Page 3 of 18
PA5.1-2 | Edema, Hyperemia, Congestion & Hemorrhage — SDL Guide (Part 3)
Haemorrhage — Types, Causes, and Significance
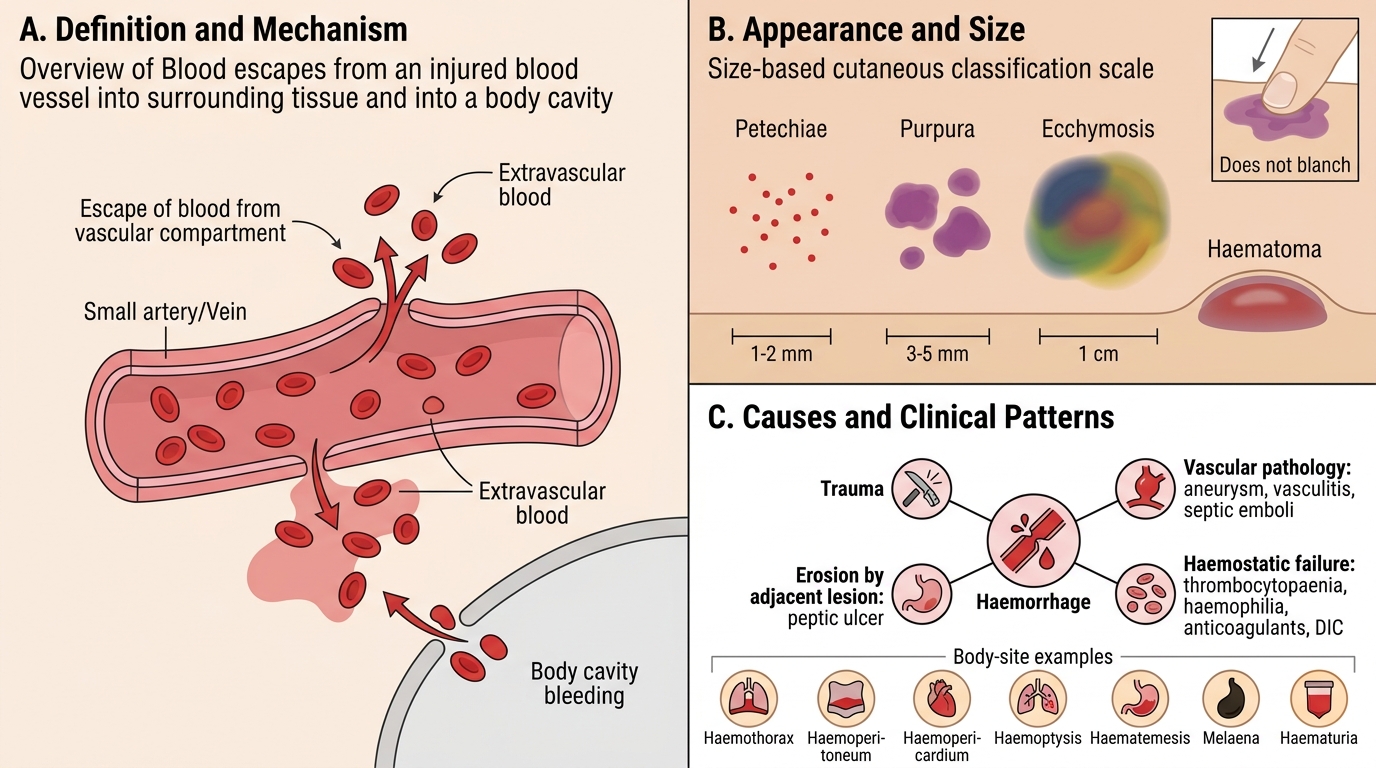
Haemorrhage is the escape of blood from the vascular compartment. It is classified by site, size, mechanism, and temporal pattern.
Classification by appearance and size:
- Petechiae: pinpoint haemorrhages (1–2 mm), skin, mucous membranes, serosal surfaces; seen in thrombocytopaenia, vasculitis, rickettsial infections.
