necrosis), even a tissue with high regenerative capacity cannot achieve true regeneration; connective tissue scar fills in instead.
Repair by connective tissue (fibrosis/scarring) occurs when regeneration is impossible or insufficient: the damaged tissue is replaced by granulation tissue that matures into a collagenous scar. This restores structural integrity but sacrifices specialised function.
Cell Proliferative Capacity — Who Can Regenerate?
Cell Proliferative Capacity and Healing Outcome
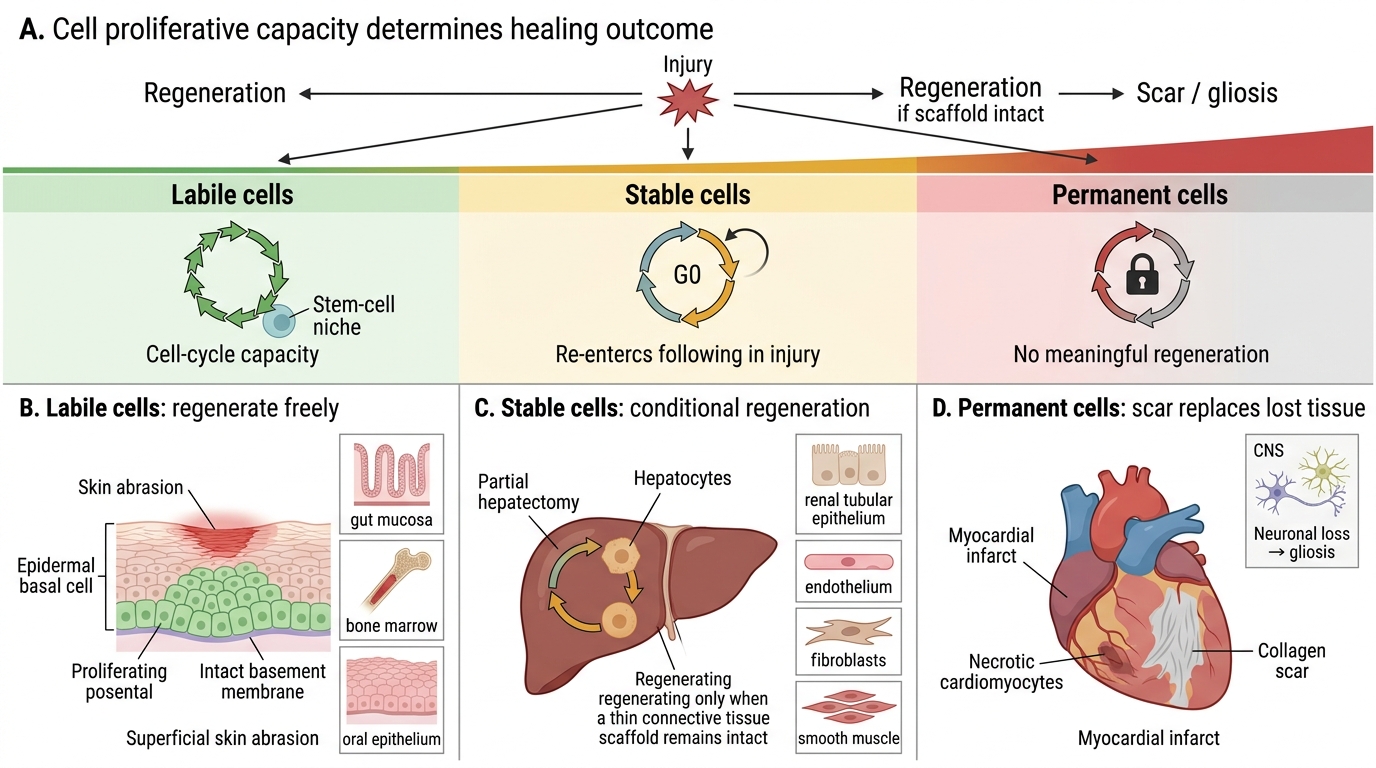
The fate of an injured tissue depends heavily on which class its cells belong to:
| Class | Characteristic | Examples | Healing potential |
|---|---|---|---|
| Labile cells | Continuously cycling; robust stem-cell compartment | Skin epidermis, gut mucosa, bone marrow, oral epithelium | High — regenerate freely |
| Stable cells | Normally quiescent (G0); re-enter cell cycle when stimulated | Hepatocytes, renal tubular cells, smooth muscle, fibroblasts, endothelium | Moderate — regenerate if scaffold intact |
| Permanent cells | Terminally differentiated; cannot divide post-natally | Neurons (CNS), cardiac myocytes, skeletal muscle fibres | None — defect filled by scar/gliosis |
Key clinical corollary: a superficial skin abrasion heals by regeneration (labile epithelial cells). A myocardial infarct heals exclusively by scar (permanent cardiomyocytes). A partial hepatectomy regenerates if the connective tissue scaffold survives.
