Page 10 of 18
PA5.6 | Infarction & Thrombus Morphology — Practical — SDL Guide (Part 2)
Composite Specimen Panel — H5P Image Hotspots Activity
Study the four panels below before answering the hotspot questions embedded in the H5P activity. Each panel isolates one key morphological feature you must be able to name and explain.
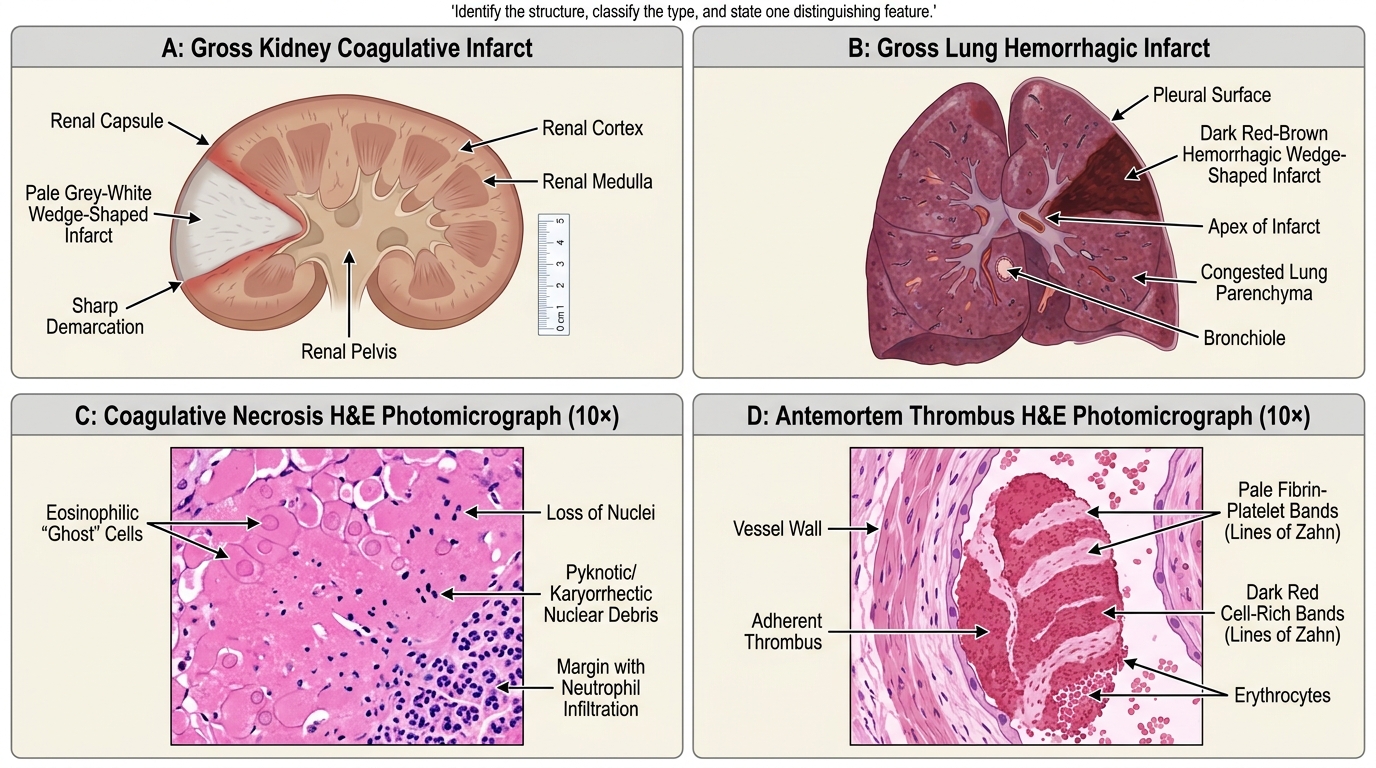
Morphology of Infarction and Thrombosis
For each panel, the H5P hotspots will ask you to identify the structure, classify the type, and state one distinguishing feature. Attempt the activity before reading the micro section.
