Page 12 of 25
PA4.1 | Healing & Repair — Regeneration, Granulation Tissue, Wound Healing — SDL Guide (Part 2)
Growth Factors and ECM — The Molecular Orchestra
Growth Factors and ECM in Wound Healing
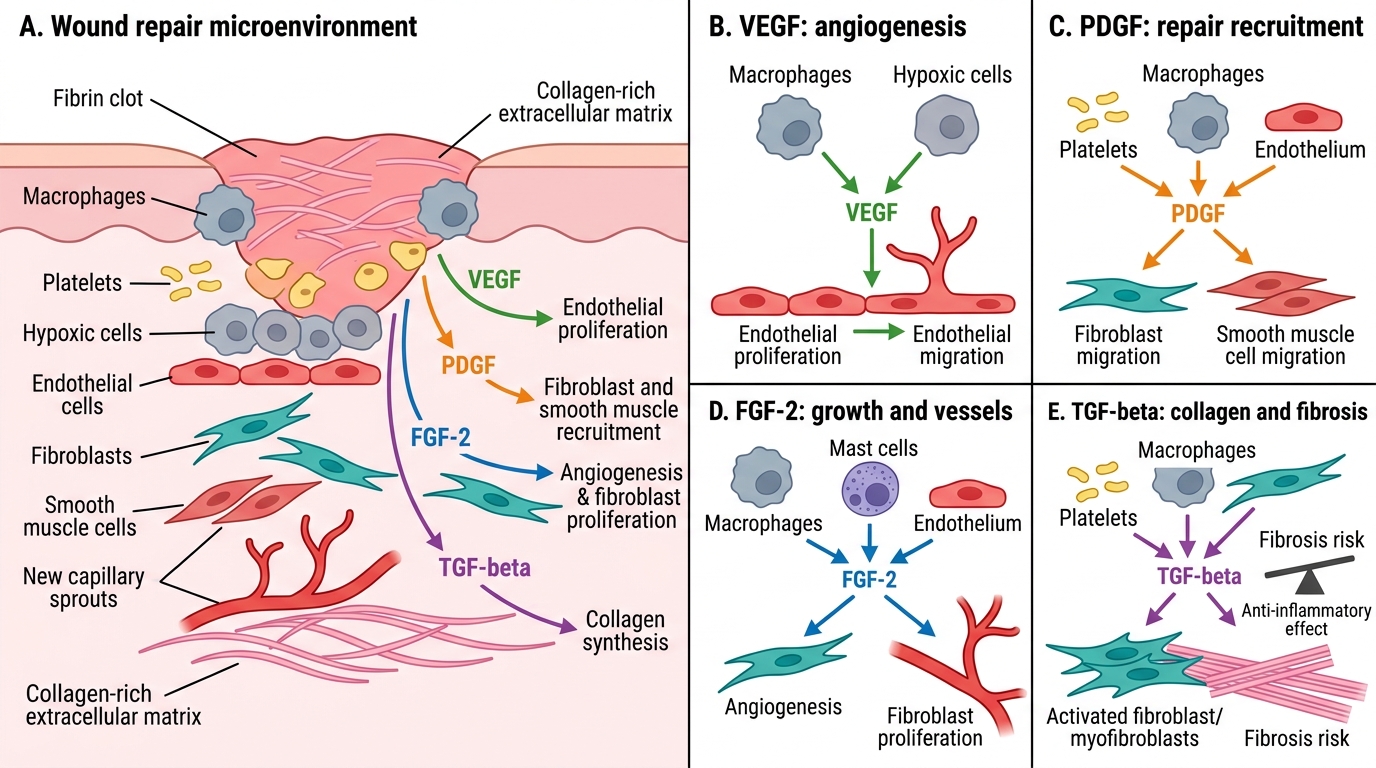
Four growth factors deserve explicit memory at Year-2 level:
| Growth factor | Source | Primary role in healing |
|---|---|---|
| VEGF (Vascular Endothelial Growth Factor) | Macrophages, hypoxic cells | Angiogenesis — endothelial proliferation and migration |
| PDGF (Platelet-Derived Growth Factor) | Platelets, macrophages, endothelium | Fibroblast + smooth-muscle recruitment; initiates repair signalling |
| FGF (Fibroblast Growth Factor, esp. FGF-2) | Macrophages, mast cells, endothelium | Angiogenesis + fibroblast proliferation |
| TGF-β (Transforming Growth Factor-beta) | Platelets, macrophages, fibroblasts | Fibroblast activation, collagen synthesis, anti-inflammatory; chief driver of fibrosis |
ECM roles: fibronectin provides provisional scaffold and promotes cell migration; hyaluronan retains water, resists compression early on; proteoglycans (e.g., decorin) regulate collagen fibrillogenesis; type III collagen provides early tensile strength, replaced by type I in remodelling.
