Page 16 of 25
PA3.4 | Inflammation Morphology — Practical — SDL Guide
Learning Objectives
- Identify the dominant inflammatory cell type in an H&E section and classify the inflammation as acute, chronic, or granulomatous
- Recognise the microscopic patterns of acute inflammation: suppurative/abscess, fibrinous, serous, ulcer, and phlegmon
- Describe the microscopic features of chronic inflammation including mononuclear infiltrate, fibrosis, and granulation tissue
- Identify a granuloma and name its key cellular components: epithelioid histiocytes, Langhans giant cells, lymphocyte cuff, and caseation
- Match gross appearances (abscess, fibrinous surfaces, chronic ulcer, granulomatous lymph nodes) to their microscopic counterparts
- Apply a systematic low-to-high-power reading strategy for inflammation specimens
INSTRUCTIONS
This practical module trains your eye for the most common pattern-recognition task in pathology: deciding, from a glass slide, whether inflammation is acute, chronic, or granulomatous. The skill directly underlies PA3.4 and is assessed in every university practical examination. Work through each section actively — pause at each micro_quiz before reading the explanation.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 3 (Acute and Chronic Inflammation) (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 4 (Inflammation) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
The registrar slides a haematoxylin and eosin (H&E) stained section under the microscope and says: 'Tell me — acute or chronic?' You have 30 seconds. The dominant cell is everything. This module gives you the pattern library to answer that question instantly, every time.
RECALL
Before you start, briefly recall from your Year-1 physiology:
• What are the five cardinal signs of acute inflammation and their vascular basis?
• Name the first cell to arrive at an acute inflammatory site.
• What is a monocyte's tissue name once it has emigrated?
Jot your answers — the microscopy will map directly onto these responses.
WHY THIS MATTERS
