Page 17 of 25
PA3.4 | Inflammation Morphology — Practical — SDL Guide (Part 2)
Acute Patterns: Fibrinous and Serous
Fibrinous vs Serous Acute Inflammation
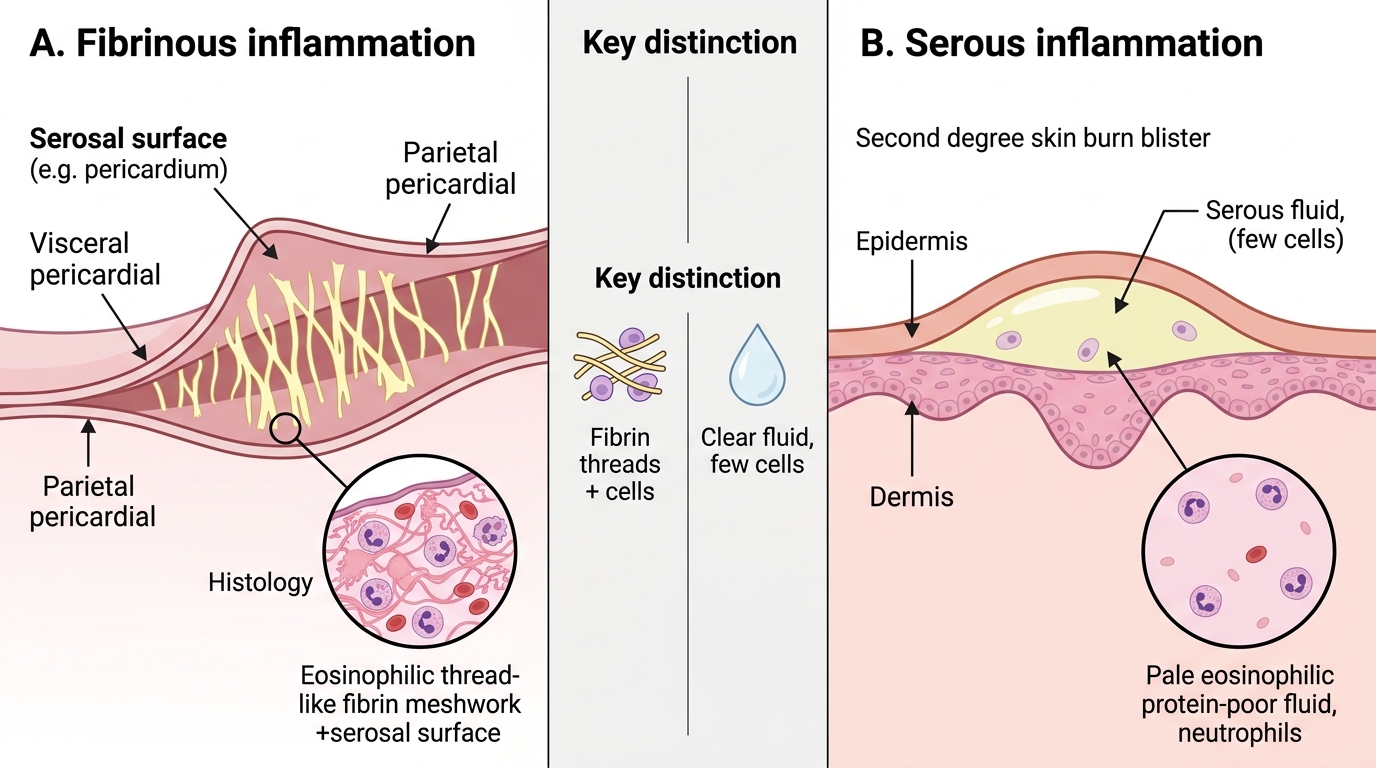
Fibrinous inflammation occurs when the vascular leak is large enough to allow high-molecular-weight fibrinogen to escape and polymerise as fibrin.
Microscopic: eosinophilic, thread-like or meshwork material on a serosal surface or within an organ; may contain trapped neutrophils and red cells.
Classic example: fibrinous pericarditis — the friction-rub lesion. Grossly described as 'bread-and-butter' pericarditis: when the pericardial surfaces are pulled apart they look like two pieces of buttered bread being separated. Microscopically: fibrin strands coat the visceral and parietal pericardium; neutrophils scattered within.
Serous inflammation involves a more dilute, protein-poor exudate with few cells.
Microscopic: pale eosinophilic fluid in body cavities or subepidermally (skin blisters); sparse neutrophils. Example: the blister of a second-degree burn, or an early viral pleuritis.
Distinction to know: fibrinous vs. serous — fibrin threads vs. clear fluid; fibrinous is more cellular and exudative.
SELF-CHECK
A slide shows eosinophilic thread-like material coating a serosal surface with scattered neutrophils. The gross description from the post-mortem report reads 'roughened, dull surface that peeled off in strings'. What is the pattern and what classic gross description applies?
