Page 9 of 18
PA5.6 | Infarction & Thrombus Morphology — Practical — SDL Guide
Learning Objectives
- Distinguish pale (anaemic) from red (haemorrhagic) infarcts on gross examination, citing the organ and mechanism responsible for each type.
- Describe the systematic gross features of an infarct: shape, colour, consistency, and margin changes across early, established, and healed stages.
- Identify coagulative necrosis on H&E sections and list the cellular sequence from neutrophil infiltration through to fibrous scar formation.
- Recognise lines of Zahn in a thrombus and explain why their presence confirms antemortem formation.
- Differentiate an antemortem thrombus from a postmortem clot on gross inspection.
INSTRUCTIONS
Pathology practicals test pattern recognition under time pressure. The ability to look at a pot specimen or a glass slide and immediately articulate 'pale wedge-shaped infarct, renal cortex, arterial occlusion' separates a pass from a distinction. This module trains you to read infarcts and thrombi systematically — colour, shape, necrosis type, age, and antemortem vs postmortem — using the exact mental framework examiners expect.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 4 (Hemodynamic Disorders) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch. 4 (textbook)
- Underwood's General and Systematic Pathology, 6th ed., Ch. 6 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 60-year-old man with atrial fibrillation collapses at home. At autopsy, the left kidney shows a pale, wedge-shaped area with its apex pointing toward the hilum, and the heart shows a soft, yellow zone in the posterior left ventricular wall. A glass slide from the posterior wall shows ghost cells — nuclei gone, but cell outlines preserved.
Two different organs. Two infarcts. One word — ischaemic death — but the appearances are strikingly different. Your job today is to read these differences fluently, the way a radiologist reads a chest X-ray: systematically, then confidently.
