Page 2 of 18
PA5.1-2 | Edema, Hyperemia, Congestion & Hemorrhage — SDL Guide (Part 2)
Clinical Patterns of Oedema
Clinical Patterns of Oedema
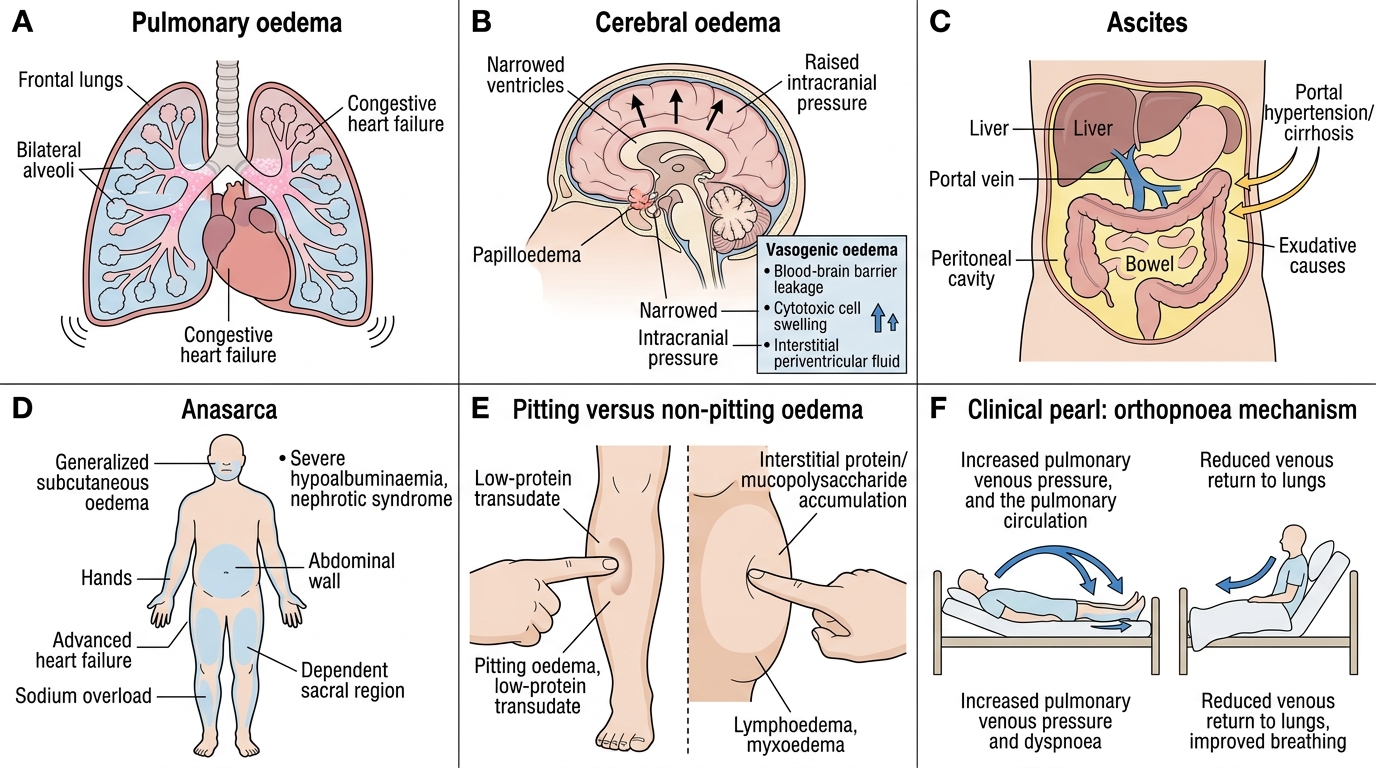
Recognising the distribution of oedema guides the diagnosis before any investigation:
- Pulmonary oedema: bilateral alveolar flooding; frothy pink (haemorrhagic) sputum, crepitations at lung bases; life-threatening; usually CHF or ARDS.
