Page 11 of 18
PA5.6 | Infarction & Thrombus Morphology — Practical — SDL Guide (Part 3)
The Reading Framework: Approach Any Specimen in 4 Steps
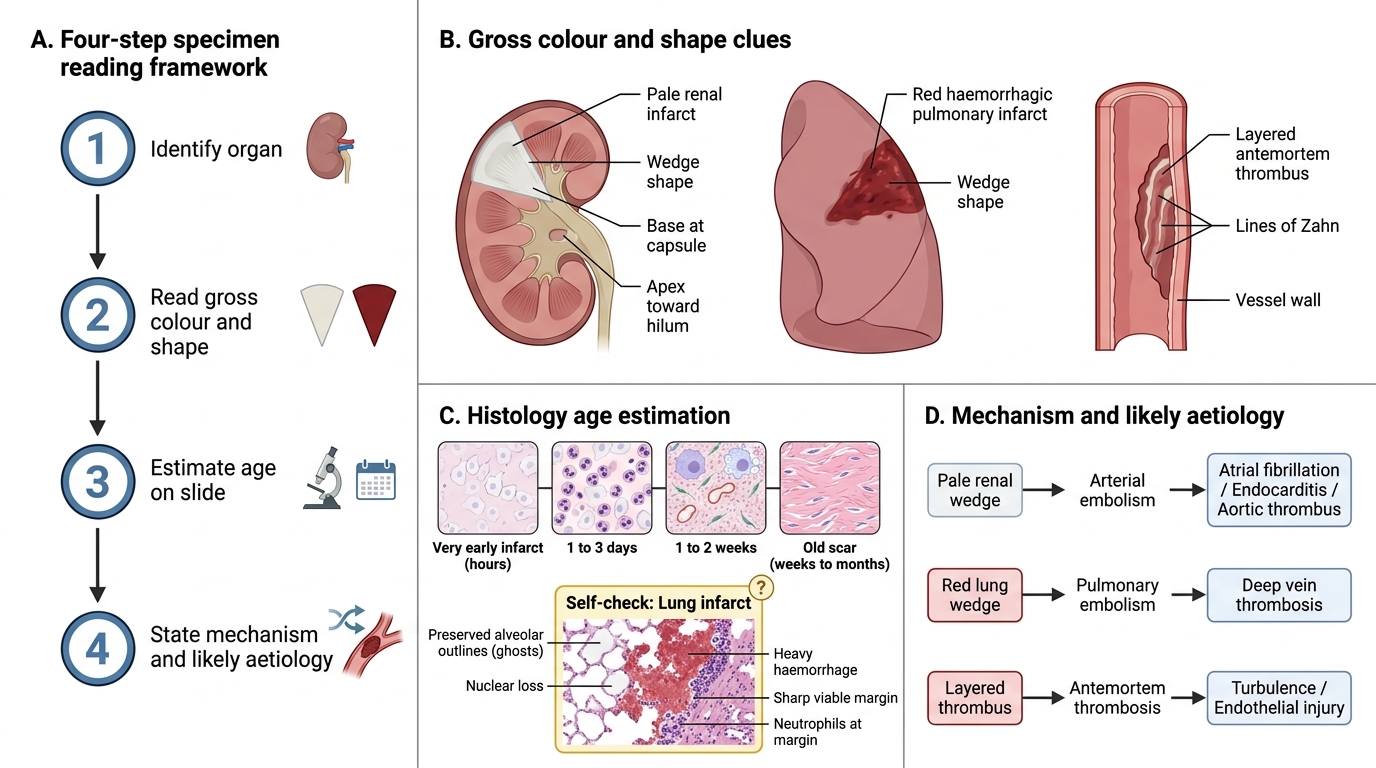
Four-Step Framework for Reading Hemodynamic Disorder Specimens
Use this systematic approach in the practical examination — it earns marks even if you miss a detail, because it shows you know how to read a specimen.
Step 1 — Identify the organ.
Name it. State one distinguishing feature (e.g., 'kidney — corticomedullary architecture visible on cut section').
Step 2 — Gross colour and shape of the lesion.
• Pale/grey-white → likely pale infarct (arterial, solid organ).
• Dark red/haemorrhagic → likely red infarct (dual supply, venous, loose tissue) or thrombus/clot.
• Wedge-shaped with base at capsule, apex at hilum → end-arterial infarct.
• Segmental loop → intestinal infarct.
Step 3 — Estimate the age (if a slide).
• Ghost cells only → very early (< 24 h).
• Ghost cells + neutrophils → 1–3 days.
• Macrophages + granulation tissue → 1–2 weeks.
• Dense collagen, no cells → old scar.
Step 4 — State the mechanism and likely aetiology.
• Pale wedge in kidney → arterial embolism → source? (AF, endocarditis, aortic thrombus).
• Red wedge in lung → pulmonary embolism → source? (DVT).
• Attached layered thrombus → antemortem formation → turbulence or endothelial injury.
Practise this sequence on every pot specimen until it is automatic.
SELF-CHECK
A histology slide shows a region of lung with preserved alveolar outlines but complete nuclear loss, heavy haemorrhage filling the alveolar spaces, and a sharp margin with viable lung on the right. Neutrophil infiltration is present at the viable margin. How old is this infarct, and what type is it?
A. Old scar (weeks old); pale infarct
B. 1–3 days old; red (haemorrhagic) infarct
C. Less than 6 hours old; pale infarct
D. 2 weeks old; organised thrombus
Reveal Answer
Answer: B. 1–3 days old; red (haemorrhagic) infarct
Preserved alveolar outlines with nuclear loss = coagulative necrosis (confirming infarct, not abscess). Heavy intra-alveolar haemorrhage = haemorrhagic (red) infarct — consistent with lung's dual supply. Neutrophil infiltration at the margin dates the lesion to 1–3 days after the event. An old scar would show dense collagen and no nuclei in any layer. Less than 6 hours would show very minimal or no inflammatory response.
SELF-CHECK
In a thrombus removed from a deep femoral vein at post-mortem, H&E shows alternating pale eosinophilic layers (fibrin + platelets) and darker erythrocyte-rich layers. The most important conclusion from this finding is:
A. The thrombus formed after death — postmortem passive clotting creates these layers
B. The thrombus is septic — bacteria trapped between layers
C. The thrombus formed during life — lines of Zahn confirm antemortem origin
D. The thrombus is fully organised — granulation tissue in layers
Reveal Answer
Answer: C. The thrombus formed during life — lines of Zahn confirm antemortem origin
Lines of Zahn — the alternating pale (platelet-fibrin) and dark (red cell) layers — form ONLY when flowing blood progressively deposits material at a site of turbulence or endothelial damage during life. This is the single most important microscopic criterion for antemortem thrombus formation. Postmortem clots are homogeneous on H&E (no alternating layers). Organisation means fibroblast/capillary ingrowth, not layering.