Page 18 of 25
PA3.4 | Inflammation Morphology — Practical — SDL Guide (Part 3)
Chronic Inflammation — Microscopic Features
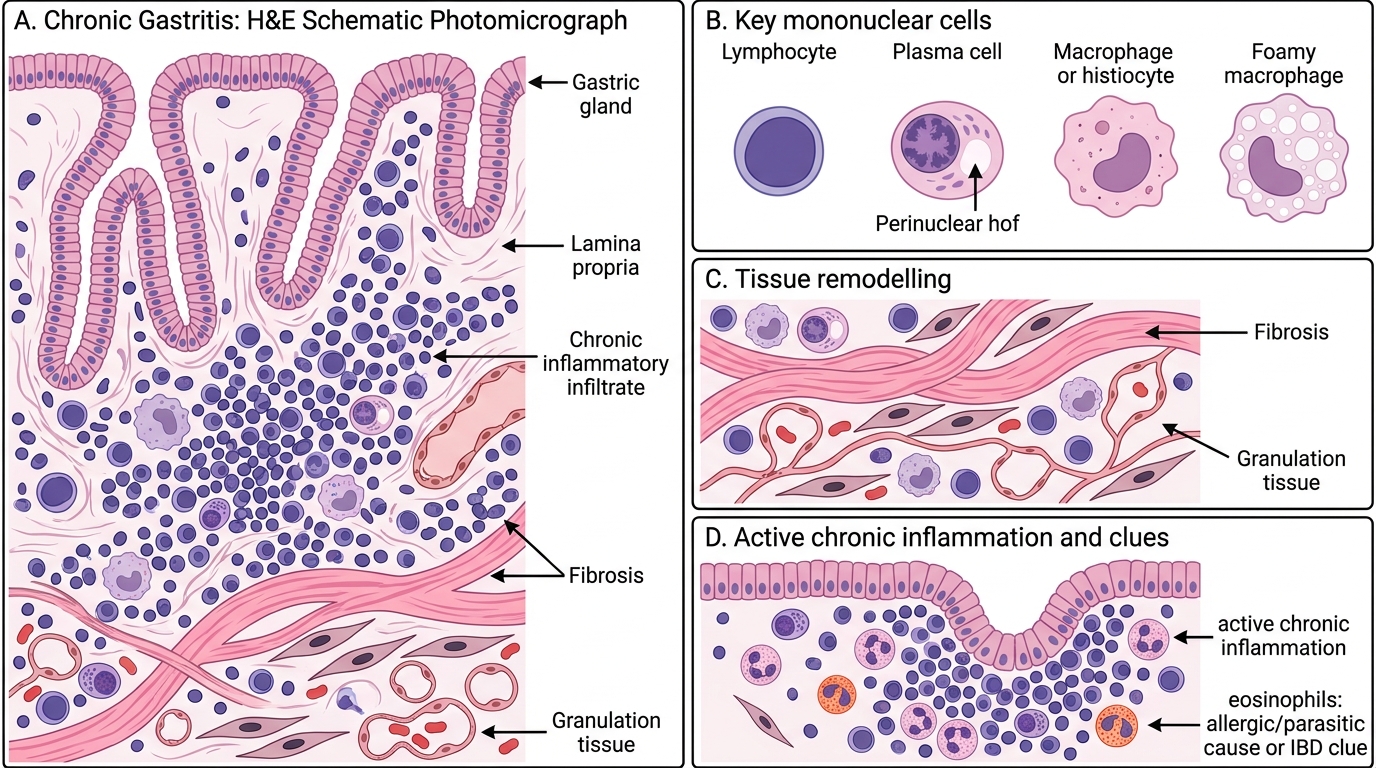
Chronic inflammation is defined by a mononuclear infiltrate — lymphocytes, plasma cells, and macrophages — often with tissue remodelling.
Key cells and their nuclear signatures:
• Lymphocyte: small, round, dark nucleus, scant cytoplasm — the most numerous cell in most chronic inflammatory infiltrates
• Plasma cell: eccentric nucleus with clock-face (cartwheel) chromatin and a clear perinuclear hof (Golgi zone) — the antibody-secreting cell
• Macrophage/histiocyte: kidney-shaped or oval nucleus, abundant pale cytoplasm — phagocytic workhorse; when activated, may show cytoplasmic vacuoles (lipid-laden 'foamy macrophage')
Associated tissue changes:
• Fibrosis: collagen deposition by activated fibroblasts — pink, acellular bands on H&E; indicates attempted repair
• Granulation tissue: combination of new thin-walled capillary loops, fibroblasts, and mixed inflammatory cells — the substrate of healing
• Glandular or epithelial hyperplasia in some chronic inflammatory sites (e.g. chronic gastritis)
Chronic inflammation often has scattered neutrophils too, especially at active ulcer edges — this is called 'active chronic inflammation' and is important to recognise in gastric and bowel biopsies.