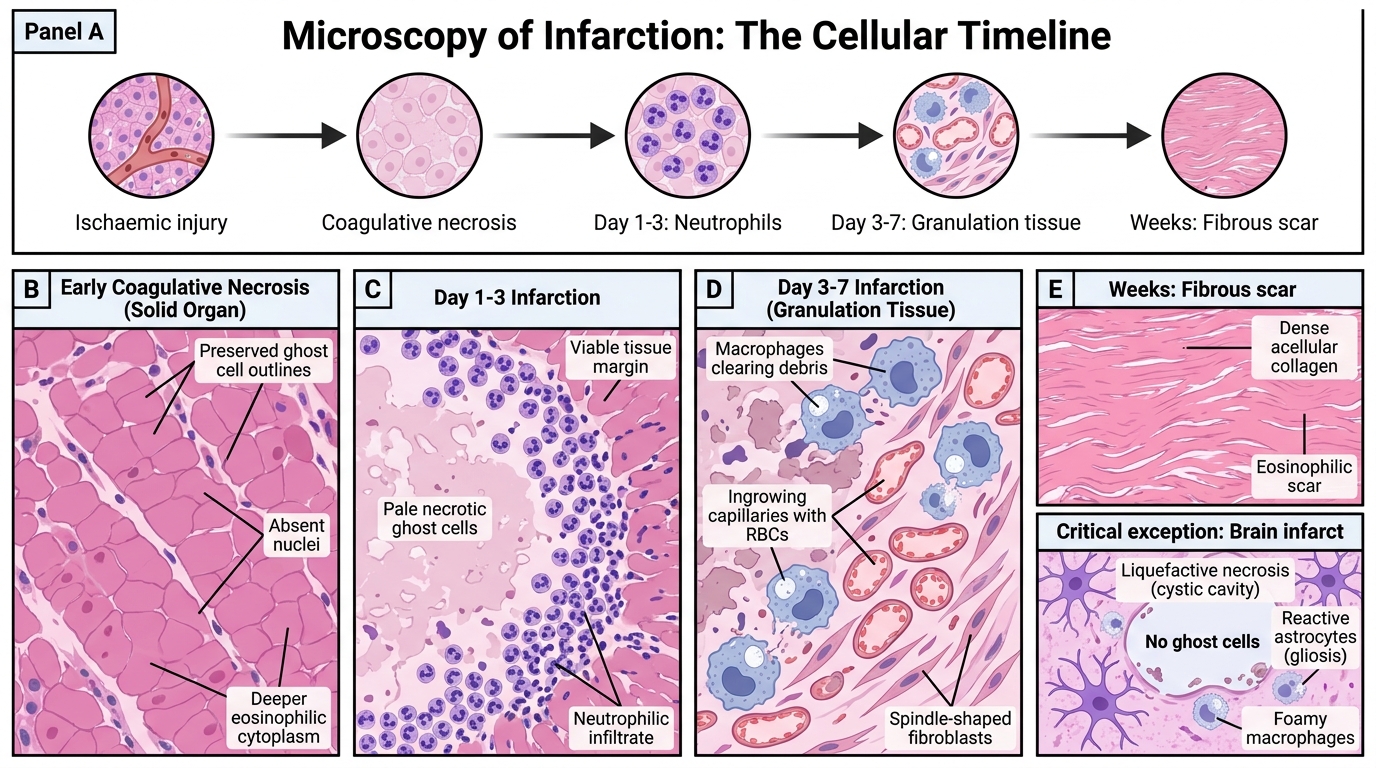
Microscopy of Infarction: The Cellular Timeline
The histological changes in an infarct follow a predictable sequence. Learn to age an infarct on a slide.
Coagulative necrosis (the dominant pattern)
• Nuclei disappear (karyolysis, karyorrhexis, pyknosis — all terms mean dead nucleus).
• Cell outlines (ghost cells) are preserved for days because the structural protein framework denatures but does not dissolve immediately.
• Cytoplasm becomes more eosinophilic (deeper pink) on H&E.
