Page 6 of 18
PA5.3-5 | Thrombosis, Embolism, Infarction & Shock — SDL Guide (Part 2)
Embolism: Types, Sources & Consequences
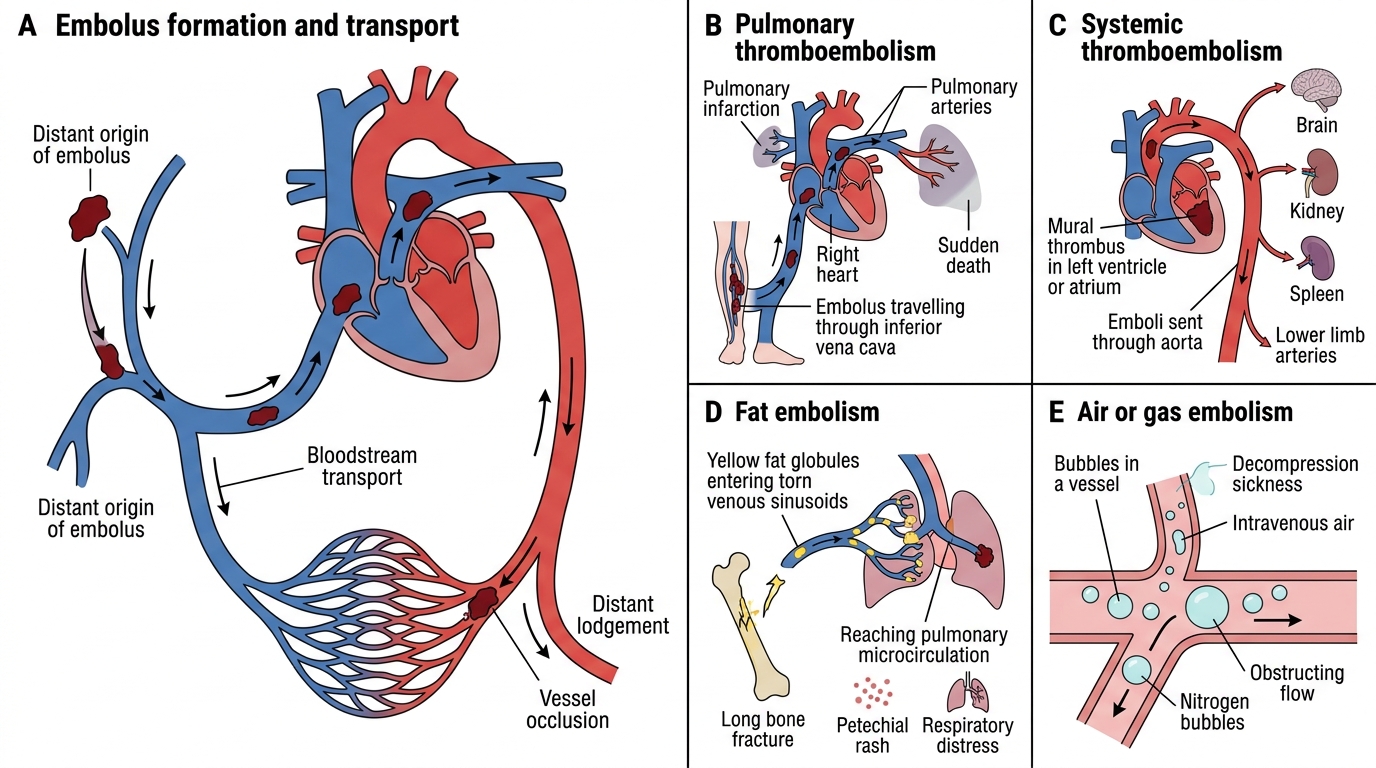
Embolism is the lodgement of an abnormal mass (embolus) within the vascular system at a site distant from its origin, carried there by the bloodstream. An embolus may be solid, liquid, or gaseous.