Overarching concept: TGF-β is the master fibrogenic cytokine. Its unchecked activity drives pathological fibrosis in liver (cirrhosis), lung, and kidney.
SELF-CHECK
Which growth factor is the primary driver of angiogenesis during granulation tissue formation?
A. TGF-β
B. VEGF
C. PDGF
D. FGF-2
Reveal Answer
Answer: B. VEGF
VEGF (Vascular Endothelial Growth Factor) is the dominant angiogenic signal, produced by macrophages and hypoxic cells. It drives endothelial proliferation and capillary sprouting. PDGF recruits fibroblasts; TGF-β drives collagen synthesis; FGF-2 supports angiogenesis but is secondary to VEGF.
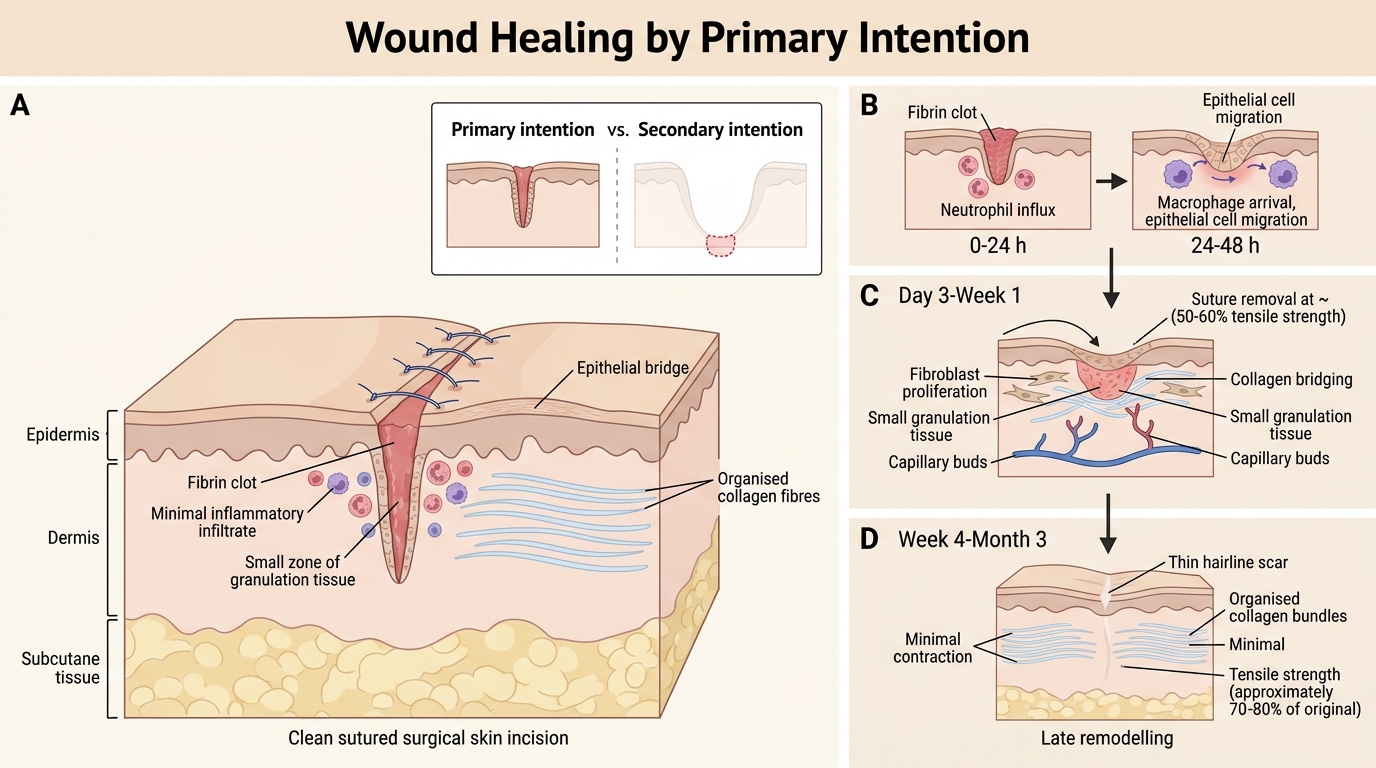
Wound Healing by Primary Intention
Primary intention (healing by first intention) applies to clean, surgically apposed wounds (e.g., a sutured surgical incision):
- Wound edges are close together — minimal tissue defect
- Inflammatory response is brief and localised
- Granulation tissue volume is small
- Epithelial coverage occurs within 24-48 hours (epithelial bridge across incision)
- Collagen deposition is organised and aligned
- Minimal wound contraction
- End result: thin, hairline scar with rapid functional restoration
Timeline (skin incision, primary closure):
| Time | Event |
|---|---|
| 0-24 h | Fibrin clot; neutrophil influx |
| 24-48 h | Macrophage arrival; epithelial cells migrate across incision |