A. Fibrinous pericarditis — 'bread-and-butter' appearance
B. Serous inflammation — 'honey-coloured crust'
C. Suppurative inflammation — 'pyogenic membrane'
D. Granulomatous inflammation — 'caseous necrosis'
Reveal Answer
Answer: A. Fibrinous pericarditis — 'bread-and-butter' appearance
Eosinophilic thread-like (fibrin) material on a serosal surface with neutrophils = fibrinous inflammation. On the pericardium, the two apposing fibrinous layers produce the classic 'bread-and-butter' gross appearance when separated. This is a favourite university examination spot-diagnosis.
Acute Patterns: Ulcer and Phlegmon
Acute Patterns: Ulcer and Phlegmon
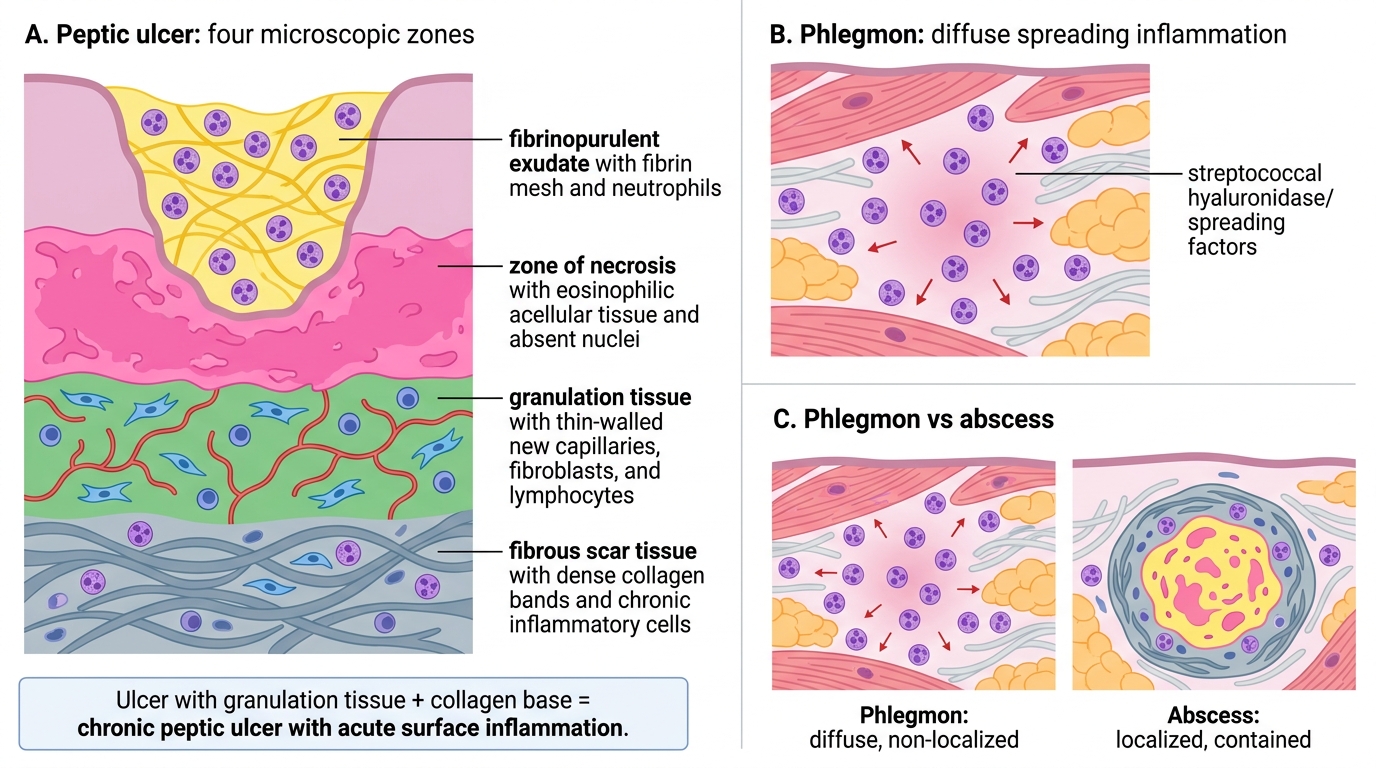
Ulcer = a local defect (excavation) of the surface of an organ produced by the sloughing of necrotic tissue.
Microscopic layers of a peptic ulcer (prototype):
1. Superficial: fibrinopurulent exudate (fibrin + neutrophils)
2. Below: zone of necrosis (eosinophilic, no viable nuclei)
3. Below: granulation tissue (thin-walled new capillaries, fibroblasts, lymphocytes)
4. Base: fibrous scar tissue (collagen bands, often with chronic inflammatory cells)
An ulcer spanning all four zones indicates a long-standing lesion — the granulation and fibrosis confirm chronicity even though the surface is acutely inflamed.
Phlegmon (cellulitis) = diffuse spreading acute inflammation through tissue planes, without localisation.
Microscopic: neutrophils diffusely infiltrating between muscle fibres, fat lobules, or dermal collagen — no central necrosis, no capsule. Streptococci produce spreading factors (hyaluronidase) that prevent walling-off.