| Type | Source | Destination | Key clinical scenario |
|---|---|---|---|
| Thromboembolism (most common) | DVT of lower limb | Pulmonary arteries | Post-op PE, sudden dyspnoea |
| Systemic arterial | Mural thrombus (MI, AF, dilated CMP) | Brain, spleen, kidney, limbs | Stroke, splenic/renal infarct |
| Fat embolism | Long-bone fracture (femur, tibia) — marrow fat | Pulmonary + cerebral capillaries | Hypoxia + petechiae + confusion 24-72 hr post-fracture |
| Air embolism | IV line, chest trauma, neck surgery | Right heart / pulmonary | Churning 'mill-wheel' murmur; >100 mL fatal |
| Amniotic fluid embolism | Amniotic fluid enters maternal veins at delivery | Pulmonary vessels | Acute dyspnoea, DIC, cardiovascular collapse; rare but highly fatal |
| Atherosclerotic (cholesterol crystal) | Ruptured plaque | Distal arterioles | Blue toe syndrome, livedo reticularis |
| Tumour embolism | Tumour cells invading vessels | Pulmonary, systemic | Haematogenous metastasis mechanism |
| Septic embolism | Infected thrombus (endocarditis, septic thrombophlebitis) | Distal organs | Pulmonary abscesses from right-sided endocarditis |
Pulmonary thromboembolism (PTE): 95% arise from DVT of lower limb veins. A saddle embolus straddles the bifurcation of the main pulmonary artery → sudden death from acute cor pulmonale. Smaller emboli → pulmonary infarction (haemorrhagic, wedge-shaped, pleural surface). Smaller still → transient dyspnoea without infarction. Repeated small emboli → pulmonary hypertension.
Embolism: Types, Sources and Consequences
SELF-CHECK
A 24-year-old male sustains a closed femoral shaft fracture. 36 hours later he develops confusion, petechiae on the chest wall, and oxygen saturation of 85%. The MOST likely diagnosis is:
A. Pulmonary thromboembolism from DVT
B. Fat embolism syndrome
C. Air embolism from IV line insertion
D. Septic embolism from wound infection
Reveal Answer
Answer: B. Fat embolism syndrome
The triad of hypoxia + neurological features + petechiae appearing 24-72 hours after long-bone (especially femoral) fracture is classic fat embolism syndrome. Bone marrow fat globules enter torn venous sinusoids, travel to pulmonary and cerebral capillaries, and cause mechanical obstruction plus toxic fatty acid release. Petechiae result from fat globules in dermal capillaries — a pathognomonic finding not seen in PE.
Infarction: Red vs White
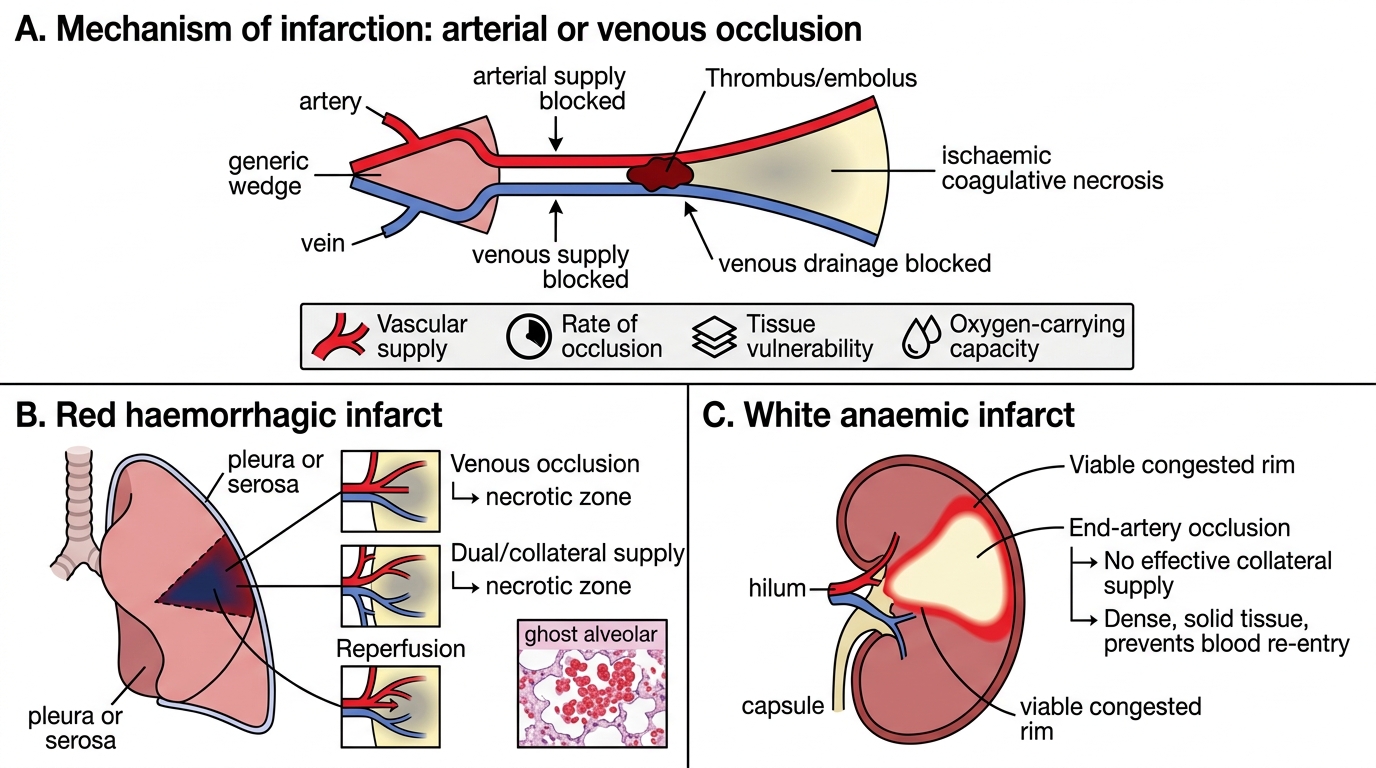
Infarction is an area of ischaemic coagulative necrosis caused by occlusion of arterial supply or venous drainage. Most infarcts result from thrombosis or embolism.