| Day 3-5 | Granulation tissue; fibroblast proliferation begins |
| Week 1 | Collagen bridges; sutures removed (~50-60% tensile strength) |
| Week 4+ | Remodelling; scar pales |
| Month 3 | ~70-80% original tensile strength (maximum achievable) |
Wound Healing by Primary Intention
Wound Healing by Secondary Intention
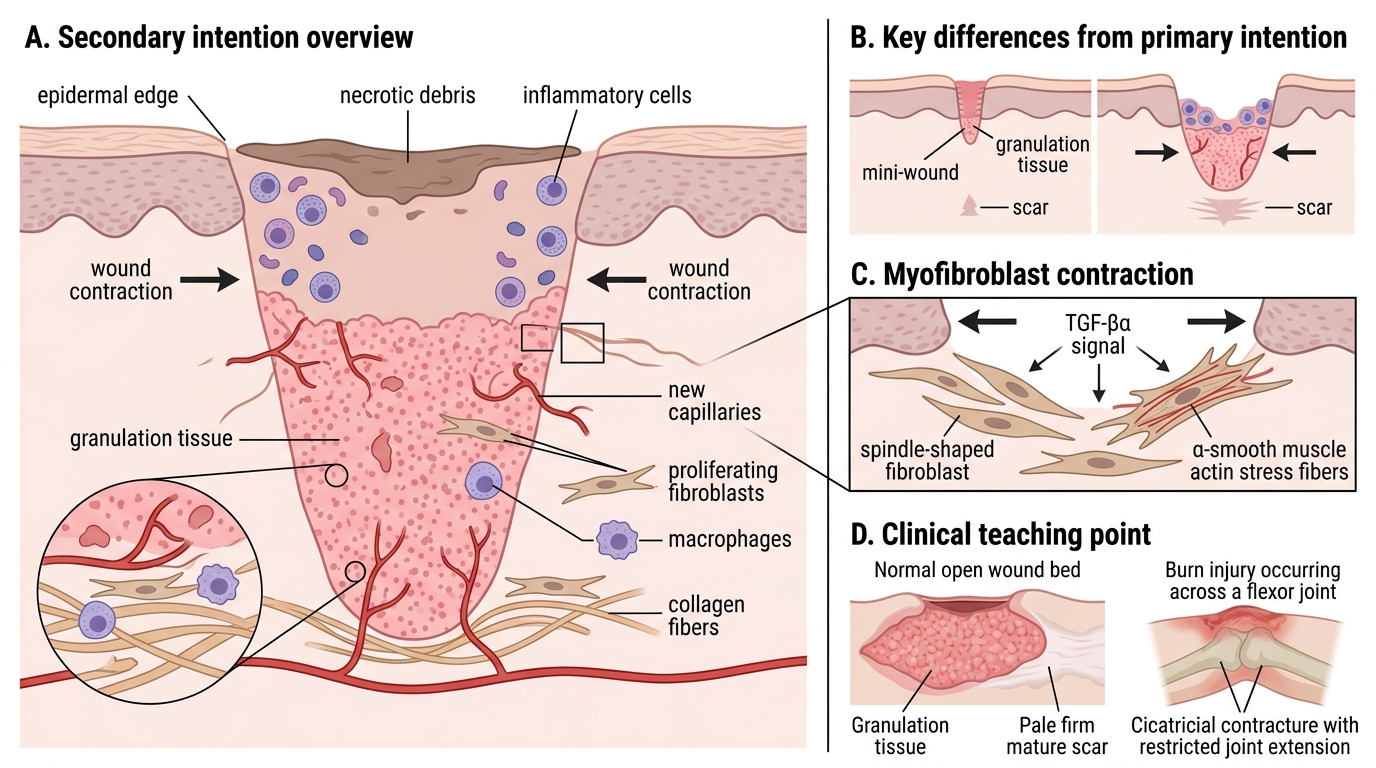
Wound Healing by Secondary Intention
Secondary intention (healing by second intention) occurs when wounds have:
• Large tissue defects that cannot be approximated (e.g., burn, abscess cavity, pressure ulcer)
• Infected wounds
• Wounds left open deliberately
Key differences from primary intention:
- More inflammation — extensive necrotic debris must be phagocytosed
- Abundant granulation tissue — fills the large defect from the base upward
- Wound contraction — a critical mechanism unique to large secondary wounds
Wound contraction is mediated by myofibroblasts — fibroblasts that acquire smooth-muscle-like actin filaments (α-smooth muscle actin, α-SMA) under TGF-β stimulation. They generate contractile force, drawing wound edges inward. This reduces the surface area requiring scar formation but can cause contracture if it overshoots.
- Larger, wider scar — more collagen deposited; scar may be hypertrophic
