Page 1 of 18
PA5.1-2 | Edema, Hyperemia, Congestion & Hemorrhage — SDL Guide
Learning Objectives
- Explain the Starling forces that govern fluid exchange across capillary walls and predict how their imbalance causes oedema
- Classify oedema by pathogenic mechanism and identify the characteristic clinical pattern each produces
- Distinguish a transudate from an exudate and state the diagnostic significance of each
- Compare active hyperaemia with passive congestion in terms of mechanism, colour, and histological appearance
- Describe the macroscopic and microscopic features of chronic venous congestion in the lung (heart-failure cells) and liver (nutmeg liver)
- Classify haemorrhage by type and site, and relate haemorrhage volume and location to its clinical consequences
INSTRUCTIONS
Fluid balance across capillary walls is a fundamental physical process — when it goes wrong it underpins some of the most common presentations in medicine: ankle swelling in heart failure, frothy sputum in pulmonary oedema, distended abdomen in cirrhosis. This module builds the mechanistic vocabulary that links a ward sign to a pathophysiological cause, and sets the foundation for every oedematous, congestive, and haemorrhagic disorder you will encounter in clinical years.
References
- Robbins & Kumar: Basic Pathology, 10th ed., Ch 4 — Hemodynamic Disorders, Thromboembolic Disease, and Shock (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 4 — Disturbances of Blood Flow and Circulation (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man with known ischaemic heart disease presents to casualty at 3 a.m. unable to lie flat, coughing up frothy pink sputum. His ankles have been swollen for weeks and his abdomen has begun to distend. Within sixty seconds of your examination you need to know: where is the fluid, why is it there, and is it going to kill him in the next hour? Every answer traces back to a few elegant physical forces and the vessels that contain them.
WHY THIS MATTERS
Oedema, congestion, and haemorrhage are three of the highest-yield topics in the PA5 block. They appear in university theory papers, clinical case vivas, and — most importantly — at the bedside of virtually every hospitalised patient. Mastering the Starling-force framework now gives you a single logical scaffold to hang dozens of individual diseases on for the rest of your clinical training.
