Page 7 of 18
PA5.3-5 | Thrombosis, Embolism, Infarction & Shock — SDL Guide (Part 3)
Stages of Shock
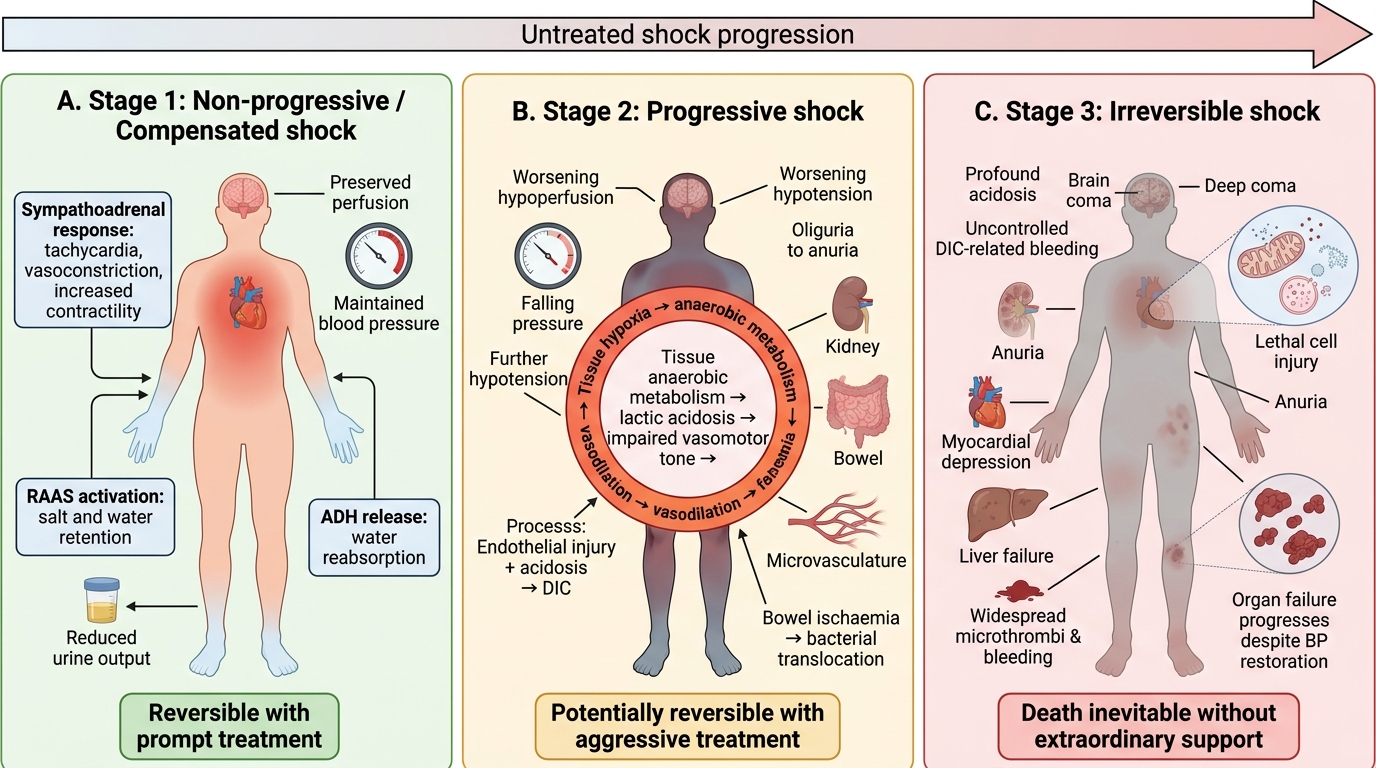
All types of shock progress through three stages if untreated:
Stage 1 — Non-progressive (Compensated) Shock:
Reflex compensatory mechanisms maintain perfusion to vital organs.
• Baroreceptor activation → sympathoadrenal discharge → tachycardia, vasoconstriction, ↑ contractility.
