Page 13 of 25
PA4.1 | Healing & Repair — Regeneration, Granulation Tissue, Wound Healing — SDL Guide (Part 3)
Factors That Impair Wound Healing
Factors That Impair Wound Healing
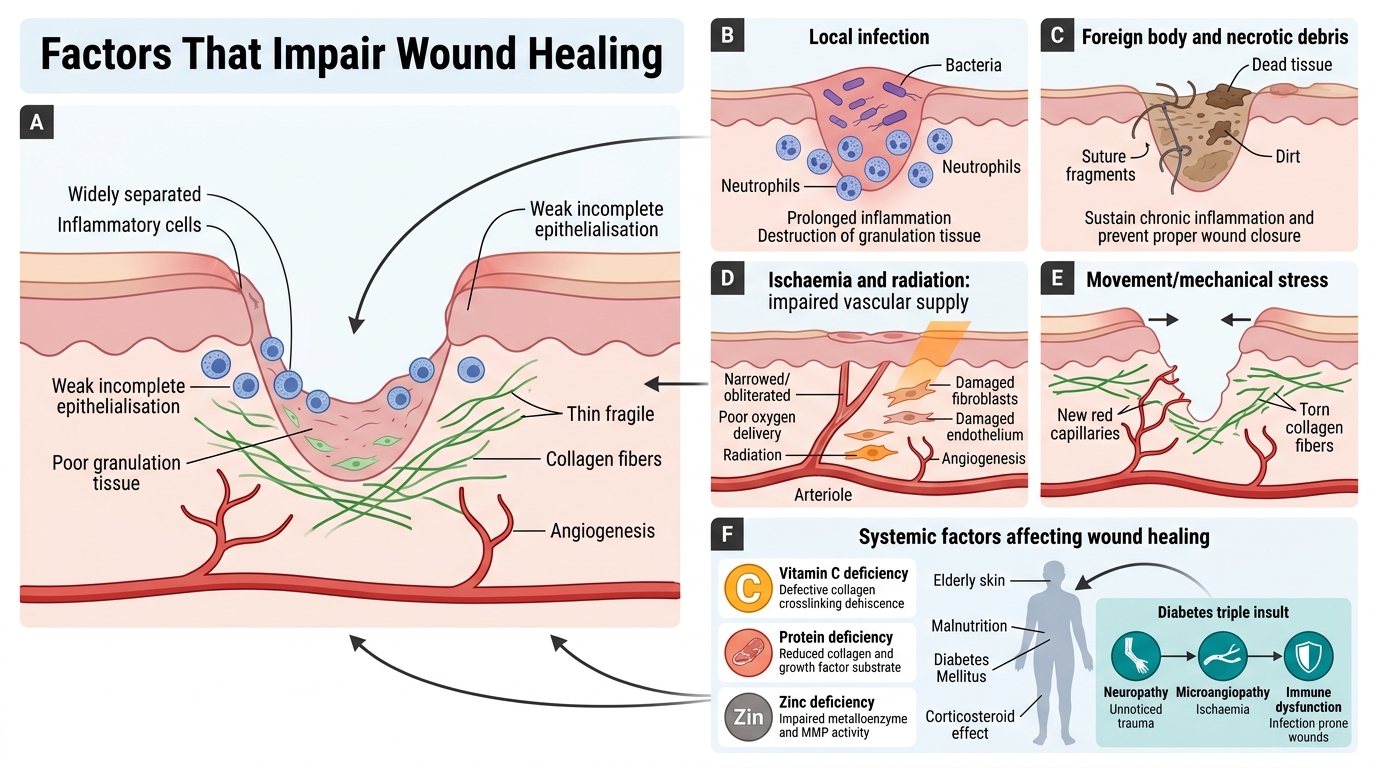
Local factors:
- Infection — the single most important local factor; bacteria prolong inflammation, destroy granulation tissue, and prevent epithelialisation
- Foreign body — sutures, debris, dead tissue — sustain inflammation and prevent closure (Virchow's triad of chronic inflammation)
- Ischaemia — inadequate blood supply deprives the wound of oxygen and nutrients; granulation tissue cannot form without angiogenesis
- Movement/mechanical stress — disrupts new capillaries and collagen deposition; immobilisation of fractures follows this principle
- Radiation — damages proliferating cells (fibroblasts, endothelium) and causes obliterative endarteritis
Systemic factors:
- Age — elderly patients heal more slowly: reduced angiogenesis, lower growth factor levels, thinner skin, comorbidities
- Nutrition:
- Vitamin C (ascorbate) deficiency → impaired collagen synthesis (ascorbate is essential for prolyl/lysyl hydroxylase enzymes that crosslink procollagen) → wound dehiscence, scurvy
- Protein deficiency → inadequate substrate for collagen and growth factor production
- Zinc deficiency → impaired metalloenzyme activity (many MMPs are zinc-dependent)