RECALL
Before you begin, retrieve from your Year-1 physiology:
• What is the normal oncotic pressure of plasma, and which protein generates most of it?
• In which direction does hydrostatic pressure push fluid — into or out of the capillary?
• Name two lymphatic drainage territories that are clinically important when obstructed.
Hold these in mind — the pathology in this module is simply what happens when each of these parameters shifts in the wrong direction.
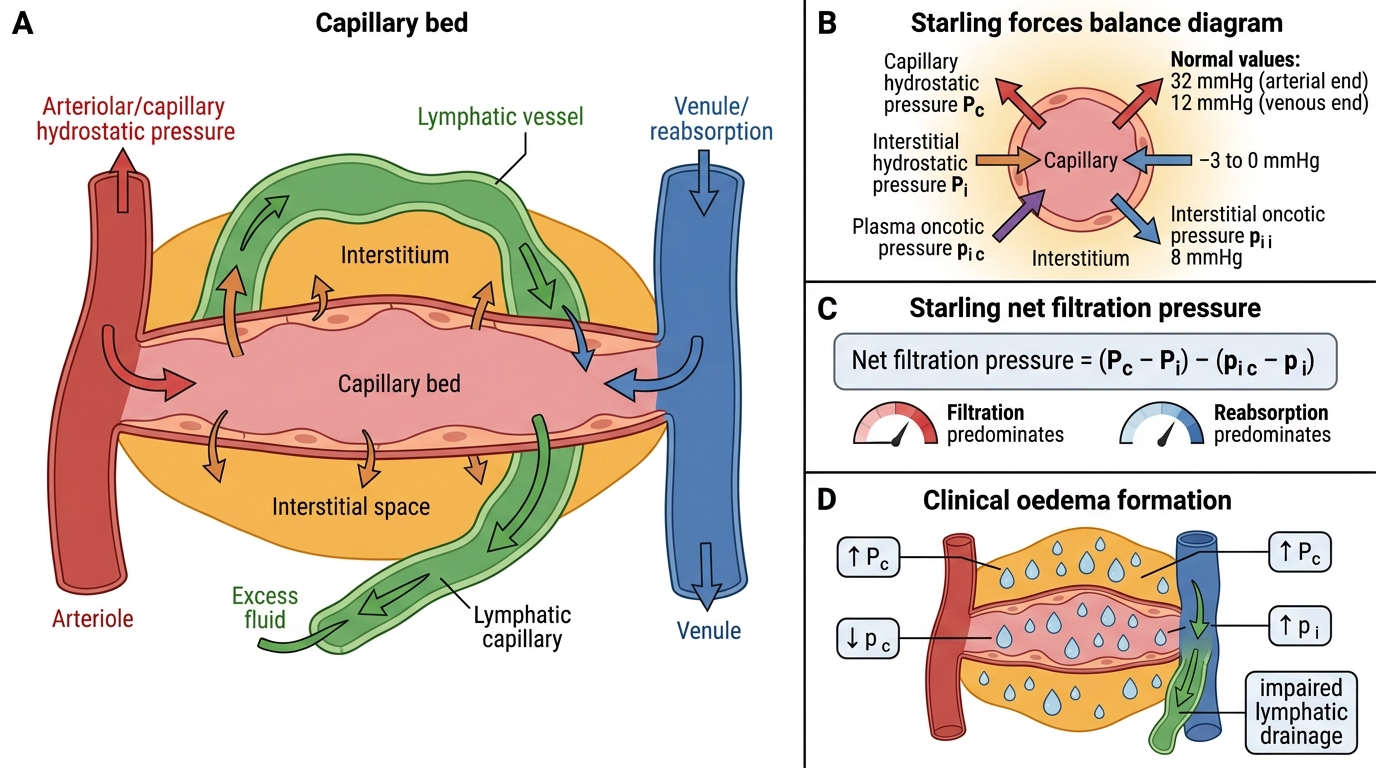
Starling Forces and the Physiology of Fluid Exchange
Fluid movement across the capillary wall is governed by four Starling forces:
| Force | Direction | Normal value |
|---|---|---|
| Capillary hydrostatic pressure (Pc) | Outward (filtration) | ~32 mmHg arteriolar end; ~12 mmHg venular end |
| Interstitial fluid hydrostatic pressure (Pi) | Inward (reabsorption) | −3 to 0 mmHg |
| Plasma oncotic pressure (πc) | Inward (reabsorption) | ~25 mmHg |
| Interstitial oncotic pressure (πi) | Outward | ~8 mmHg |
Net filtration pressure = (Pc − Pi) − (πc − πi). At the arteriolar end, filtration predominates; at the venular end, reabsorption predominates. The small net excess filtered (~20 L/day) is returned to the circulation by lymphatic drainage — the critical safety valve.
Oedema forms whenever net filtration exceeds lymphatic return capacity. This happens when one or more Starling forces shifts unfavourably or when lymphatic drainage is impaired.
Starling Forces and Capillary Fluid Exchange
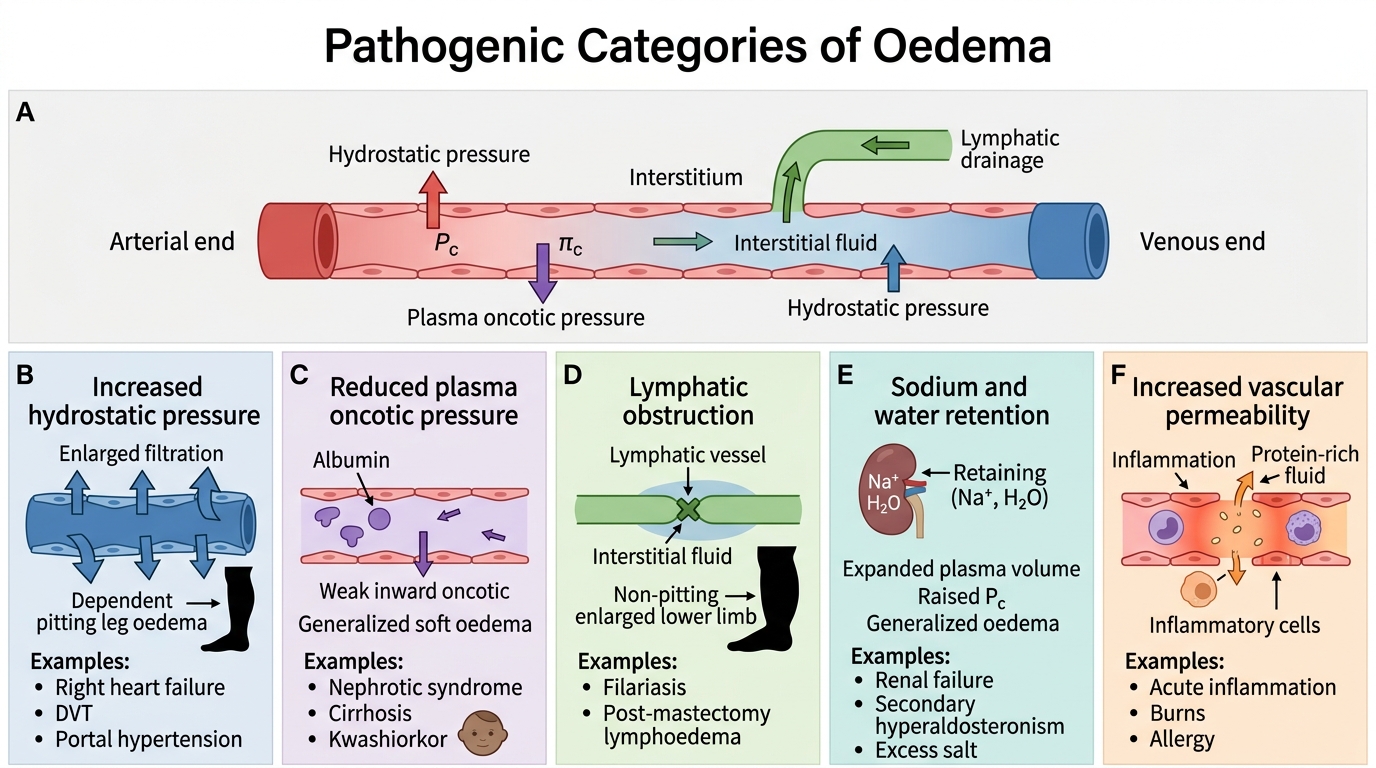
Pathogenic Categories of Oedema
Five distinct mechanisms produce oedema; each maps to one or more Starling force changes.
1. Increased hydrostatic pressure — Pc rises, tipping balance toward filtration.
- Right-heart failure: venous back-pressure elevates capillary hydrostatic pressure → dependent (pitting) oedema of legs, ascites.
- Venous obstruction (DVT, portal hypertension): localised or regional hydrostatic rise.
2. Reduced plasma oncotic pressure — πc falls, removing the inward-drawing force.
- Nephrotic syndrome: massive proteinuria → hypoalbuminaemia.
- Cirrhosis: failed hepatic albumin synthesis.