Red (haemorrhagic) infarcts occur when blood re-enters the necrotic zone:
• Venous occlusion (ovarian, mesenteric vein thrombosis) — arterial blood flows in but cannot drain.
• Loose (spongy) tissue architecture — lung has dual blood supply (bronchial + pulmonary); blood floods the necrotic area.
• Reperfusion after restoration of arterial supply.
• Examples: lung, small intestine, ovary, testis.
• Morphology: red-blue, haemorrhagic, wedge-shaped (base on pleura/serosa), coagulative necrosis with ghost alveolar outlines on histology.
White (anaemic) infarcts occur in solid organs with end-arterial supply:
• Single arterial supply with no effective collaterals; dense tissue resists blood re-entry into the necrotic zone.
• Examples: spleen, kidney, heart (myocardial infarction), brain (pale infarct in some zones).
• Morphology: pale yellow-white, wedge-shaped (apex toward hilum), firm; surrounded by a hyperaemic rim of viable congested tissue.
Factors influencing infarct development:
1. Nature of vascular supply (end-artery vs dual/collateral) — most important.
2. Rate of occlusion — gradual → collaterals develop; sudden → no compensation.
3. Tissue vulnerability — neurons: 3-5 min; myocardium: 20-30 min; skeletal muscle: hours.
4. Oxygen-carrying capacity — anaemia and hypoxia worsen infarct size.
Evolution (e.g., renal infarct): 0-24 hr — ill-defined area; 24-48 hr — pale, distinct border with hyperaemic rim; days to weeks — scar (fibrosis replaces necrotic tissue).
Red versus White Infarction
SELF-CHECK
A patient with mitral stenosis and atrial fibrillation suddenly develops severe left loin pain. Imaging shows a pale wedge-shaped lesion in the kidney with a hyperaemic rim. This is BEST explained by:
A. Red infarct due to renal venous occlusion
B. Red infarct due to dual blood supply of the kidney
C. Abscess formation from a septic embolus
D. White infarct due to arterial embolism to a solid end-arterial organ
Reveal Answer
Answer: D. White infarct due to arterial embolism to a solid end-arterial organ
AF with mitral stenosis creates left atrial stasis → mural thrombus → systemic arterial embolism. The kidney has an end-arterial supply with no effective collaterals, so occlusion of a renal artery branch produces a white (anaemic) infarct — pale, firm, and wedge-shaped. The hyperaemic rim is reactive congestion in the surviving tissue at the margin. A venous cause would produce a red infarct; the kidney does not have a dual blood supply comparable to the lung.