- Diabetes mellitus — triple insult: neuropathy (lack of sensation → unnoticed trauma), ischaemia (microangiopathy → poor blood supply), immune dysfunction (impaired neutrophil/macrophage function → infection-prone)
- Corticosteroids (glucocorticoids) — suppress inflammation, reduce fibroblast proliferation and collagen synthesis; mask infection signs; must taper before elective wound healing procedures
Complications and Aberrations of Repair
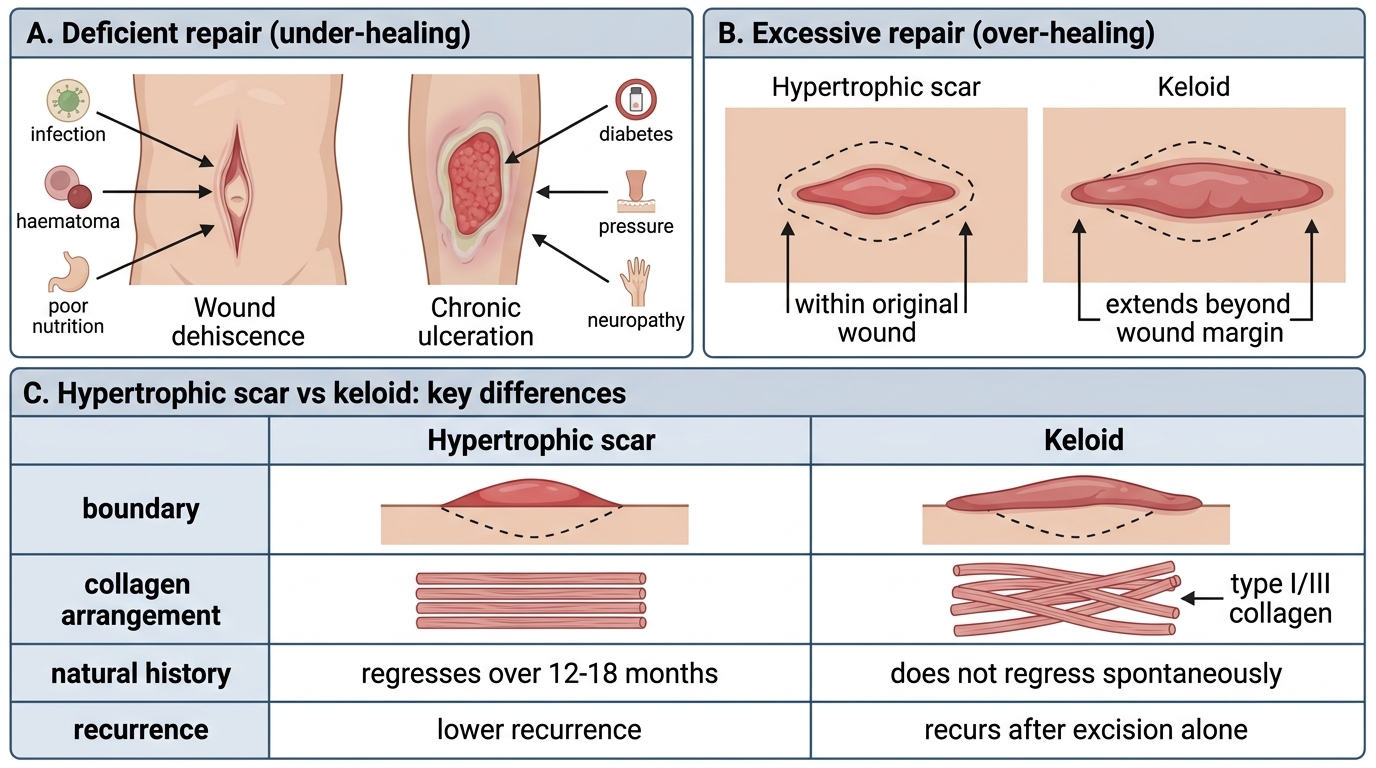
Deficient repair (under-healing):
- Wound dehiscence — failure of wound edges to hold together; common after abdominal surgery; precipitated by infection, haematoma, or poor nutrition
- Chronic ulceration — healing arrested; granulation tissue present but cannot progress; causes include ischaemia (arterial/venous), diabetes, pressure, neuropathy
Excessive repair (over-healing):
- Hypertrophic scar — raised, red scar confined within original wound boundaries; collagen bundles parallel to surface; tends to regress over 12-18 months; responds to pressure therapy
- Keloid — excessive scar that extends beyond original wound margins; type I/III collagen in thick, haphazard bundles; more common in darker-skinned individuals, chest/upper back/earlobes; does NOT regress spontaneously; recurs after excision alone
| Feature | Hypertrophic scar | Keloid |
|---|---|---|
| Boundary | Within wound | Exceeds wound margin |
| Regression | Yes, over time | No |