IMPORTAN: Eosinophils in the infiltrate suggest allergic/parasitic aetiology or IBD — their presence is worth noting.
Chronic Inflammation: Microscopic Features
SELF-CHECK
You are examining a colonic biopsy. At 40× you see: cells with small dark round nuclei (most numerous), cells with eccentric nuclei showing peripheral clumped chromatin and a pale cytoplasmic zone, and occasional cells with kidney-shaped nuclei. There is also increased pink fibrous material between crypts. What is the most appropriate diagnosis?
A. Acute colitis — the dominant cell is neutrophil
B. Granulomatous colitis — the kidney-shaped nuclei indicate giant cells
C. Normal colonic mucosa — all cells described are physiological
D. Chronic inflammation with fibrosis — lymphocytes, plasma cells, and macrophages with collagen deposition
Reveal Answer
Answer: D. Chronic inflammation with fibrosis — lymphocytes, plasma cells, and macrophages with collagen deposition
Small dark round = lymphocytes; eccentric nucleus with clock-face chromatin + perinuclear hof = plasma cells; kidney-shaped = macrophages. Increased fibrous material = fibrosis. Together: chronic inflammation with fibrosis. The kidney-shaped nucleus of a macrophage must not be confused with a giant cell, which has multiple nuclei arranged in a specific pattern.
Granulomatous Inflammation — The Granuloma in Detail
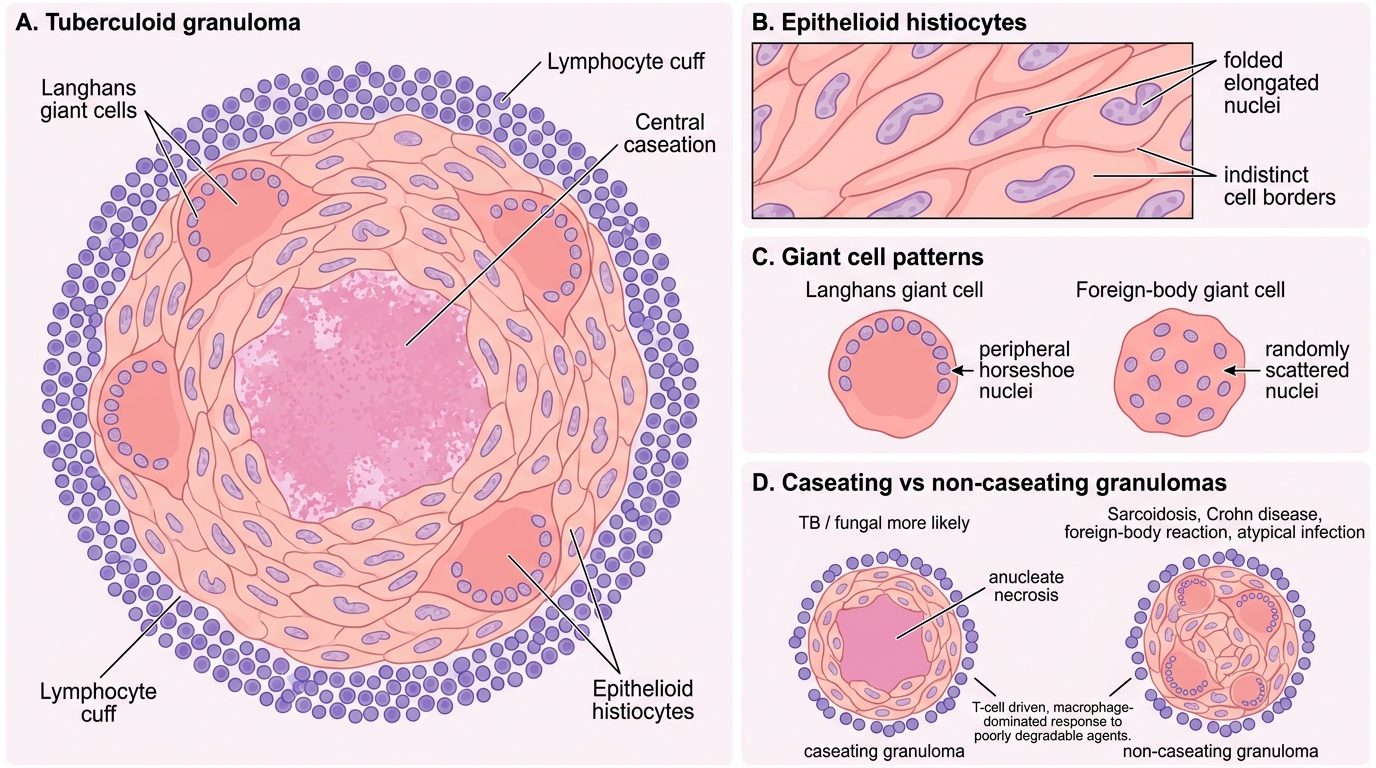
A granuloma is a focal aggregate of activated macrophages (epithelioid histiocytes) surrounded by lymphocytes, with or without giant cells and central necrosis.