• RAAS activated → salt + water retention.
• ADH release → water reabsorption.
• Clinical: tachycardia, cool peripheries, maintained BP, reduced urine output. Reversible with prompt treatment.
Stage 2 — Progressive Shock:
Compensatory mechanisms overwhelmed. Widespread tissue hypoxia → anaerobic metabolism → lactic acidosis.
• Acidosis impairs vasomotor tone → vasodilation → further hypotension → viscous cycle.
• Endothelial injury + acidosis → DIC (especially septic shock).
• Bowel ischaemia → bacterial translocation amplifies injury.
• Clinical: worsening hypotension, oliguria → anuria, confusion, metabolic acidosis, multi-organ dysfunction. Potentially reversible with aggressive treatment.
Stage 3 — Irreversible Shock:
Lethal cell injury — mitochondrial dysfunction, lysosomal rupture, myocardial depression, hepatic failure.
• Even if BP is restored, organ failure progresses.
• Clinical: anuria, deep coma, profound acidosis, uncontrolled DIC-related bleeding. Death inevitable without extraordinary support.
Stages of Shock
CLINICAL PEARL
The lactate trap in septic shock: A patient may maintain a 'normal' blood pressure on vasopressors yet remain in progressive shock — tissues are still hypoperfused. Serum lactate > 2 mmol/L (or > 4 mmol/L in severe septic shock) unmasks occult hypoperfusion. The Surviving Sepsis Campaign uses lactate clearance (>10% reduction in 2 hours) as a resuscitation endpoint — not BP alone. Pathologically, this reflects the shift from aerobic to anaerobic glycolysis producing lactate as tissues exhaust their oxygen supply.
Morphological Changes in Shock
Morphological Changes in Shock
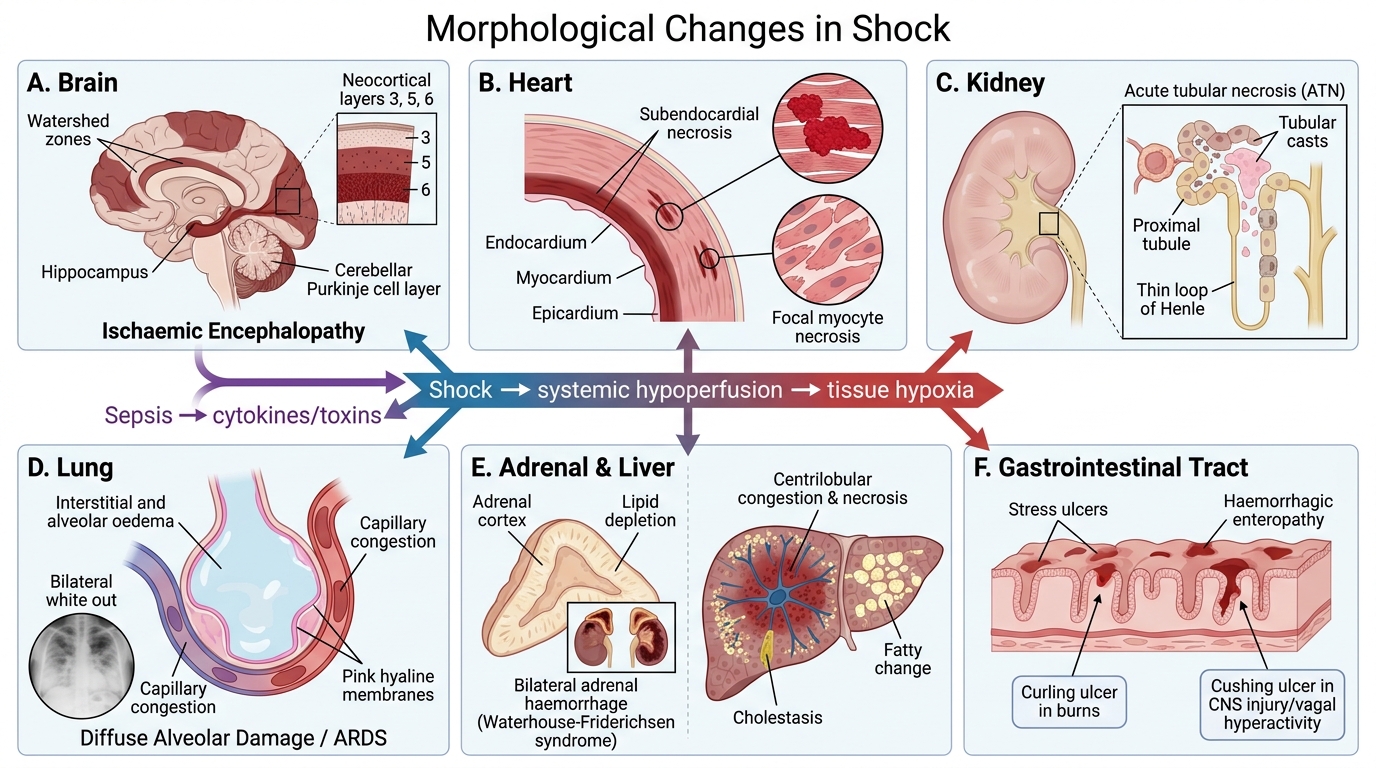
Shock injures every organ through hypoxia and (in sepsis) direct cytokine/toxin effects:
Brain: ischaemic encephalopathy — neuronal necrosis in watershed zones (boundaries between major arterial territories); most vulnerable: hippocampus, Purkinje cells of cerebellum, neocortex layers 3, 5, 6.
Heart: subendocardial necrosis (farthest from coronary supply); focal myocyte necrosis; contraction band necrosis (catecholamine surge).
