Page 14 of 25
PA4.1 | Healing & Repair — Regeneration, Granulation Tissue, Wound Healing — SDL Guide (Part 4)
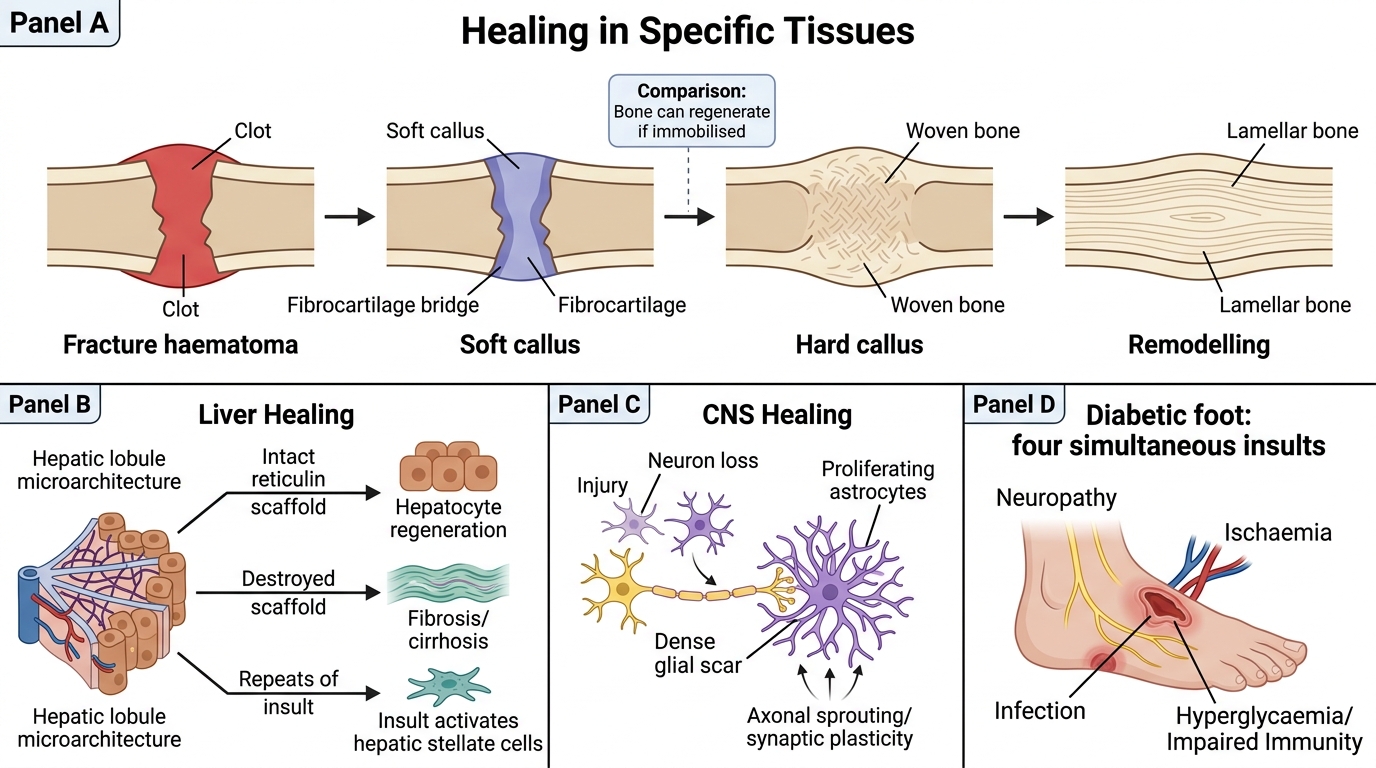
Healing in Specific Tissues
Healing in Specific Tissues
Bone fracture healing — a specialised form of repair combining both regeneration and connective-tissue repair:
- Fracture haematoma — immediate clot fills the fracture gap
- Soft callus — fibrocartilage produced by periosteal chondroblasts bridges the gap (weeks 1-3)
- Hard callus — woven bone replaces fibrocartilage (weeks 3-12); radiologically visible
- Remodelling — lamellar bone replaces woven bone; excess callus resorbed along lines of stress (months-years)
Key difference from skin: bone can undergo true regeneration (restore original architecture) if properly immobilised — because osteoprogenitor cells survive and the periosteal template remains.
Liver healing:
• Focal hepatocyte loss (viral hepatitis) + intact reticulin framework → hepatocyte regeneration
• Massive necrosis (fulminant hepatitis, large abscess) + destroyed framework → fibrosis/cirrhosis
• Repeated insults (alcohol, HBV/HCV) → progressive fibrosis driven by activated hepatic stellate cells (the liver's myofibroblast equivalent)
CNS healing (gliosis):
• Neurons are permanent cells — they cannot regenerate after loss
• Astrocytes proliferate and fill defects with a glial scar (gliosis)
• Functional recovery depends on axonal sprouting and synaptic plasticity, not parenchymal regeneration
• Implication: CNS infections, strokes, and trauma result in permanent neurological deficits unless plasticity compensates
CLINICAL PEARL
The diabetic foot — four simultaneous insults on wound healing:
A diabetic patient with a foot ulcer has:
1. Neuropathy → cannot feel pain → ignores the wound and keeps walking on it
2. Peripheral arterial disease → ischaemia → inadequate granulation tissue formation
3. Immune dysfunction → neutrophil and macrophage hypofunction → infection establishes and persists
4. Advanced glycation end-products (AGEs) → cross-link collagen abnormally → stiff, poorly remodelling tissue
This is why diabetic foot ulcers are the leading cause of non-traumatic lower-limb amputations worldwide — and why aggressive glycaemic control, vascular assessment, debridement, and offloading must all be addressed simultaneously.
SELF-CHECK
A surgical wound in a malnourished patient (serum albumin 2.1 g/dL, vitamin C deficient) breaks open on post-operative day 10. The most likely mechanism underlying this dehiscence is:
A. Impaired angiogenesis due to VEGF deficiency
B. Deficient collagen synthesis and cross-linking due to vitamin C deficiency
C. Excess MMP activity causing uncontrolled collagen degradation
D. Myofibroblast failure reducing wound contraction
Reveal Answer
Answer: B. Deficient collagen synthesis and cross-linking due to vitamin C deficiency
Vitamin C (ascorbate) is an obligatory cofactor for prolyl hydroxylase and lysyl hydroxylase — enzymes that hydroxylate procollagen residues, enabling triple-helix formation and cross-linking. Without it, collagen is structurally weak and wound tensile strength is severely compromised, leading to dehiscence. Protein deficiency worsens this by reducing substrate. Angiogenesis, MMP activity, and myofibroblast function are not the primary culprit here.