- Protein-energy malnutrition: kwashiorkor — characterised by pitting oedema in the face and lower limbs in a child with adequate caloric intake but severely deficient protein intake. The 'moon face' and pot-belly of kwashiorkor are classic clinical signs of hypoalbuminaemic oedema.
3. Lymphatic obstruction — lymphatic return abolished; even normal filtration accumulates.
- Filariasis (Wuchereria bancrofti): mosquito-borne nematode; chronic obliterative lymphangitis produces elephantiasis — massive, non-pitting oedema of the lower limbs, scrotum or vulva.
- Post-mastectomy/radiotherapy: lymph node removal or fibrosis → upper-limb lymphoedema.
4. Sodium and water retention — increased total body sodium obligates water, expanding plasma volume and raising Pc.
- Renal failure, secondary hyperaldosteronism (heart failure, cirrhosis), excess dietary salt.
5. Increased vascular permeability — inflammatory oedema; protein-rich fluid leaks through damaged endothelium, raising interstitial oncotic pressure (πi) and further drawing fluid out. This is the mechanism of the flare-and-wheal reaction, blister fluid, and septic oedema.
Pathogenic Categories of Oedema
SELF-CHECK
A 6-year-old child in a rural clinic has generalised pitting oedema, sparse reddish hair, and a distended abdomen. Serum albumin is 1.8 g/dL (normal: 3.5–5.0). Which Starling force derangement is the PRIMARY driver of oedema in this child?
A. Increased capillary hydrostatic pressure due to venous outflow obstruction
B. Reduced plasma oncotic pressure due to protein deficiency (kwashiorkor)
C. Lymphatic obstruction due to parasitic infection
D. Increased vascular permeability due to systemic inflammation
Reveal Answer
Answer: B. Reduced plasma oncotic pressure due to protein deficiency (kwashiorkor)
The child has kwashiorkor — protein-energy malnutrition with adequate calories but severe protein deficit. Hypoalbuminaemia reduces plasma oncotic pressure (πc), the main inward-drawing Starling force, so even normal capillary hydrostatic pressure results in net filtration and oedema accumulation. Venous obstruction (A) raises Pc. Lymphatic obstruction (C) does not depend on albumin levels. Inflammation (D) raises permeability but the clinical picture here is nutritional, not infective.