| Recurrence | Low | High (after excision) |
| Site preference | Any wound | Chest, earlobe, upper back |
| Ethnic predisposition | None | Darker skin types |
Complications and Aberrations of Repair
- Contracture — deforming wound contraction across joint/functional surface (discussed above under secondary intention)
- Desmoid tumour / aggressive fibromatosis — rare; uncontrolled proliferation of fibroblasts in abdominal wall or retroperitoneum; locally invasive, no metastasis
SELF-CHECK
A 22-year-old woman develops a firm, raised scar on her earlobe after ear piercing. The scar extends well beyond the piercing site. The most accurate characterisation is:
A. Hypertrophic scar — will regress over time without treatment
B. Keloid — confined within the wound boundary
C. Keloid — extends beyond the original wound margin and will not regress spontaneously
D. Contracture — caused by myofibroblast over-activity
Reveal Answer
Answer: C. Keloid — extends beyond the original wound margin and will not regress spontaneously
A keloid is defined by extension beyond the original wound margins — the key distinguishing feature from a hypertrophic scar, which stays within boundaries. Keloids do not regress spontaneously and are prone to recurrence after surgical excision alone. Earlobes, chest, and upper back are classic sites. Contracture involves joint/functional deformity by myofibroblast contraction, not scar overgrowth.