Distinction: phlegmon spreads; abscess is contained.
SELF-CHECK
A gastric biopsy shows, from surface to base: fibrin + neutrophils → coagulative necrosis → new capillary buds with fibroblasts → dense collagen. The surface epithelium is absent. What is the diagnosis and what does the presence of collagen at the base indicate?
A. Acute erosion — collagen indicates normal gastric mucosa
B. Peptic ulcer — collagen indicates the lesion has a chronic fibrous base
C. Phlegmon — collagen indicates diffuse tissue infiltration
D. Suppurative gastritis — collagen indicates a pyogenic membrane
Reveal Answer
Answer: B. Peptic ulcer — collagen indicates the lesion has a chronic fibrous base
The classic four-layer sequence (fibrinopurulent exudate / necrosis / granulation tissue / fibrosis) is diagnostic of a peptic ulcer. The collagen at the base confirms chronicity — this is not an acute erosion. This distinction matters clinically because scarring can cause pyloric stenosis.
The Four Inflammation Patterns — H5P Image Hotspots Activity
Study the composite panel below. Each quadrant shows one pattern at representative H&E magnification. For each panel, identify the dominant cell and name the pattern before reading the label.
IMPORTAN: Look at each quadrant in sequence. Use the low-to-high strategy: start with the predominant colour and cellular density, then identify nuclear morphology.
IMPORTAN: After completing the hotspot activity, try to sketch (from memory) the nuclear shape that distinguishes a neutrophil from a macrophage.
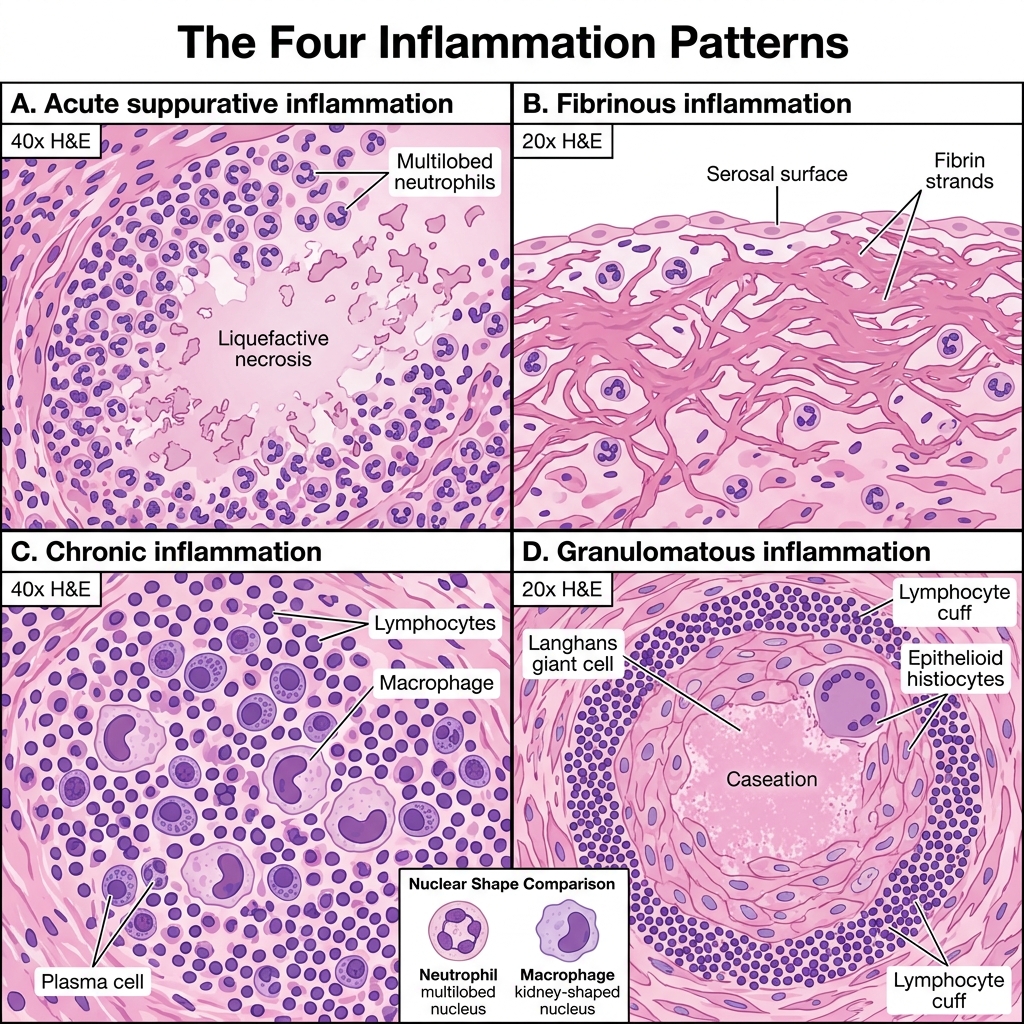
Four Patterns of Inflammation on H&E