WHY THIS MATTERS
PA5.6 appears on every MBBS Part II practical examination that involves a museum pot or a histology slide labelled 'infarct.' Examiners award marks for:
- Naming the type (pale vs haemorrhagic) with justification.
- Stating the organ and naming the occluded vessel.
- Estimating age from histological features.
- Distinguishing antemortem thrombus from postmortem clot.
Clinically, recognising infarct patterns on imaging is a direct extension of this morphological literacy — the wedge on CT correlates exactly with the wedge in the pot.
RECALL
Before you begin, check your Year-1 groundwork:
- Coagulative necrosis — the dominant necrosis type in most solid organs (exception: brain).
- Ischaemia — reduced arterial supply causing cell death downstream of an occlusion.
- Oedema vs congestion — passive venous engorgement produces haemorrhagic zones; arterial cut-off produces pale zones.
- Fibrin — the protein scaffold linking platelets in a thrombus, staining pink on H&E.
If any of these feel uncertain, spend 5 minutes with Robbins Ch. 2 before continuing.
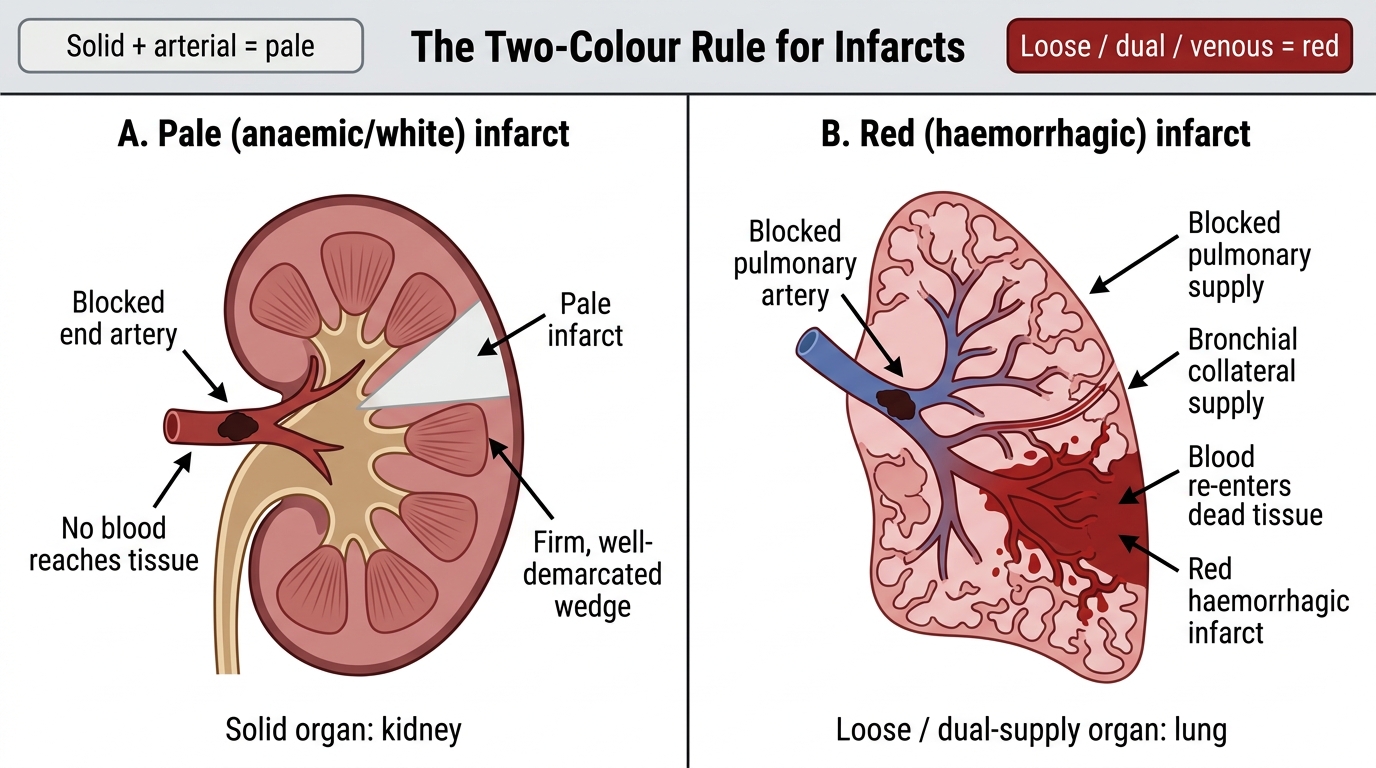
Classifying Infarcts: The Two-Colour Rule
Every infarct is classified first by colour because colour encodes the mechanism.
Pale (anaemic/white) infarct — occurs in solid organs with end-arterial supply and little collateral circulation: heart, kidney, spleen. When the artery is blocked, no blood reaches the tissue. The zone dies and turns pale grey-white. It is firm and well-demarcated.
Red (haemorrhagic) infarct — occurs when blood re-enters a dead zone after the occlusion, filling the necrotic tissue. This happens in three settings:
• Organs with dual blood supply (lung has pulmonary artery + bronchial artery).
• Organs with venous occlusion (intestine — the artery keeps pushing blood in, the vein cannot drain it).
• Loose, spongy tissue (lung parenchyma) that accommodates seeping blood.
Memory rule: Solid + arterial = pale. Loose/dual/venous = red.
Pale vs Red Infarcts: The Two-Colour Rule