Every surgical specimen — an appendix, a lymph node, a lung lobe — comes to pathology with the question: what kind of inflammation is this, and how active is it? Your answer drives the clinician's choice between antibiotics, steroids, anti-TB therapy, or surgery. Pattern recognition on H&E is not an academic exercise; it is the first diagnostic act.
Reading Strategy: Low Power → High Power
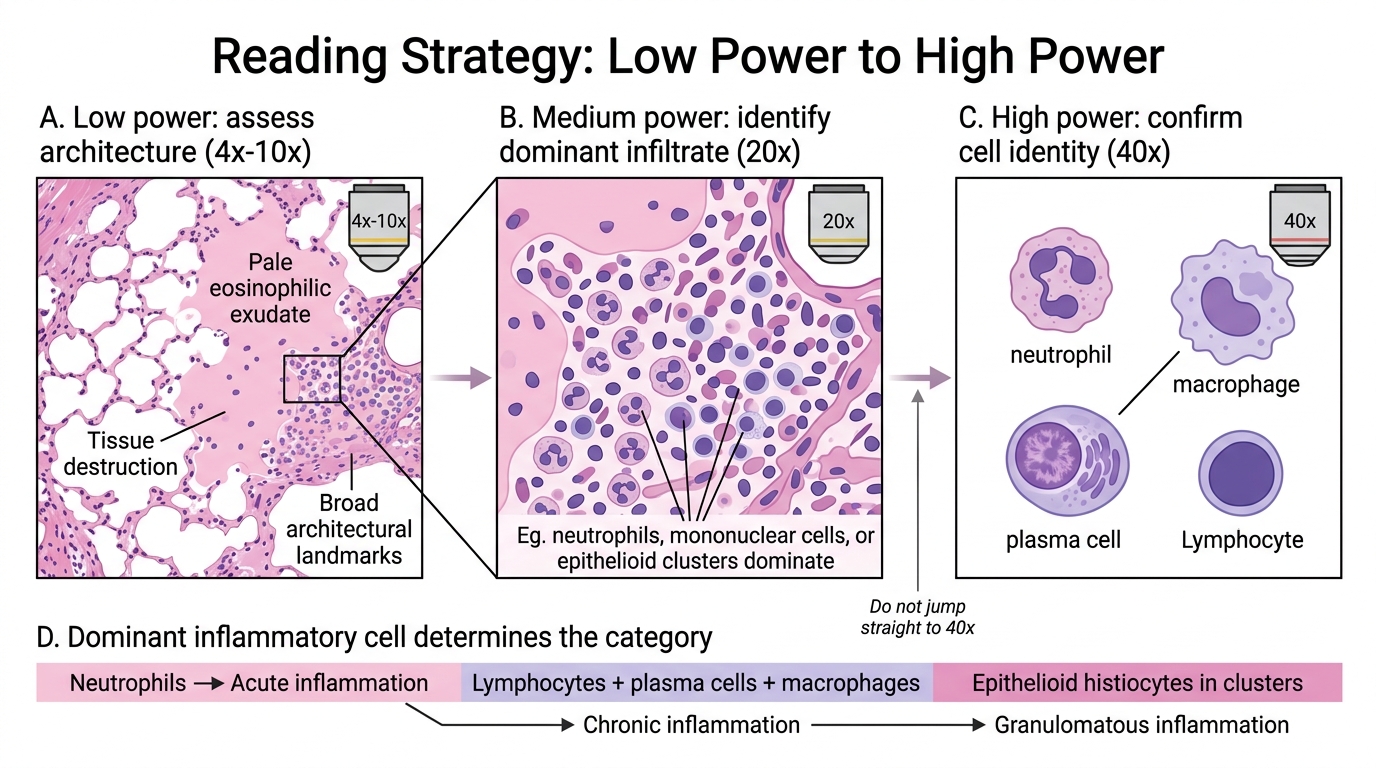
Low-to-High Power Reading Strategy in Inflammation
A disciplined reading sequence prevents missed diagnoses.
1. Low power (4×–10×): Assess architecture. Is the tissue normal? Is there destruction, exudate, or fibrosis? Identify any discrete collections or nodules.
2. Medium power (20×): Identify dominant cell type in the infiltrate (neutrophils vs. mononuclear cells vs. epithelioid clusters).
3. High power (40×): Confirm cell identity by nuclear morphology. Count: multilobed = neutrophil; kidney-shaped/oval = macrophage; clock-face chromatin = plasma cell; small dark round = lymphocyte.
The single most important question: what is the dominant inflammatory cell?
• Neutrophils → acute inflammation
• Lymphocytes, plasma cells, macrophages → chronic inflammation
• Epithelioid histiocytes in clusters → granulomatous inflammation
This low→high sequence is required in university practicals. Examaminers deduct marks for jumping straight to 40×.
SELF-CHECK
On low power you see a tissue section with diffuse pale eosinophilic material filling alveolar spaces plus small, dark-staining cells with multilobed nuclei. What is the dominant cell type and what category of inflammation does this represent?
A. Lymphocytes — chronic inflammation
B. Plasma cells — chronic inflammation
C. Neutrophils — acute inflammation
D. Epithelioid histiocytes — granulomatous inflammation
Reveal Answer
Answer: C. Neutrophils — acute inflammation
Multilobed (segmented) nuclei are the hallmark of neutrophils. Neutrophil dominance places this firmly in the acute inflammation category. The pale eosinophilic material in the alveoli is likely fibrinous or serous exudate — features of acute lobar pneumonia.