• This is the histological hallmark of ischaemic cell death in heart, kidney, spleen.
Day 1–3: Neutrophil infiltration
• Acute inflammation begins at the viable margin.
• Neutrophils flood the necrotic zone, attempting to clear debris.
• On the slide: a rim of pale necrotic ghost cells surrounded by dark-staining neutrophils.
Day 3–7: Granulation tissue ingrowth
• Macrophages replace neutrophils (debris clearance).
• New capillaries and fibroblasts begin to grow in from the margin.
• The slide shows vascular channels and spindle cells replacing necrosis.
Weeks: Fibrous scar
• Collagen replaces the granulation tissue.
• Mature scar: dense, acellular, eosinophilic collagen replacing the original architecture.
Critical exception — Brain infarct → Liquefactive necrosis
The brain's high lipid content and lack of structural protein scaffold means brain infarcts liquefy. Ghost cells are NOT seen. Instead: fluid-filled cavity (cystic softening) surrounded by reactive astrocytes (gliosis). Never apply 'coagulative' to brain.
Microscopy of Infarction: Cellular Timeline
SELF-CHECK
On an H&E slide of a renal infarct, you see pale pink areas where tubular outlines are intact but all nuclei are absent. The correct descriptive term for this necrosis pattern is:
A. Liquefactive necrosis
B. Caseous necrosis
C. Coagulative necrosis
D. Fat necrosis
Reveal Answer
Answer: C. Coagulative necrosis
Preserved cell outlines with complete nuclear loss is the defining feature of coagulative necrosis — the type seen in ischaemic infarcts of solid organs (heart, kidney, spleen). Liquefactive necrosis (brain, abscess) shows dissolution of outlines. Caseous necrosis (TB) shows amorphous pink granular debris with no architecture. Fat necrosis shows saponification with calcium deposits in adipose tissue.
CLINICAL PEARL
The brain exception is the examiner's favourite trap. Every time the examiner says 'infarct,' the expected answer for most organs is coagulative necrosis. But if the specimen or stem mentions brain, the answer is liquefactive necrosis — and the reason (lipid-rich tissue, no structural protein scaffold, liquefies to a cyst) must accompany the answer. Forgetting this costs marks in both theory and practical viva.
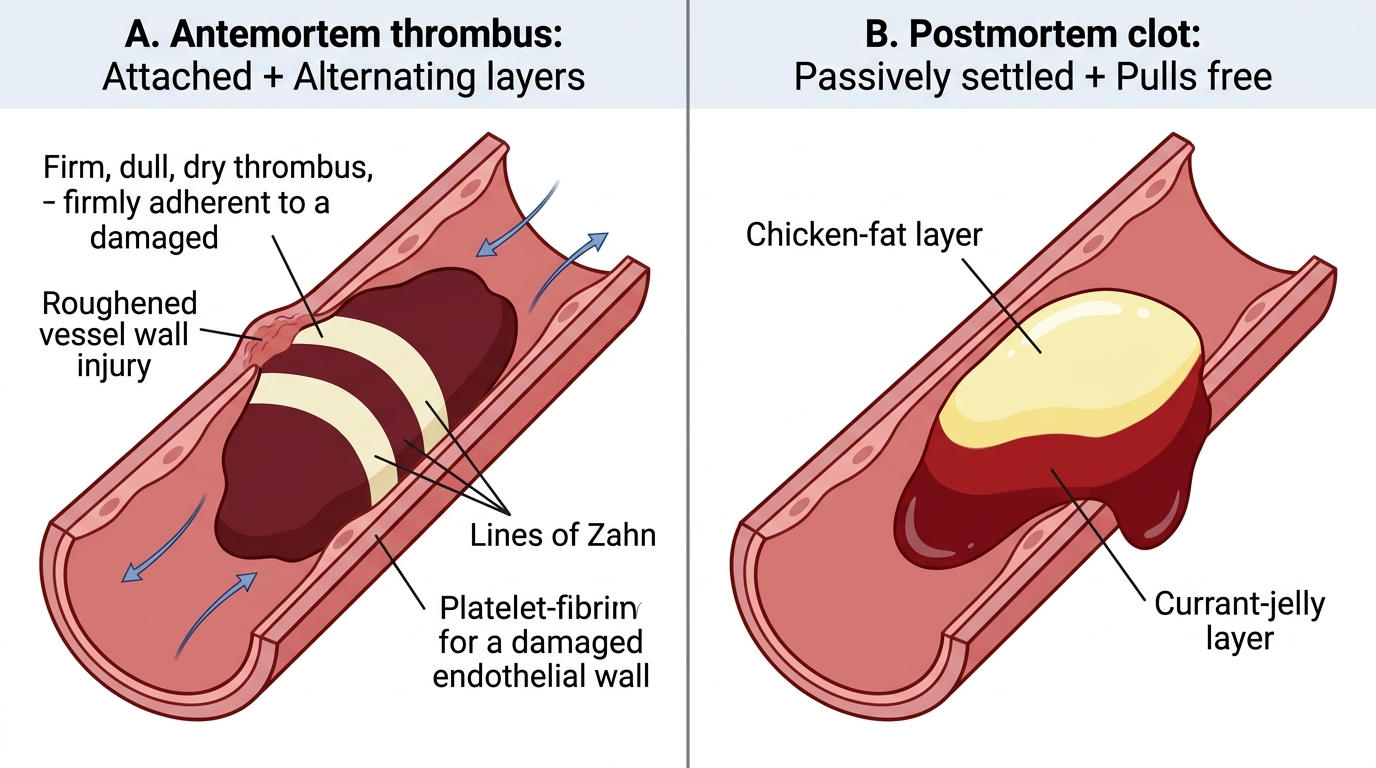