- Cerebral oedema: raised intracranial pressure; papilloedema, Cushing triad (hypertension + bradycardia + irregular respirations); vasogenic (BBB breakdown) vs cytotoxic (cell swelling) vs interstitial subtypes.
- Ascites: peritoneal fluid accumulation; portal hypertension (cirrhosis, right heart failure) or exudative (TB peritonitis, malignancy).
- Anasarca: generalised subcutaneous oedema — severe hypoalbuminaemia or total-body sodium overload (nephrotic syndrome, advanced heart failure).
- Pitting vs non-pitting oedema: pitting occurs when protein content is low (transudate in tissue); non-pitting occurs when protein or mucopolysaccharide accumulates in the interstitium — lymphoedema (elephantiasis), myxoedema (hypothyroidism, glycosaminoglycan deposition).
CLINICAL PEARL
The orthopnoea and paroxysmal nocturnal dyspnoea of left-heart failure both arise from redistribution: lying down shifts dependent oedema fluid into the pulmonary circulation, acutely worsening pulmonary venous pressure. Sitting upright reduces this redistribution — hence patients sleep with multiple pillows. Knowing this mechanism lets you infer the haemodynamic situation at the bedside without any imaging.
Hyperaemia vs Congestion — Active and Passive Vascular Engorgement
Hyperaemia vs Congestion
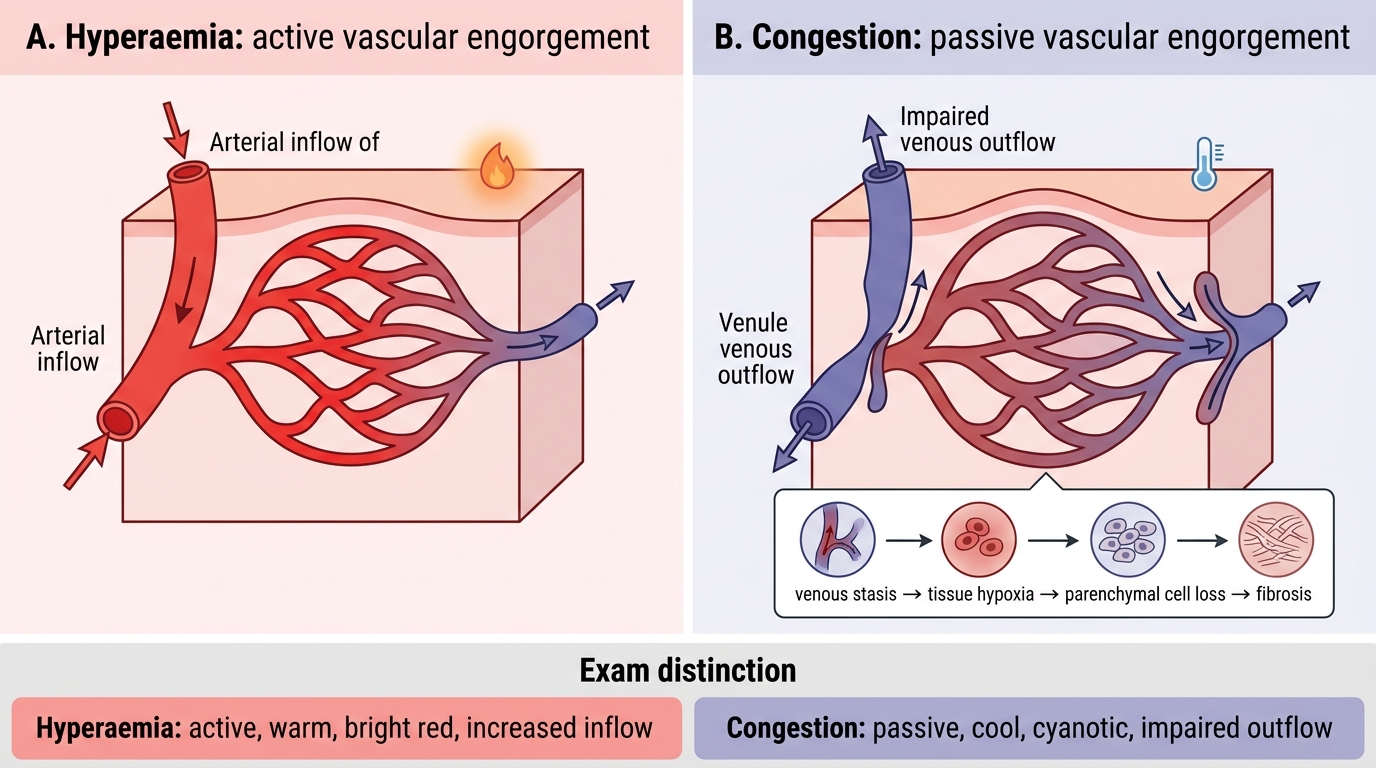
Both hyperaemia and congestion describe increased blood volume within a tissue, but they are mechanistically opposite:
Hyperaemia (active engorgement)
- Mechanism: arteriolar dilatation — increased inflow of oxygenated blood.