Components of a tuberculoid granuloma (prototype):
- Epithelioid histiocytes (centre): elongated, pale/eosinophilic nuclei with folded margins, indistinct cell borders (cells appear to merge) — so named because they resemble epithelial cells
- Langhans giant cells: multinucleate macrophage fusions with nuclei arranged in a peripheral horseshoe or ring pattern — classically around the granuloma edge; MUST be distinguished from foreign-body giant cells (nuclei randomly scattered centrally)
- Central caseation: if present, strongly suggests TB or fungal aetiology; amorphous, pink, cheese-like, anucleate — no ghost outlines (unlike coagulative necrosis)
- Lymphocyte cuff: rim of small lymphocytes outside the epithelioid zone, maintaining the cell-mediated immune response
Granulomas WITHOUT caseation (non-caseating granulomas) suggest sarcoidosis, foreign-body reaction, Crohn's disease, or fungal/atypical mycobacterial infection.
Remember: the granuloma is a T-cell–driven, macrophage-dominated response — it means the agent is poorly degradable (TB bacilli, fungi, silica, suture material).
Tuberculoid Granuloma: Structure and Diagnostic Features
CLINICAL PEARL
Langhans vs. Foreign-body giant cell — a classic trap:
• Langhans giant cell: nuclei at the periphery in a horseshoe or ring → think TB/fungal granuloma
• Foreign-body giant cell: nuclei scattered centrally (haphazard) → think suture, silica, talc
The nuclear arrangement is the exam discriminator. The cell formation mechanism is the same (macrophage fusion), but the stimulus and clinical meaning differ completely.
SELF-CHECK
In a lymph node biopsy from a patient with cough and weight loss, you see: aggregates of pale, elongated cells with indistinct margins (resembling epithelium), ringed by small lymphocytes, with a central zone of structureless pink material. No nuclear ghost outlines are visible in the central zone. What are the cells, what is the central material, and what is the most likely aetiology?
A. Neutrophils / fibrinous exudate / bacterial lymphadenitis
B. Epithelioid histiocytes / caseation necrosis / tuberculosis
C. Plasma cells / amyloid / chronic lymphadenopathy
D. Reed-Sternberg cells / necrosis / Hodgkin lymphoma
Reveal Answer
Answer: B. Epithelioid histiocytes / caseation necrosis / tuberculosis
Pale elongated cells with indistinct margins in clusters = epithelioid histiocytes. Structureless pink material without nuclear ghosts = caseation necrosis (coagulative necrosis would retain ghost outlines; liquefactive necrosis would be more cellular-debris-rich). Caseating granuloma in a lymph node + constitutional symptoms = tuberculosis until proven otherwise.
