Page 5 of 18
PA5.3-5 | Thrombosis, Embolism, Infarction & Shock — SDL Guide
Learning Objectives
- Recall the steps of normal haemostasis and link them to mechanisms of thrombosis (PA5.4)
- Apply Virchow's triad to explain why arterial and venous thrombi form in different clinical contexts
- Distinguish the morphology and fate of thrombi, including lines of Zahn
- Classify types of embolism, recognise their sources, and predict clinical consequences (PA5.5)
- Differentiate red (haemorrhagic) from white (anaemic) infarction and identify the governing factors
- Define shock, classify its types, and trace the stages from compensated to irreversible, with emphasis on septic shock pathogenesis (PA5.3)
INSTRUCTIONS
Circulatory failure — thrombosis, embolism, infarction, and shock — accounts for the majority of in-hospital deaths worldwide. Mastering these four interconnected processes gives you a mechanistic framework that explains sudden chest pain, post-operative DVT, multi-organ failure, and the cascade behind sepsis. This module builds directly on Year-1 physiology of coagulation (cross-reference Hematology H10 for clotting factor details) and anchors the clinico-pathological correlations you will encounter in clinical postings.
References
- Robbins & Kumar: Basic Pathology, 10th ed., Ch 3 (Hemodynamic Disorders) (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 4 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old woman, 3 days post-hip replacement, develops sudden breathlessness and pleuritic chest pain. Her oxygen saturation drops to 88%. The resident suspects a pulmonary embolus — but where did the clot come from, how did it travel, and why did it pick this moment? By the end of this module, you will be able to answer all three questions — and extend that reasoning to shock, infarction, and a dozen other embolic disasters.
WHY THIS MATTERS
Thromboembolism is the leading preventable cause of hospital death. Shock kills one in four patients who reach the ICU. Understanding the pathological sequence — haemostasis → thrombosis → embolism → infarction → shock — is not background knowledge; it is the diagnostic and therapeutic framework you will apply every day in medicine, surgery, and obstetrics.
RECALL
Before reading further, rehearse what you already know:
- What are the three phases of normal haemostasis? (Cross-reference Hematology H10 for detail — we summarise only.)
- Name three anticoagulant mechanisms that normally prevent spontaneous clotting.
- What is the difference between a platelet plug and a fibrin clot?
Normal haemostasis in brief: (1) Vascular spasm (immediate, transient); (2) Primary haemostasis — platelet adhesion via vWF → activation → aggregation forming the platelet plug; (3) Secondary haemostasis — coagulation cascade (intrinsic + extrinsic) → thrombin → fibrin mesh stabilises the plug. Endothelial counter-regulators (prostacyclin, NO, thrombomodulin, TFPI, tPA) confine clotting to the injury site. When these fail or are overwhelmed, pathological thrombosis begins.
Thrombosis: Virchow's Triad
Thrombosis is the pathological formation of a solid mass (thrombus) from blood constituents within the vascular system in a living subject. Rudolf Virchow described three predisposing factors — Virchow's triad — that remain the cornerstone of thrombosis teaching:
- Endothelial injury — the dominant factor for arterial thrombosis. Damaged endothelium exposes subendothelial collagen and tissue factor, activating both platelets and the coagulation cascade. Causes: atherosclerotic plaque disruption, hypertension, smoking, hypercholesterolaemia, mechanical trauma.
- Abnormal blood flow — turbulence (at arterial bifurcations, stenoses) disrupts laminar flow, activating endothelium and bringing platelets into wall contact. Stasis (slow venous flow, immobility, cardiac failure) prevents dilution of activated clotting factors and inhibits fresh inhibitor delivery. Stasis is the dominant factor in deep vein thrombosis (DVT).
- Hypercoagulability — primary (hereditary: Factor V Leiden, Protein C/S deficiency, antithrombin deficiency) or secondary (acquired: oral contraceptives, pregnancy, malignancy, prolonged immobility, antiphospholipid syndrome).
Clinical examples:
• Coronary artery thrombus: endothelial injury (plaque rupture) is primary.
• Post-operative DVT: stasis + hypercoagulability (surgical trauma, immobility).
• Atrial fibrillation → mural thrombus: stasis in non-contractile atrium.