- Colour: bright red (erythema) — oxygen-rich haemoglobin.
- Causes: physiological (exercise, blushing, fever), inflammatory (vasodilators — histamine, prostaglandins), portal hyperaemia in early portal hypertension.
- Temperature: warm.
Congestion (passive engorgement)
- Mechanism: impaired venous outflow — blood dams back.
- Colour: dusky red-purple (cyanosis) — deoxygenated haemoglobin accumulates.
- Causes: heart failure, venous obstruction, compression.
- Temperature: cool (slow flow, heat loss).
- Acute congestion: vessel distension, minimal tissue damage.
- Chronic congestion: tissue hypoxia → parenchymal cell loss, fibrous replacement (chronic passive congestion).
Key distinction for exams: hyperaemia is an active, warm, red change; congestion is a passive, cool, cyanotic change.
Chronic Venous Congestion — Lung and Liver
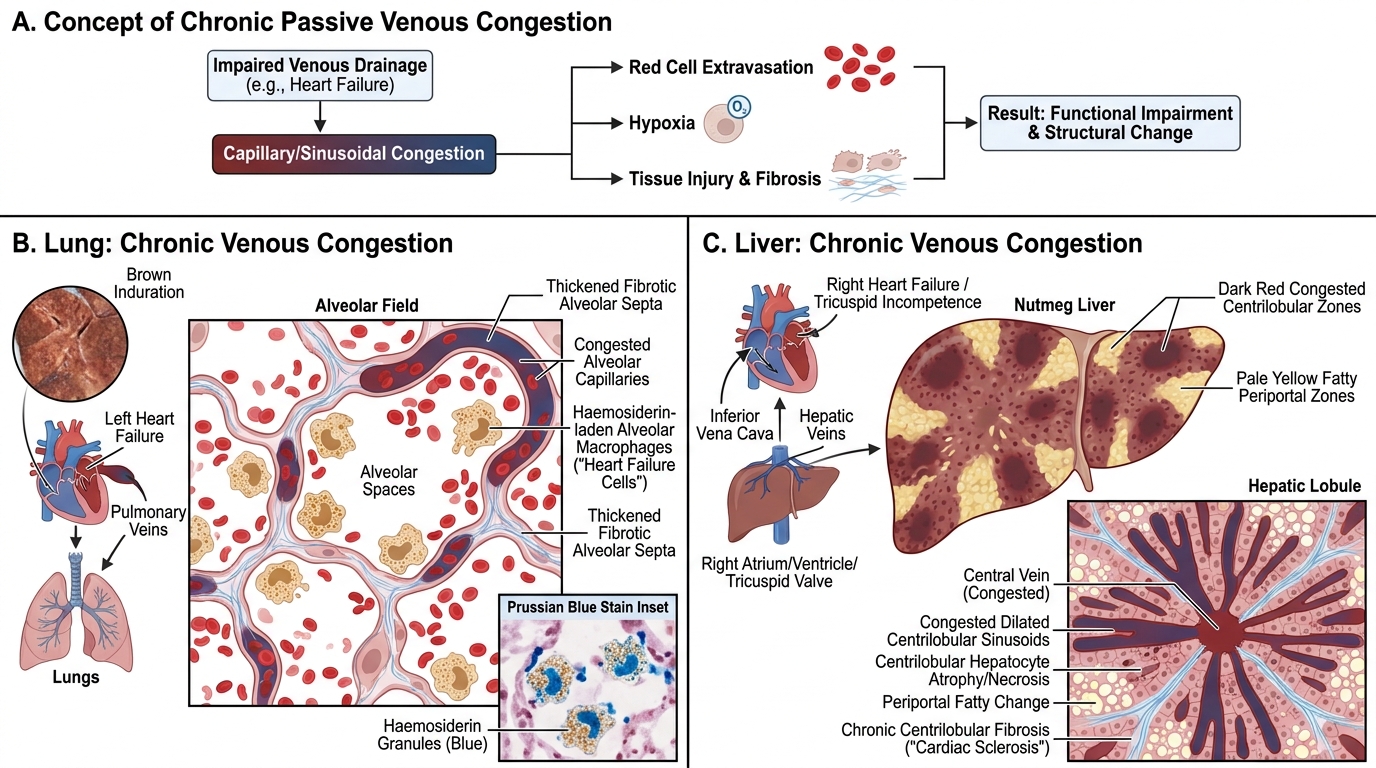
Chronic passive congestion produces characteristic macroscopic and microscopic changes in target organs:
Lung (chronic venous congestion — left heart failure)
- Macroscopic: brown induration — firm, brown discolouration.
- Microscopic:
- Alveolar capillaries distended with red cells.
- Red cells extravasate into alveoli → haemoglobin → haemosiderin.
- Alveolar macrophages engulf haemosiderin → heart failure cells (haemosiderin-laden macrophages); seen in sputum (Prussian blue positive) and BAL.
- Fibrous thickening of alveolar walls (reactive fibrosis from chronic hypoxia).
Liver (chronic venous congestion — right heart failure or tricuspid incompetence)
- Macroscopic: nutmeg liver — alternating dark red congested centrilobular zones and paler, fatty periportal zones give the cut surface a speckled, nutmeg appearance.