Gross Pathology — Matching Macroscopic to Microscopic
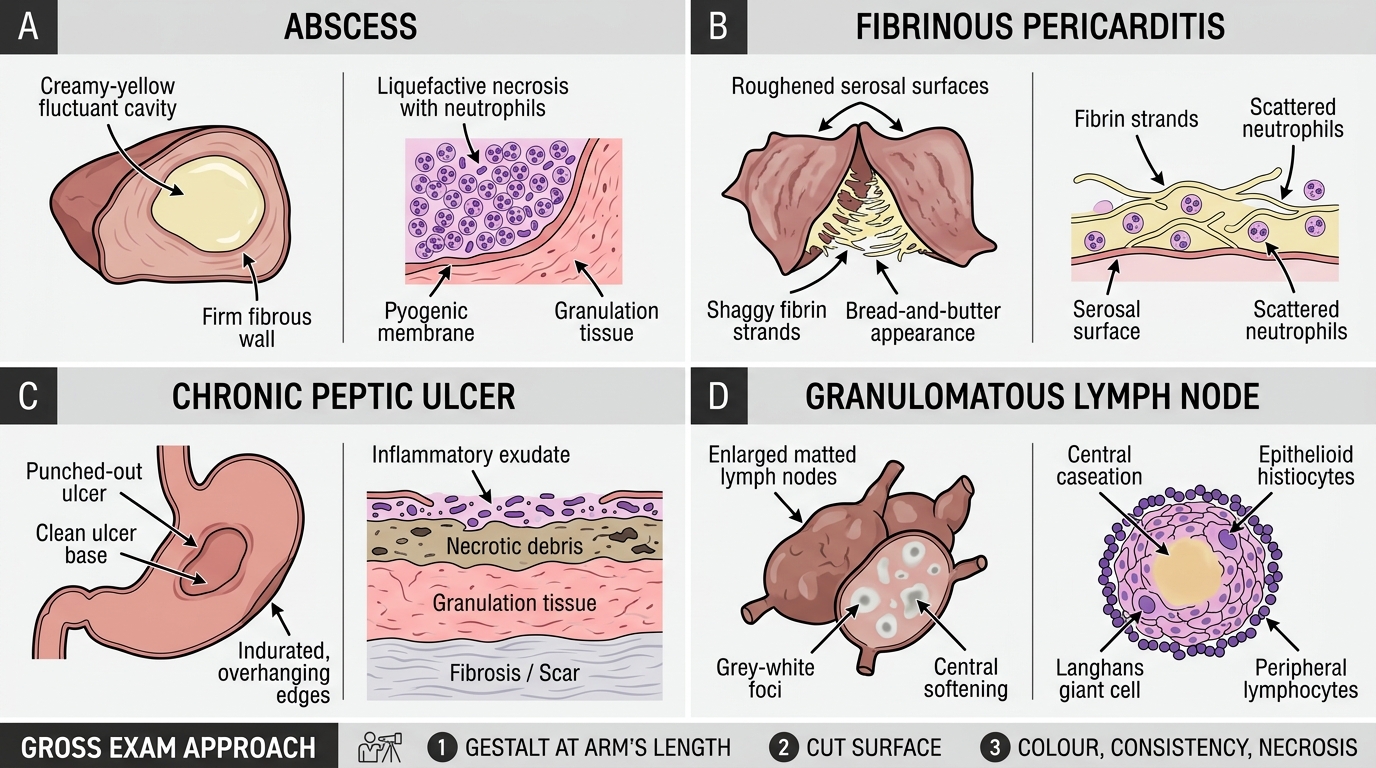
Gross recognition is tested in 'spot diagnosis' stations. Correlate each gross appearance with its microscopic counterpart:
| Gross appearance | Macroscopic clue | Microscopic correlate |
|---|---|---|
| Abscess | Creamy-yellow, fluctuant cavity; firm wall | Liquefactive necrosis + neutrophils; pyogenic membrane → granulation tissue |
| Fibrinous pericarditis | Roughened, shaggy, dull surfaces; 'bread-and-butter' when separated | Fibrin strands on serosal surface; scattered neutrophils |
| Chronic peptic ulcer | Oval punched-out base; indurated overhanging edges; clean base | Four-zone ulcer: exudate / necrosis / granulation tissue / fibrosis |
| Granulomatous lymph node | Enlarged, matted; cut surface shows grey-white foci, possibly central softening | Caseating granulomas: epithelioid cells + Langhans giant cells + lymphocytes + caseation |
Tip for gross exams: hold the specimen at arm's length first (gestalt impression), then examine the cut surface systematically: colour, consistency, margins, cavities.
Gross Pathology: Macroscopic Clues and Microscopic Correlates
SELF-CHECK
At a gross pathology station you are shown a lymph node cut surface with grey-white foci and one area of central softening. The examiner asks: 'What would you expect to see under the microscope?' Which answer is most complete?
A. Dense fibrin strands on a serosal surface with neutrophils — fibrinous pleuritis
B. Diffuse neutrophil infiltration with liquefactive necrosis — suppurative lymphadenitis
C. Epithelioid histiocytes in granulomas with Langhans giant cells, lymphocyte cuff, and central caseation — tuberculosis
D. Small dark lymphocytes replacing normal architecture — reactive hyperplasia
Reveal Answer
Answer: C. Epithelioid histiocytes in granulomas with Langhans giant cells, lymphocyte cuff, and central caseation — tuberculosis
Grey-white foci with central softening in a lymph node = caseating granulomas. Central softening = liquefaction of caseous material. Microscopically: epithelioid histiocytes + Langhans giant cells + caseation + lymphocyte cuff = tuberculoid granuloma. This is the most common gross-to-micro correlation in Indian university examinations for PA3.4.