Clinical teaching point: The pink, granular, raised tissue filling an open wound bed IS healthy granulation tissue doing its job. The transition to pale, firm scar is maturation — not deterioration.
CLINICAL PEARL
Wound contraction vs cicatricial contracture — know the difference:
Wound contraction = normal, beneficial process during healing of large open wounds; myofibroblasts pull edges inward, reducing the wound area.
Contracture = a complication that occurs when wound contraction deforms a joint, digit, eyelid, or other functional structure. Burns across flexor surfaces of joints are the classic example. Prevention: early skin grafting, splinting in position of function, physiotherapy.
SELF-CHECK
A 45-year-old woman undergoes mastectomy. The wound is large and left to heal by secondary intention. Which cell type is primarily responsible for wound contraction?
A. Macrophages secreting TGF-β
B. Mast cells releasing histamine
C. Myofibroblasts expressing α-smooth muscle actin
D. Endothelial cells forming new capillaries
Reveal Answer
Answer: C. Myofibroblasts expressing α-smooth muscle actin
Myofibroblasts — fibroblasts induced by TGF-β to express α-smooth muscle actin — are the contractile effectors of wound contraction. They physically shorten, pulling wound edges toward the centre. Macrophages produce TGF-β (the inducer) but do not contract directly. Mast cells and endothelial cells play no direct role in contraction.