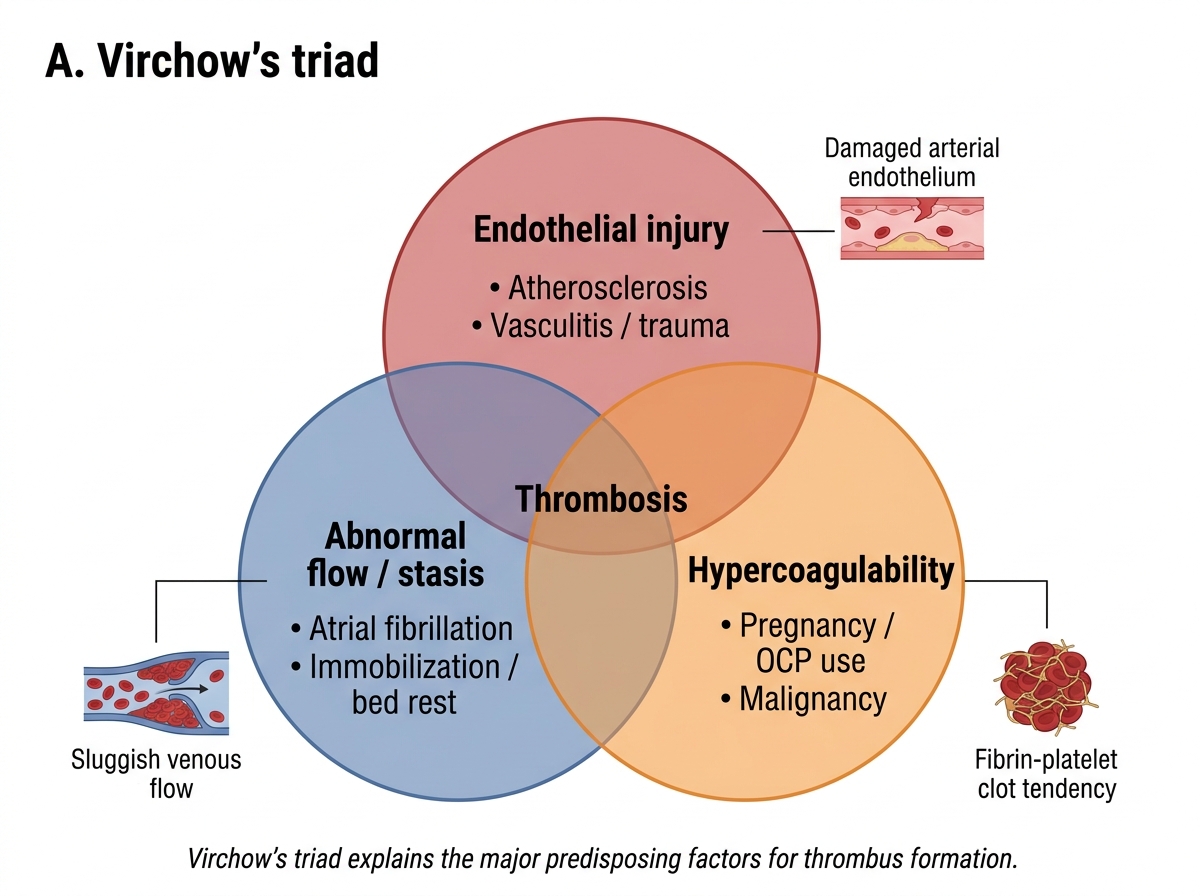
Virchow's Triad in Thrombosis
Arterial vs Venous Thrombi & Lines of Zahn
Arterial thrombi form at sites of endothelial injury and turbulence (coronary, cerebral, femoral arteries). They are platelet-rich and pale/white (platelets + fibrin, few red cells), grow retrogradely against flow, and are occlusive — causing downstream ischaemia/infarction.
Venous thrombi (phlebothrombosis) form under stasis, predominantly in the deep veins of the lower limb (calf → popliteal → femoral → iliac → inferior vena cava). They are red thrombi — large, dark red-blue, gelatinous; rich in red cells trapped in fibrin with few platelets. They grow antegrade (in the direction of flow) and may extend silently before causing symptoms.
Lines of Zahn are a key morphological feature of ante-mortem arterial thrombi: pale laminae of platelets and fibrin alternating with darker red cell-rich layers, produced by undulating pulsatile flow. Their presence confirms the thrombus formed in a living vessel with flowing blood. They are ABSENT in post-mortem clots — which are uniform and gelatinous ('chicken-fat' clot + 'currant-jelly' clot).