- Microscopic:
- Centrilobular sinusoidal dilatation and congestion.
- Centrilobular hepatocyte atrophy/necrosis (most vulnerable — furthest from portal blood supply).
- Periportal hepatocytes show fatty change (relative anoxia + fatty acids from gut).
- Chronic: cardiac sclerosis (cardiac cirrhosis) — centrilobular fibrosis extending between lobules; true cirrhosis rare unless coexistent disease.
Chronic Venous Congestion: Lung and Liver
SELF-CHECK
A 65-year-old woman with longstanding right heart failure dies. At autopsy, the liver cut surface shows a mottled appearance with alternating dark red and pale yellow-brown zones. Microscopically, centrilobular sinusoids are dilated and the centrilobular hepatocytes are atrophied. What is the MOST accurate term for this gross finding?
A. Focal nodular hyperplasia
B. Nutmeg liver
C. Hepatic steatosis
D. Budd-Chiari syndrome
Reveal Answer
Answer: B. Nutmeg liver
The alternating dark red (congested centrilobular) and pale (fatty periportal) zones on the cut surface of a chronically congested liver resemble the cross-section of a nutmeg — hence the term nutmeg liver. This is the classic macroscopic finding of chronic passive hepatic congestion due to right heart failure or tricuspid insufficiency. Focal nodular hyperplasia (A) is a benign hepatic mass with a central scar. Hepatic steatosis (C) produces diffuse yellow discolouration without the red-and-pale zonal pattern. Budd-Chiari syndrome (D) involves hepatic vein thrombosis and can cause congestion but is distinguished clinically.