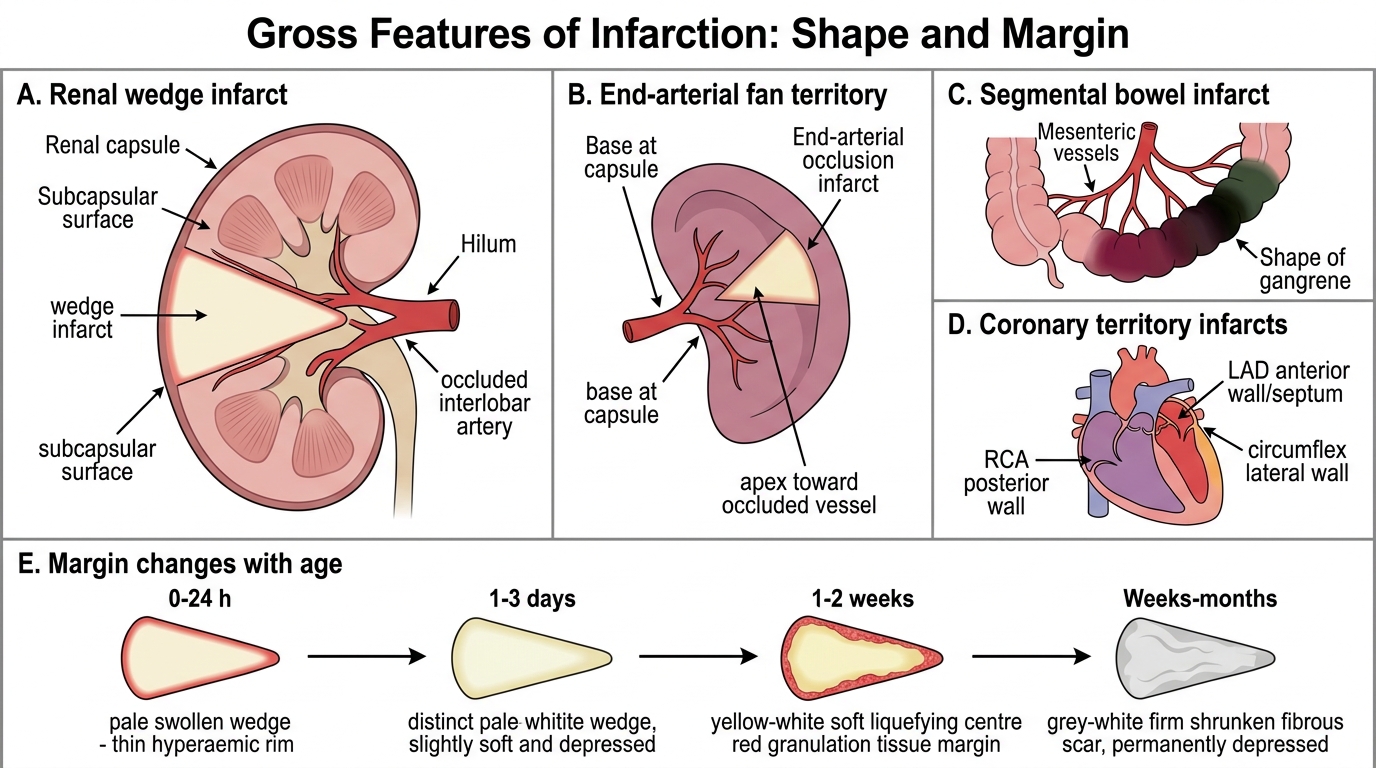
Gross Features: Reading the Shape and Margin
Shape is the second key read after colour.
Wedge-shaped infarct — the hallmark of end-arterial occlusion in a fan-distributed organ (kidney, spleen). The base faces the capsule (subcapsular), the apex points toward the hilum (toward the occluded vessel). Think of a pie slice with the narrow end at the blocked vessel.
In the intestine, infarcts are segmental — a loop of bowel goes dark red-purple, then black-green as gangrene supervenes. The shape follows the mesenteric vessel territory.
In the heart, the distribution follows coronary artery territories — posterior wall infarcts (right coronary), lateral wall (circumflex), anterior wall/septum (LAD).
Margin changes with age:
• Early (0–24 hours): barely visible; the zone is slightly pale and swollen with a hyperaemic rim (reactive red border from surrounding viable tissue).
• 1–3 days: pale/yellow-white centre becomes distinct; soft, may be slightly depressed.
• 1–2 weeks: yellow, soft, liquefying in centre; granulation tissue visible at margin.
• Weeks to months: replaced by a fibrous scar — grey-white, firm, shrunken, permanently depressed.
Gross Shape and Margin of Infarcts
SELF-CHECK
A pot specimen shows the left kidney with a grey-white, wedge-shaped lesion, base facing the cortical surface, apex pointing toward the renal pelvis. The most likely cause is:
A. Renal vein thrombosis
B. Embolism to an interlobar artery
C. Acute tubular necrosis from hypotension
D. Renal abscess formation
Reveal Answer
Answer: B. Embolism to an interlobar artery
A pale wedge infarct with apex toward the hilum indicates end-arterial occlusion — classically an embolus lodging in an interlobar or arcuate artery. Renal vein thrombosis would produce a red (haemorrhagic) infarct because venous congestion allows blood to re-enter the tissue. Acute tubular necrosis is diffuse, not wedge-shaped. An abscess is creamy/suppurative, not pale and wedge-shaped.