Timeline of Skin Wound Healing — A Consolidated View
Understanding the wound healing timeline helps you predict clinical findings at each follow-up visit:
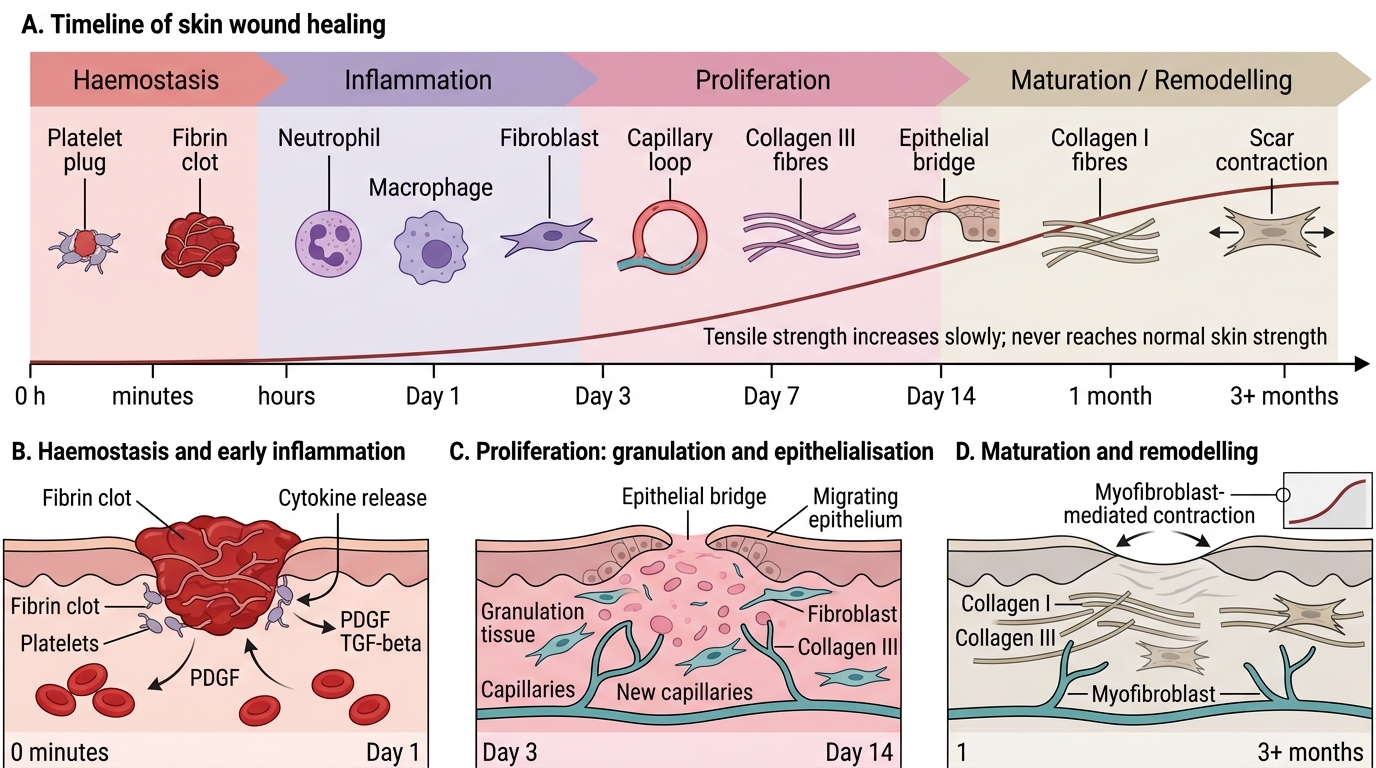
Timeline of Skin Wound Healing
| Phase | Time | Key events | Clinical correlation |
|---|---|---|---|
| Haemostasis | 0–minutes | Platelet plug → fibrin clot; PDGF, TGF-β released | Clot visible on day 1 |
| Inflammation | Hours–day 3 | Neutrophils → macrophages; debris clearance | Erythema, swelling — normal if resolving |
| Proliferation | Day 3–14 | Granulation tissue; fibroblast proliferation; collagen III; epithelialisation | Pink/red wound fill; epithelial bridge |
| Remodelling | Week 2–months | Collagen III → I; MMP activity; vascular regression; scar pales | Scar blanches, flattens, hardens |
Note: Tensile strength reaches ~50-60% by week 3, and plateaus at ~70-80% by month 3 — it never fully returns to unwounded tissue strength.