Acute Inflammation — Core Microscopic Features
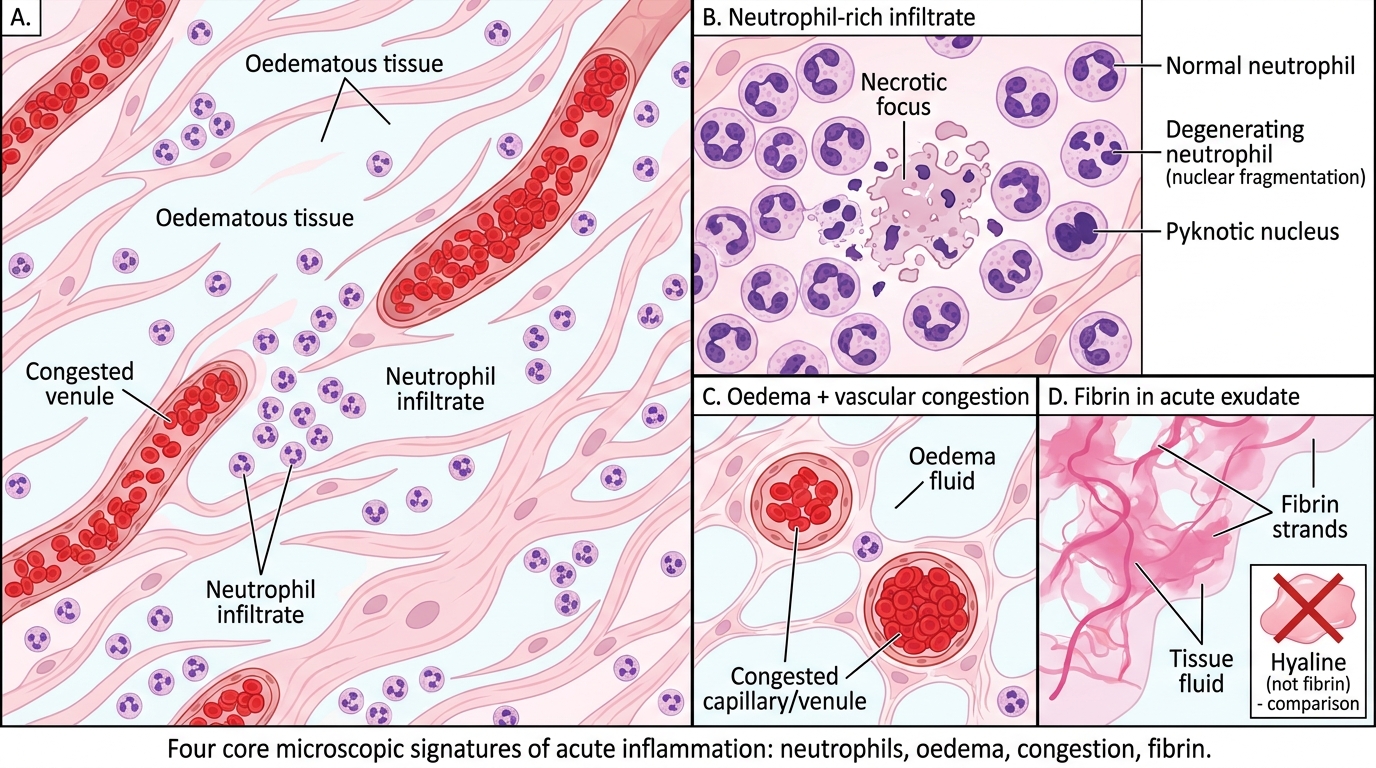
Core Microscopic Features of Acute Inflammation
Regardless of pattern, all acute inflammatory sections share four microscopic signatures:
- Neutrophil-rich infiltrate — multilobed nuclei, pink cytoplasm, often degenerating (karyorrhexis/pyknosis at the centre of necrosis)
- Oedema — pale, acellular space widening between cells and fibres (eosinophilic fluid in alveoli or interstitium)
- Vascular congestion — dilated, red-cell-packed capillaries and venules
- Fibrin — eosinophilic, amorphous to faintly fibrillar material; stains red-pink; distinct from homogeneous glass-like hyaline
These four features occur together in varying proportions across all acute patterns.
IMPORTAN: Karyorrhexis (nuclear fragmentation) in neutrophils indicates a very active, destructive process — note it when present.