Repair by Connective Tissue — Sequential Steps
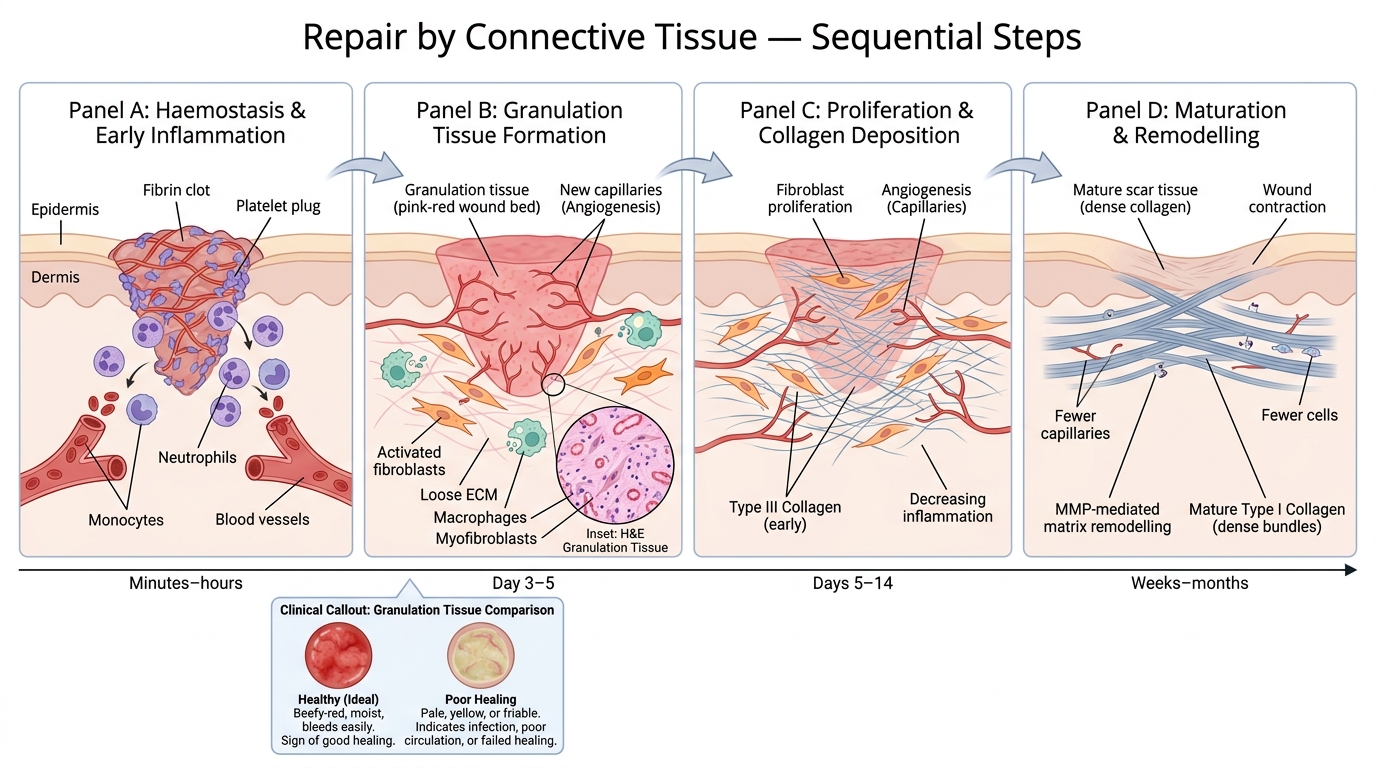
Repair proceeds in four overlapping but conceptually distinct phases:
Step 1 — Haemostasis & Early Inflammation (Minutes to hours)
Platelet plug and fibrin clot form immediately. Clot acts as provisional scaffold and releases PDGF and TGF-β, signalling the start of repair. Neutrophils arrive first (acute inflammation), followed by monocytes differentiating into tissue macrophages.
Step 2 — Granulation Tissue Formation (Day 3–5)
Macrophages orchestrate: they clear debris, release growth factors, and recruit fibroblasts and endothelial cells. The result is granulation tissue — the hallmark of repair — characterised by:
• New thin-walled capillaries (angiogenesis) giving a pink-red granular appearance
• Activated fibroblasts synthesising ECM
• Loose ECM (fibronectin, hyaluronan, type III collagen)
• Macrophages and occasional myofibroblasts
IMPORTANT: Clinically, healthy granulation tissue is beefy-red, moist, and bleeds easily. Pale, yellow, or friable granulation tissue signals poor healing.
Sequential Steps in Repair by Connective Tissue
Step 3 — Proliferation (Days 5–14)
Fibroblasts proliferate and secrete increasing amounts of collagen (initially type III). Angiogenesis continues. The wound gains tensile strength.
Step 4 — Maturation & Remodelling (Weeks to months)
Matrix metalloproteinases (MMPs) degrade type III collagen, which is progressively replaced by thicker type I collagen fibres, cross-linked by lysyl oxidase. The vascular density decreases (vessels regress). The scar loses its red colour and becomes pale. A fully matured scar retains only ~70-80% of the original tensile strength.