Quick Differential at a Glance
Quick Differential of Inflammation Patterns
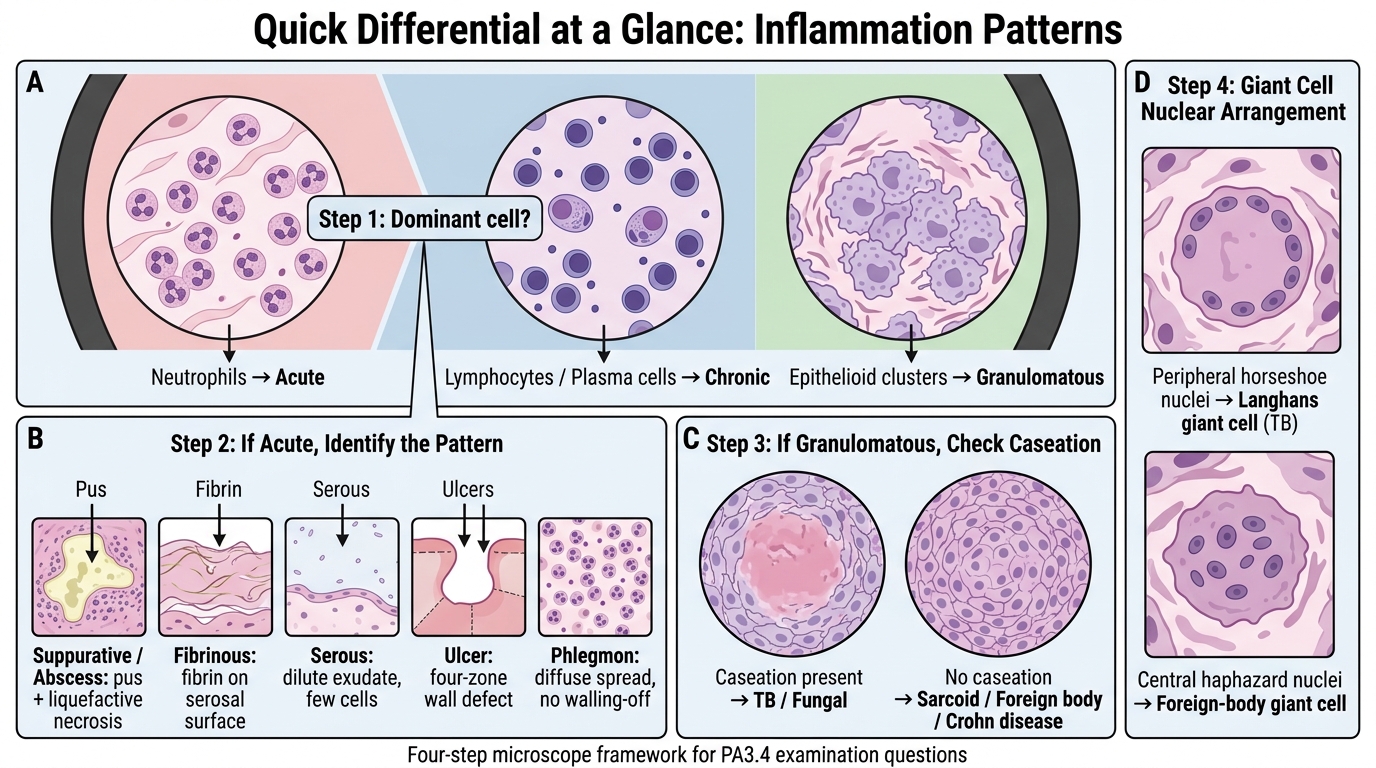
Use this decision tree at the microscope:
Step 1 — What is the dominant cell?
``
Neutrophils → ACUTE inflammation
Lymphocytes/Plasma cells → CHRONIC inflammation
Epithelioid clusters → GRANULOMATOUS inflammation
Step 2 — If ACUTE, what pattern?
`
Pus/liquefactive necrosis → Suppurative / Abscess
Fibrin on serosal surface → Fibrinous
Dilute exudate, few cells → Serous
Four-zone wall defect → Ulcer
Diffuse, no walling-off → Phlegmon
Step 3 — If GRANULOMATOUS, caseation present?
`
Yes (amorphous, anucleate) → TB / Fungal
No → Sarcoid / Foreign body / Crohn's
Step 4 — Check giant cell nuclear arrangement:
`
Peripheral horseshoe → Langhans (TB)
Central, haphazard → Foreign-body
This four-step framework answers 95% of PA3.4 examination questions.