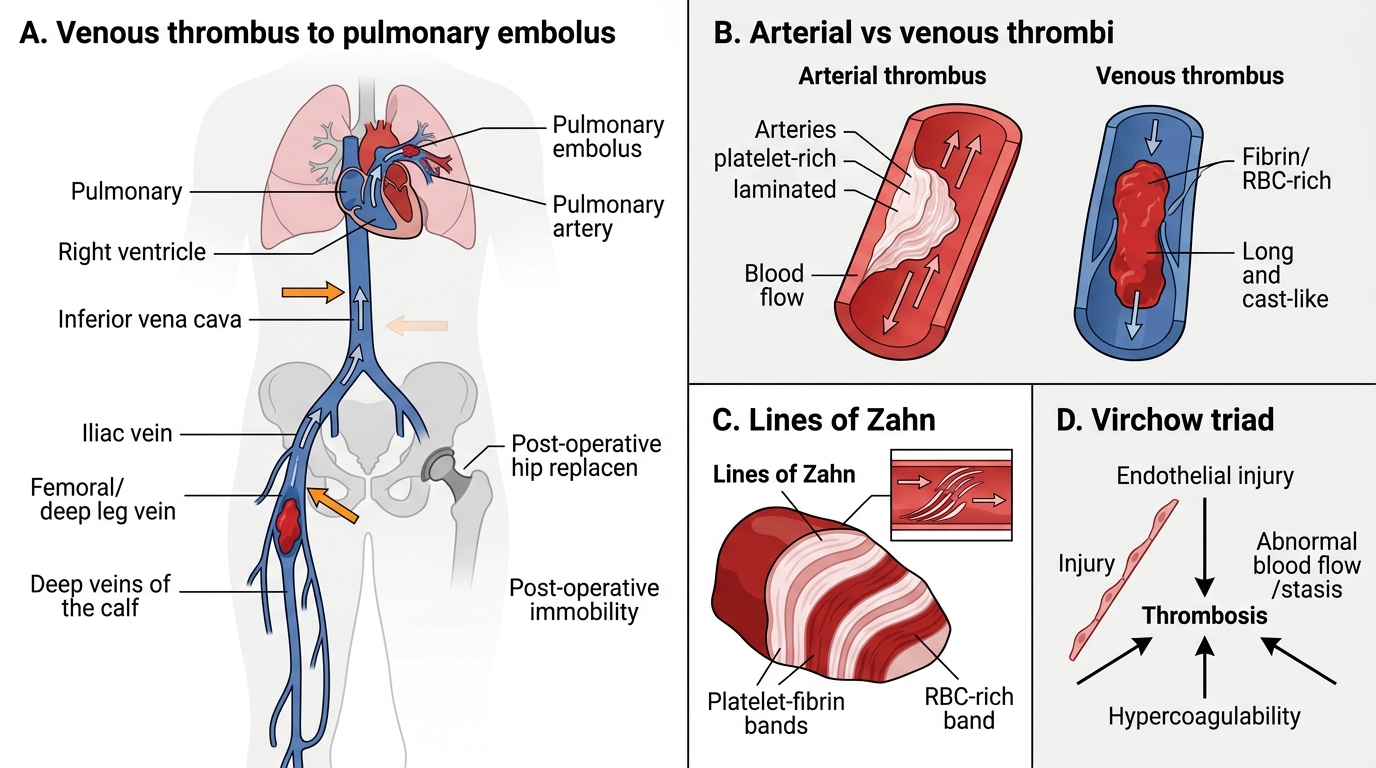
Arterial vs Venous Thrombi and Lines of Zahn
SELF-CHECK
A post-operative patient develops a calf DVT. Which component of Virchow's triad is MOST dominant in this scenario?
A. Stasis due to immobility and venous pooling
B. Endothelial injury from surgical trauma
C. Turbulence at venous valve cusps
D. Primary hypercoagulability (Factor V Leiden)
Reveal Answer
Answer: A. Stasis due to immobility and venous pooling
While surgical trauma does cause some endothelial injury, the dominant mechanism in post-operative DVT is stasis — immobility slows venous return, allows activated clotting factors to accumulate, and prevents inhibitor delivery. This is why early mobilisation and LMWH prophylaxis are standard post-operative practice.