Thrombus Morphology: Antemortem vs Postmortem
Distinguishing an antemortem (formed during life) thrombus from a postmortem clot is a classic practical and viva question.
Antemortem thrombus — key features:
• Lines of Zahn — alternating pale layers (platelet + fibrin aggregates) and dark red layers (red blood cells trapped between). These form because the thrombus builds up in layers as blood flows past a turbulent or damaged site.
• Attached to the vessel wall — the thrombus adheres at the point of endothelial injury or turbulent flow. It is firm and dry.
• Dull, friable surface (not glistening).
• May show organisation (granulation tissue growing in = organised thrombus).
Postmortem clot — key features:
• Formed after cardiac arrest when blood stagnates and clots passively.
• No lines of Zahn — the clot is homogeneous.
• Chicken-fat clot — yellow-white upper layer (plasma + leukocytes, as red cells settle by gravity before clotting).
• Currant-jelly layer — dark red lower layer (settled red cells + fibrin).
• Not attached to vessel wall — easily slips out at autopsy.
• Shiny, gelatinous, elastic.
Memory rule: Antemortem = Attached + Alternating layers. Postmortem = Passively settled + Pulls free.
Antemortem Thrombus vs Postmortem Clot
SELF-CHECK
At autopsy, the pathologist finds a dark red gelatinous material in the femoral vein that slips out easily, has a yellow-white upper layer and a dark red lower layer, and shows no attachment to the wall. The correct interpretation is:
A. Antemortem deep vein thrombosis with lines of Zahn
B. Postmortem clot — the currant-jelly and chicken-fat layers indicate passive settling after death
C. Organised thrombus with early recanalisation
D. Septic thrombus from bacteraemia
Reveal Answer
Answer: B. Postmortem clot — the currant-jelly and chicken-fat layers indicate passive settling after death
Non-attachment to the wall, shiny gelatinous texture, and the characteristic bi-layered appearance (yellow-white chicken-fat over dark red currant-jelly) are the hallmarks of a postmortem clot. Lines of Zahn (alternating pale and dark layers in a firmly attached, dull thrombus) confirm antemortem formation. An organised thrombus shows ingrowth of fibroblasts and capillaries. A septic thrombus is attached and may contain microabscesses.