Acute Patterns: Suppurative / Abscess
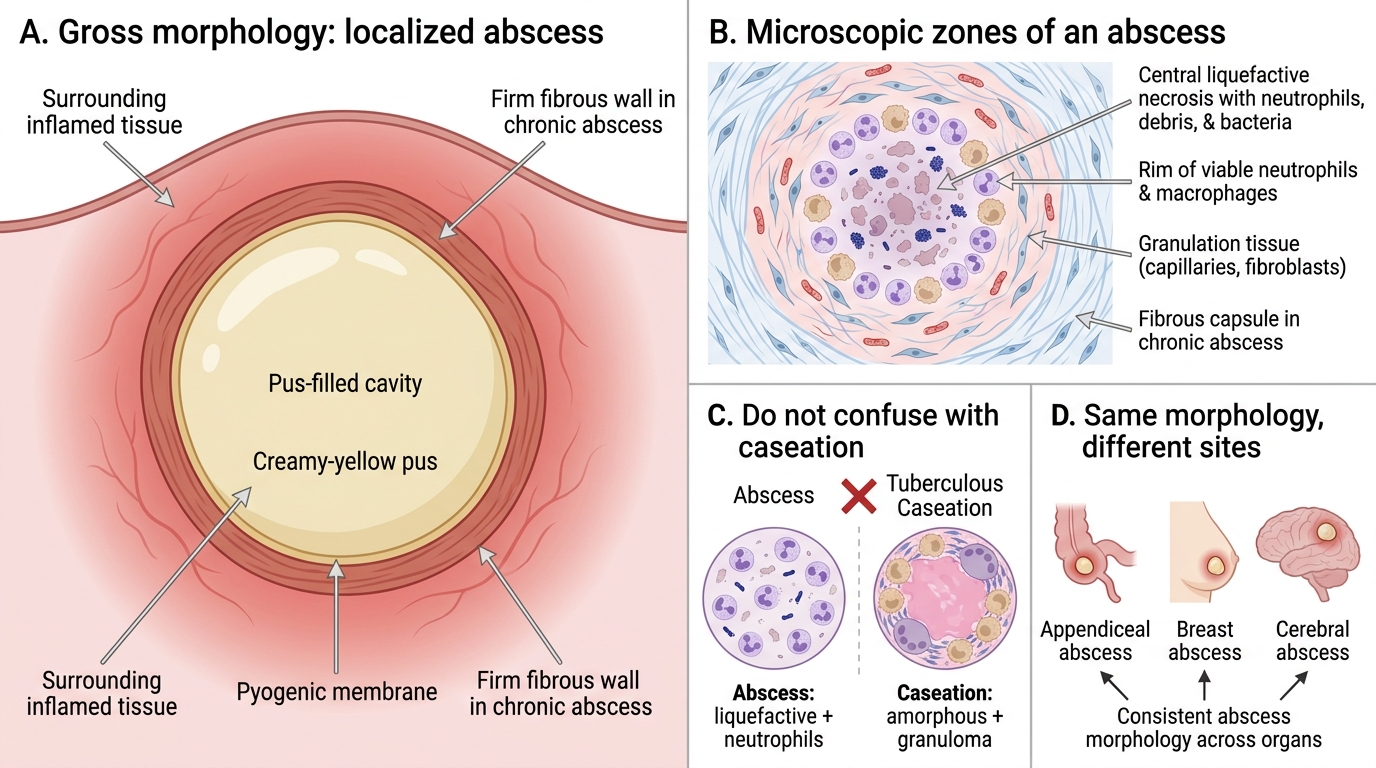
Suppurative Inflammation and Abscess Morphology
Suppurative inflammation is characterised by the formation of pus — a creamy mixture of dead and dying neutrophils, liquefied necrotic tissue, and tissue fluid.
Abscess = a localised collection of pus, walled off by a pyogenic membrane (inner zone of neutrophils and necrotic debris → outer zone of granulation tissue → outermost fibrous capsule in chronic abscess).
Microscopic hallmarks:
• Central zone: liquefactive necrosis with neutrophils (both viable and degenerate), cellular debris, and bacteria (may be visible as basophilic clumps)
• Rim: viable neutrophils, then macrophages beginning debris clearance
• Periphery: granulation tissue (new capillaries + fibroblasts) if the abscess is more than a few days old
Gross: pus-filled cavity with creamy-yellow content; walls may be firm in chronic abscess.
Clinical relevance: appendiceal abscess, breast abscess, cerebral abscess — all share this morphology.
IMPORTAN: Do not confuse liquefactive necrosis in an abscess with caseation in tuberculosis. Caseation is amorphous, cheese-like, and granuloma-associated; abscess necrosis is more cellular-ghost-rich and neutrophil-surrounded.