Shock: Definition, Types & Pathogenesis of Septic Shock
Shock and Pathogenesis of Septic Shock
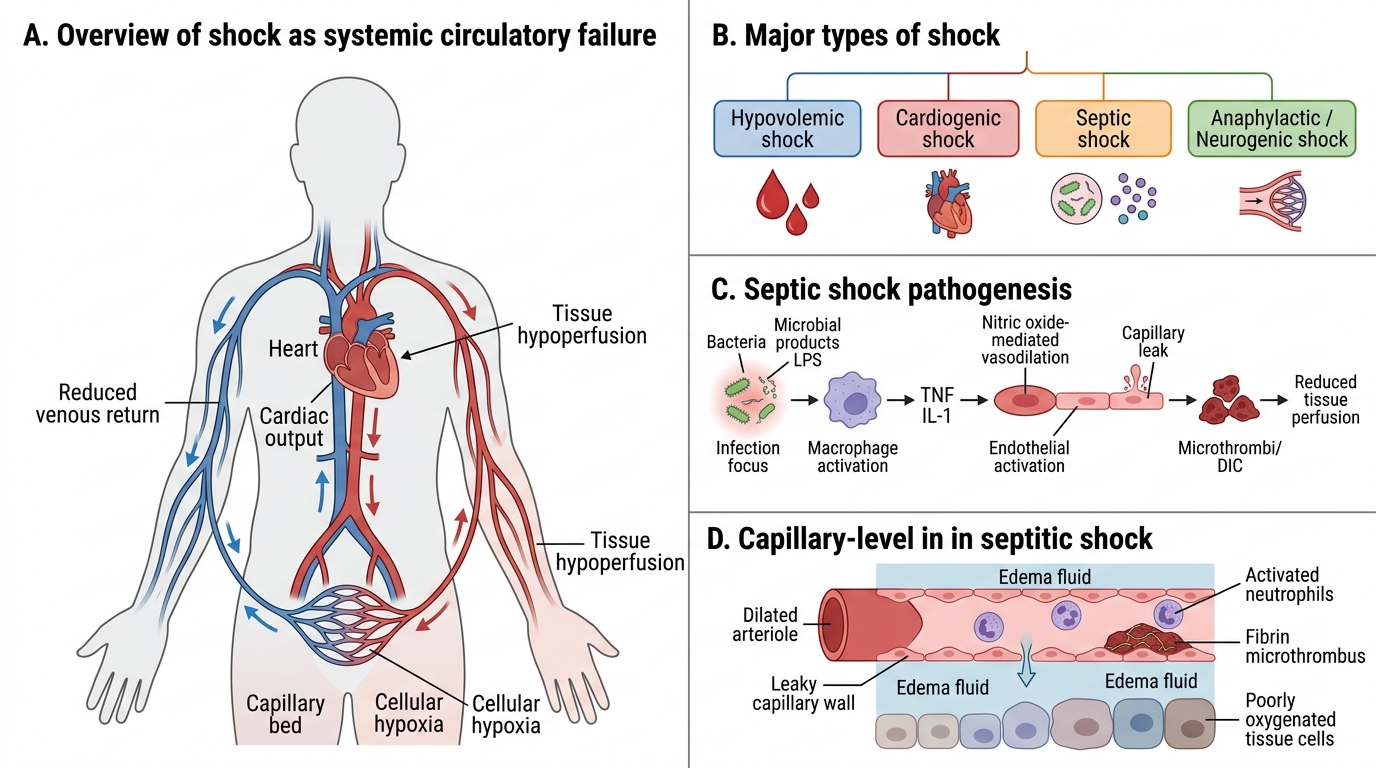
Shock is a state of systemic hypoperfusion of tissues resulting in cellular hypoxia and dysfunction, which if uncorrected leads to irreversible cell injury and death. It is not simply low blood pressure — it is a failure of oxygen delivery relative to demand.
Classification by mechanism:
| Type | Primary mechanism | Classic example |
|---|---|---|
| Hypovolaemic | Decreased circulating volume | Haemorrhage, burns, severe dehydration |
| Cardiogenic | Pump failure (↓ cardiac output) | Massive MI, severe arrhythmia, cardiac tamponade |
| Distributive — Septic | Massive vasodilation + flow maldistribution | Gram-negative/gram-positive sepsis, fungal |
| Distributive — Anaphylactic | IgE-mediated vasodilation + ↑ vascular permeability | Bee sting, penicillin reaction |
| Distributive — Neurogenic | Loss of vasomotor tone | Spinal cord injury, high spinal anaesthesia |
| Obstructive | Mechanical obstruction to flow | Massive PE, tension pneumothorax, cardiac tamponade |
Septic shock pathogenesis:
1. Infection → bacteraemia. Gram-negative: LPS (lipopolysaccharide/endotoxin); gram-positive: lipoteichoic acid, peptidoglycan.
2. LPS binds TLR4/CD14 on monocytes/macrophages → massive cytokine release: TNF-α, IL-1, IL-6, IL-8 (cytokine storm).
3. Cytokine storm effects:
• Endothelial activation → iNOS → excess nitric oxide → profound vasodilation → hypotension.
• ↑ Vascular permeability → 'third spacing' → functional hypovolaemia.
• Neutrophil activation → tissue injury (ROS, proteases).
• Endothelial damage → procoagulant state → DIC.
4. DIC — widespread microvascular thrombosis consumes clotting factors + platelets → paradoxical bleeding. Microthrombi in kidneys, lungs, adrenals → multi-organ dysfunction.
5. Compensatory anti-inflammatory response (CARS) follows SIRS — immunosuppression → risk of secondary infections.