Kidneys: acute tubular necrosis (ATN) — patchy necrosis of proximal tubule + thin loop of Henle; tubular casts; pale swollen kidneys grossly. Clinically: oliguria → anuria → acute kidney injury. ATN is reversible (tubular epithelium regenerates) — unlike cortical necrosis.
Lungs: diffuse alveolar damage (DAD/ARDS) — capillary congestion, interstitial + alveolar oedema, hyaline membrane formation (fibrin + plasma proteins); organisation with fibrosis in survivors. CXR: bilateral 'white out'; refractory hypoxia.
Adrenals: cortical cell lipid depletion (stored cholesterol consumed for stress-response steroidogenesis); in meningococcal sepsis: bilateral haemorrhagic necrosis — Waterhouse-Friderichsen syndrome.
Liver: centrilobular congestion and necrosis (pericentral hepatocytes most vulnerable to hypoxia); fatty change; cholestatic jaundice in sepsis.
GI tract: stress ulcers — Curling ulcers (burn victims), Cushing ulcers (CNS injury, vagal hyperactivity); haemorrhagic enteropathy.
SELF-CHECK
Autopsy of a patient who died after 5 days of septic shock reveals: pale swollen kidneys with necrotic proximal tubules, bilateral adrenal haemorrhage, hyaline membranes in alveoli, and subendocardial myocyte necrosis. Which finding is the MAIN cause of the oliguria/anuria during life?
A. Subendocardial myocyte necrosis reducing cardiac output
B. Diffuse alveolar damage reducing oxygen delivery to kidneys
C. Acute tubular necrosis of the proximal tubules
D. Bilateral adrenal haemorrhage causing cortisol deficiency
Reveal Answer
Answer: C. Acute tubular necrosis of the proximal tubules
Acute tubular necrosis (ATN) directly causes oliguria/anuria in shock. Ischaemia + cytotoxic injury destroy proximal tubular epithelium, preventing reabsorption and urine concentration. The good news: tubular epithelium regenerates, so ATN is reversible with adequate renal support — unlike cortical necrosis. The other findings contribute to multi-organ failure but do not directly explain the renal failure.