Fate of Thrombi
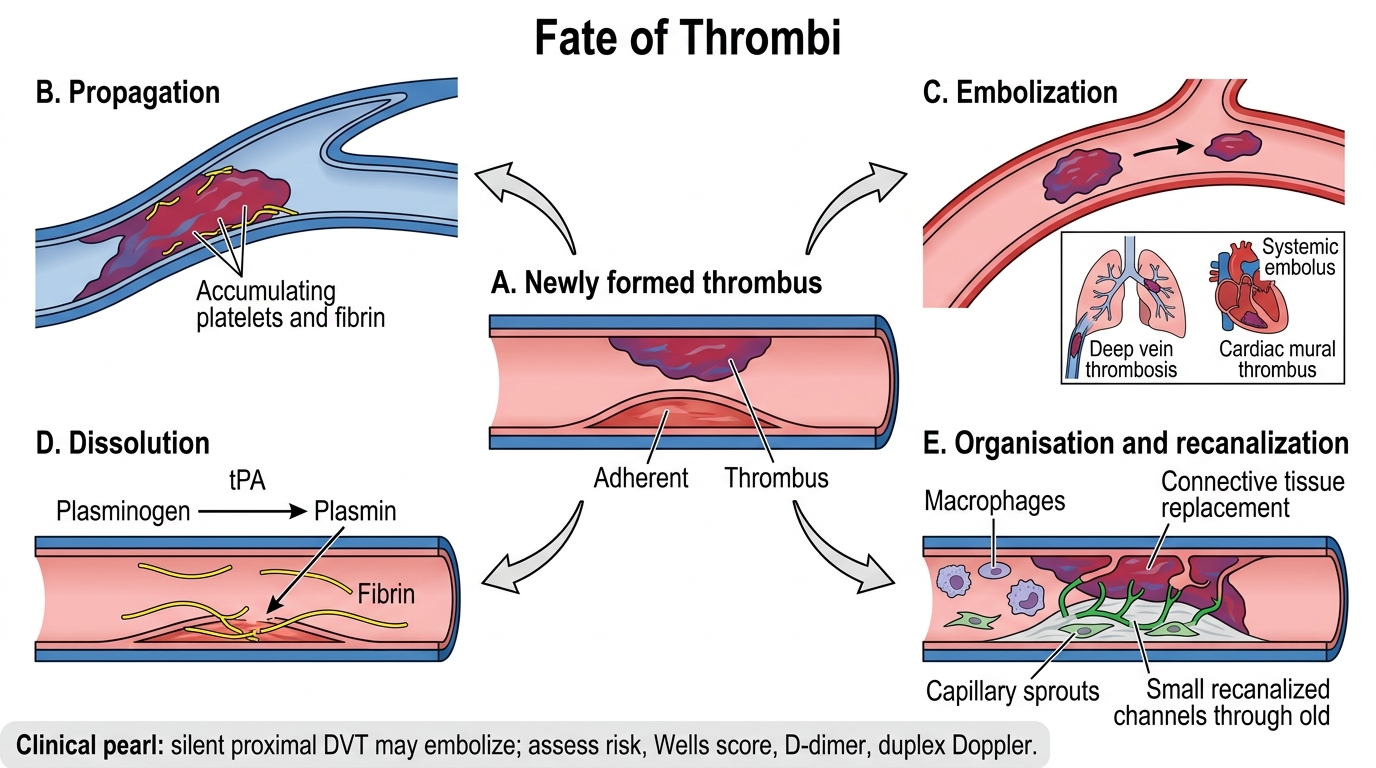
Once formed, a thrombus has four possible fates:
- Propagation — the thrombus extends along the vessel, accumulating more platelets and fibrin. A calf DVT may propagate proximally to the iliac vein, dramatically increasing embolism risk.
- Embolization — the thrombus (or a fragment) detaches and travels in the bloodstream. This is the most dangerous fate: pulmonary embolism from DVT, systemic emboli from cardiac mural thrombi.
- Dissolution — fibrinolysis (tPA, plasmin) lyses the thrombus completely, especially if small and recent. This is the basis of thrombolytic therapy (streptokinase, alteplase).
- Organisation and recanalization — over days to weeks, fibrovascular granulation tissue (macrophages, fibroblasts, capillary sprouts) grows into the thrombus from the vessel wall, converting it to connective tissue (organisation). New capillary channels may coalesce to form luminal passages (recanalization), partially restoring flow. Calcified old thrombi in veins are called phleboliths.
Fate of Thrombi
CLINICAL PEARL
The 'silent DVT' trap: Up to 50% of proximal DVTs are asymptomatic until embolization. Never wait for the classic swollen, tender calf before acting on clinical risk factors. In a post-operative or bed-bound patient with unexplained tachycardia or low-grade fever, think DVT → PE first. The Wells score + D-dimer + duplex Doppler is the standard triage triad. D-dimer has high negative predictive value — a normal result in a low-probability patient effectively rules out DVT.