- Purpura: larger (3–5 mm+) patches of cutaneous haemorrhage; do not blanch on pressure (differentiates from reactive hyperaemia).
- Ecchymoses: large (>1 cm) bruises — black eye, subcutaneous trauma; colour shifts from blue-black (haemoglobin) → green (biliverdin) → yellow-brown (haemosiderin) as macrophages phagocytose and process red cells.
- Haematoma: blood accumulating within tissue (e.g., subdural haematoma, intramuscular haematoma); may cause mass effect.
- Haemothorax / haemoperitoneum / haemopericardium: blood in body cavities.
- Haemoptysis: coughing up blood — pulmonary or bronchial source.
- Haematemesis: vomiting blood — upper GI source.
- Melaena: black, tarry stool from digested upper GI blood.
- Haematuria: blood in urine — renal, ureteric, or bladder source.
Causes of haemorrhage:
1. Trauma — most common.
2. Vascular pathology — atherosclerosis (aneurysm rupture), vasculitis, septic emboli (mycotic aneurysm).
3. Haemostatic failure — thrombocytopaenia, coagulation factor deficiency (haemophilia), anti-coagulant drugs, DIC.
4. Erosion by adjacent pathology — peptic ulcer eroding gastric artery, tumour invasion of vessel wall.
Haemorrhage: Types, Causes, and Significance
Clinical Significance of Haemorrhage — Volume, Site, and Rate
Clinical Significance of Haemorrhage
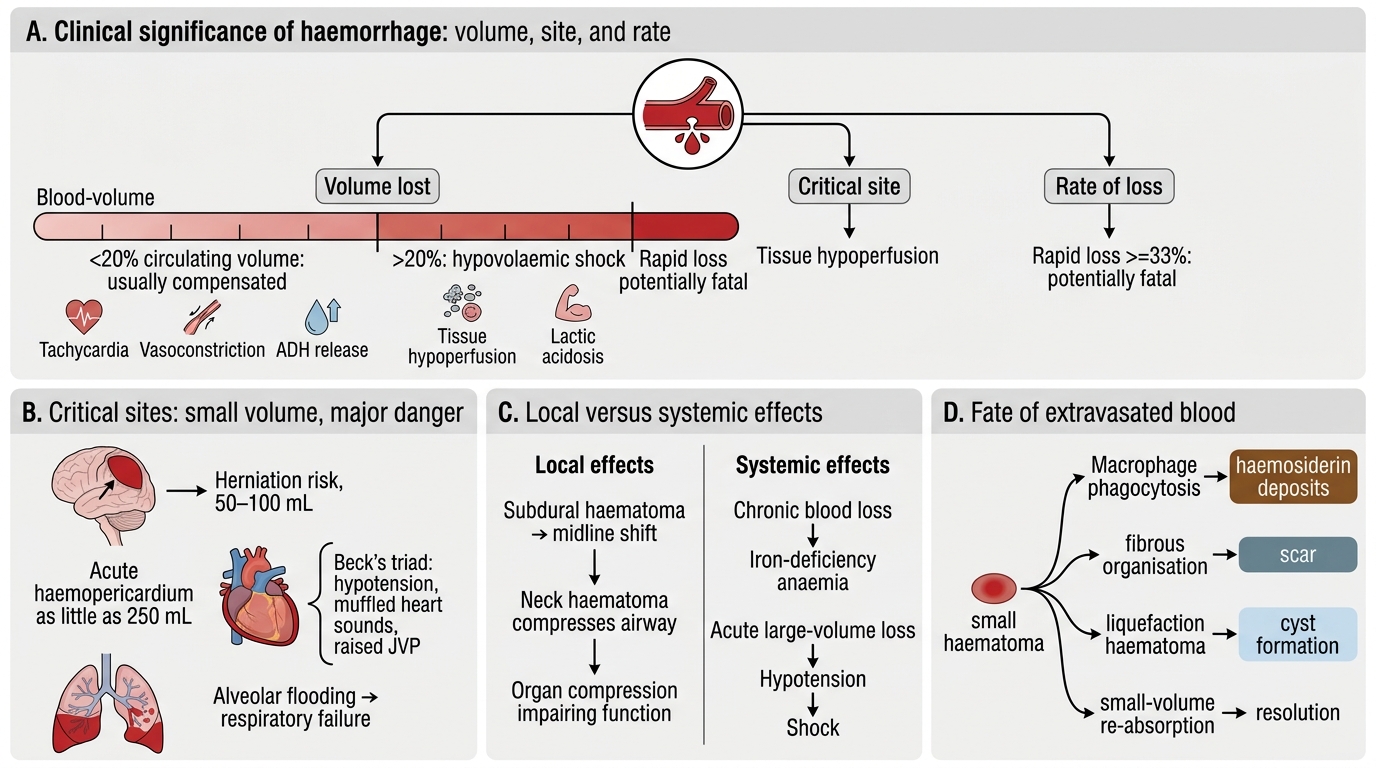
The clinical significance of haemorrhage depends on three independent variables:
Volume:
- Loss of < 20% circulating blood volume (< 1 L in adult) is generally well-tolerated by compensatory mechanisms (tachycardia, vasoconstriction, ADH release).
- > 20% → hypovolaemic shock — tissue hypoperfusion, lactic acidosis.
- Rapid loss of 33% or more can be fatal without resuscitation.
Site (even small volumes are dangerous in critical locations):
- Intracranial haematoma (50–100 mL) can be fatal by herniation.
- Haemopericardium (as little as 250 mL acute) → cardiac tamponade — Beck's triad (hypotension, muffled heart sounds, raised JVP).
- Pulmonary haemorrhage — alveolar flooding → respiratory failure.
Local vs systemic effects:
- Local: compression of adjacent structures (subdural haematoma → midline shift), obstruction of airway (neck haematoma), impaired organ function.
- Systemic: iron-deficiency anaemia (chronic blood loss); hypotension, shock (acute large-volume loss).
Outcome of extravasated blood:
- Phagocytosis by macrophages → haemosiderin deposits (permanent).
- Fibrous organisation → scar.
- Liquefaction (in haematomas) → cyst formation.
- Re-absorption (small volumes).
SELF-CHECK
A 28-year-old with severe thrombocytopaenia (platelets 8,000/µL) develops scattered 1–2 mm non-blanchable red spots over both lower legs. Which term CORRECTLY describes these lesions, and what is their mechanism?
A. Purpura — due to capillary rupture secondary to arterial hypertension
B. Ecchymoses — due to coagulation factor deficiency
C. Petechiae — due to red cell extravasation through capillary walls in the absence of adequate platelet plug formation
D. Haematoma — due to arterial bleeding into subcutaneous tissue
Reveal Answer
Answer: C. Petechiae — due to red cell extravasation through capillary walls in the absence of adequate platelet plug formation
Petechiae are pinpoint (1–2 mm) non-blanchable haemorrhages characteristically produced by thrombocytopaenia (or platelet dysfunction). When platelet count falls below ~20,000/µL, spontaneous capillary microhaemorrhages occur because primary haemostasis (platelet plug) cannot seal small vessel leaks. Purpura (A) refers to larger (> 3 mm) confluent haemorrhages and is not specific to hypertension. Ecchymoses (B) are large (> 1 cm) bruises and reflect deeper tissue haemorrhage. A haematoma (D) is a confined collection of blood — a different lesion class.
CLINICAL PEARL
Non-blanchable vs blanchable is the bedside test that separates haemorrhage from reactive hyperaemia: press a glass slide (diascopy) or a finger firmly on the lesion for 10 seconds. Haemorrhagic lesions (petechiae, purpura) do not blanch because blood is outside the vessel and cannot be displaced by pressure. Erythema from hyperaemia or capillary dilatation blanches and returns on release. This simple test changes the differential from trivial rash to potential platelet or vessel disorder.