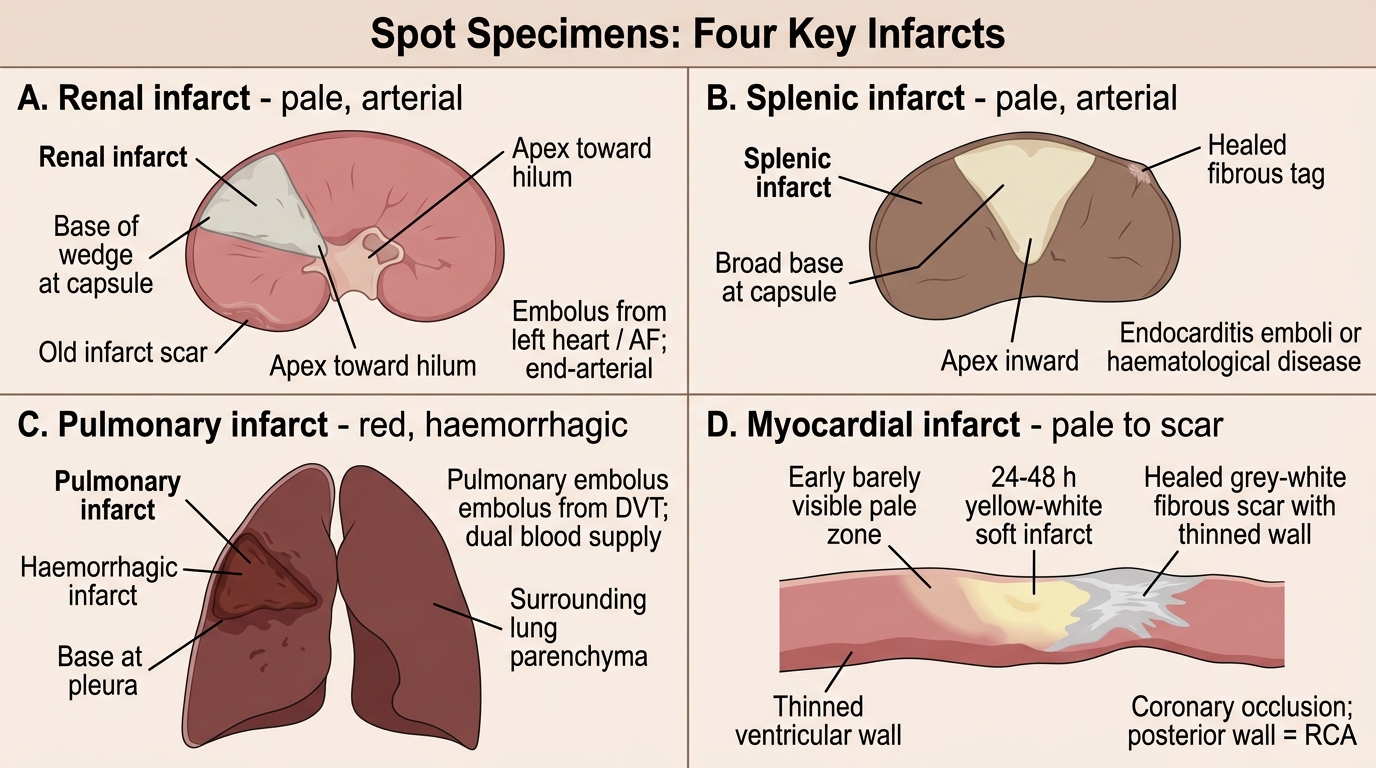
Spot Specimens: Four Key Examples
Learn these four — they cover the entire spectrum the examiner can ask:
1. Renal infarct (pale wedge)
Organ: kidney. Cut surface: pale, firm, grey-white wedge. Base at capsule (may be depressed/scarred if old). Apex at hilum. Cause: embolism (commonest — left heart thrombus, AF). Type: pale (end-arterial).
2. Splenic infarct (pale wedge)
Organ: spleen. Similar pale wedge, base at capsule. Often incidental in haematological disease (leukaemia, myelofibrosis) or endocarditis emboli. Healed = capsular fibrous tag.
3. Pulmonary infarct (red/haemorrhagic)
Organ: lung. Haemorrhagic, wedge-shaped (wedge base at pleura). Dark red-brown, firm, raised above surrounding parenchyma (congested). Cause: pulmonary embolism (DVT). Type: red (dual supply — bronchial artery re-fills the dead zone).
4. Myocardial infarct (pale, then yellow)
Organ: heart. Early: barely visible. 24–48 h: yellow-white, soft zone. Healed: grey-white fibrous scar, thinned wall. Location encodes artery: posterior wall = RCA. Type: pale (end-arterial; no collaterals in normal heart).
Four Classic Gross Specimens of Infarction