Transudate vs Exudate
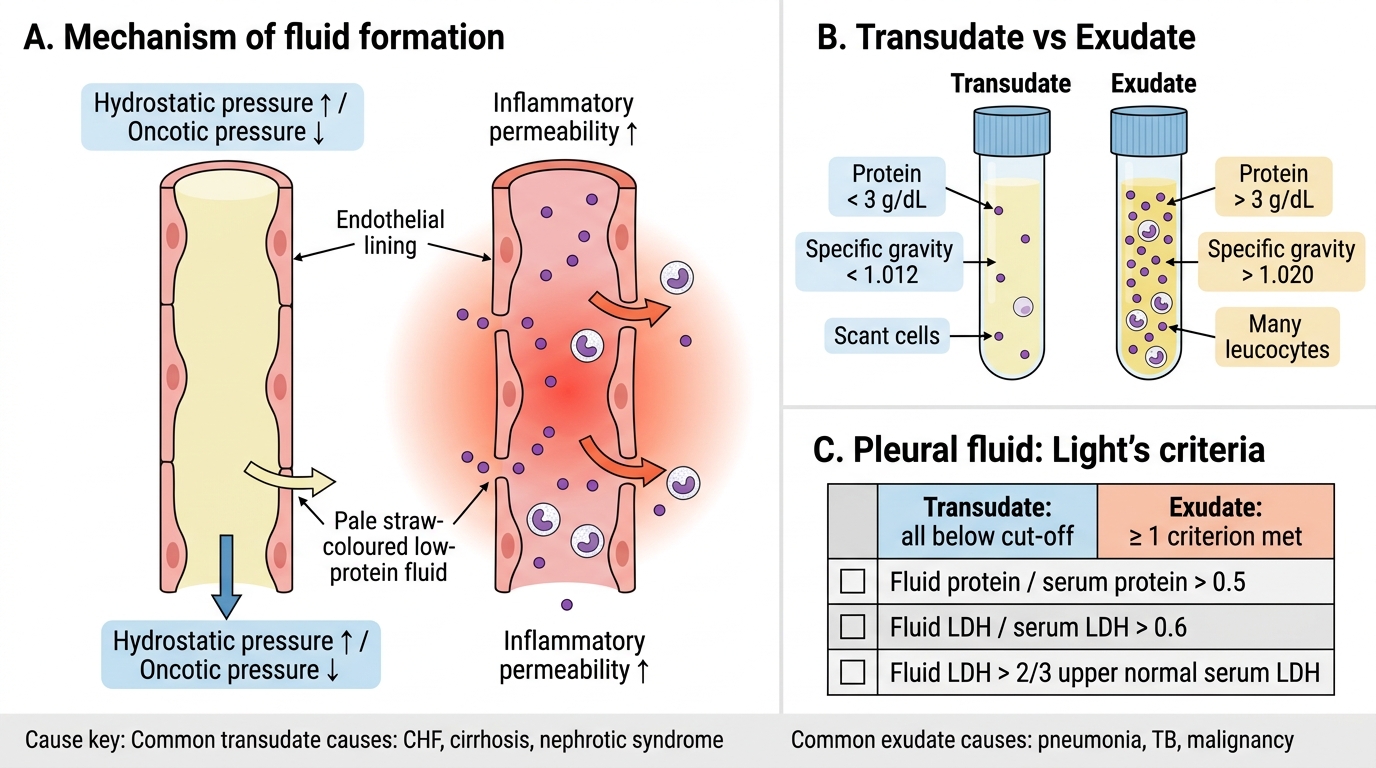
Transudate vs Exudate
The character of oedema fluid reflects its mechanism:
| Feature | Transudate | Exudate |
|---|---|---|
| Mechanism | Hydrostatic / oncotic imbalance | Inflammatory ↑ permeability |
| Protein content | < 3 g/dL (low) | > 3 g/dL (high) |
| Specific gravity | < 1.012 | > 1.020 |
| Cell count | Scant | Often many leucocytes |
| Light's criteria (pleural) | All three below cut-off | ≥ 1 criterion met |
| Causes | CHF, nephrotic, cirrhosis | Pneumonia, PE, malignancy, TB |
Light's criteria (protein fluid/serum, LDH fluid/serum, absolute LDH) are routinely used to classify pleural effusions. Transudates are managed by correcting the underlying physiology; exudates demand further workup for infection, infarction, or malignancy.