Page 15 of 24
PA6.7 | Benign vs Malignant Morphology — Practical — SDL Guide
Learning Objectives
- Identify and describe gross features that distinguish benign from malignant neoplasms on specimen examination
- Recognise microscopic features of malignancy (anaplasia, invasion, abnormal mitoses) on H&E-stained sections
- Apply a systematic reading approach — gross circumscription → micro architecture → cytologic atypia → invasion → diagnosis
- Grade tumour differentiation as well-differentiated, moderately differentiated, poorly differentiated, or undifferentiated
- Distinguish carcinoma in situ from invasive carcinoma based on basement membrane integrity
INSTRUCTIONS
In your practical classes and OSPE stations you will be asked to look at a specimen jar or a glass slide and say whether the tumour is benign or malignant — and how confident you are. This module walks you through the systematic decision framework pathologists use, from the first glance at a gross specimen to the high-power cytologic criteria that clinch malignancy. Mastering this pattern recognition skill is the foundation of all surgical pathology reporting and is tested in both theory and practical examinations.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 6 (Neoplasia) (textbook)
- Harsh Mohan — Textbook of Pathology, 8th ed., Ch 8 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
The surgical registrar hands you a formalin-fixed specimen labelled 'Breast lump, 42-year-old female.' Before you cut, you note the surface is irregular, the overlying skin is puckered, and the cut section is gritty and white with stellate extensions into surrounding fat. You already know the answer before the microscope is switched on. How? Because the gross features alone are telling you this tumour has infiltrated and provoked a desmoplastic stromal response — two cardinal signs of malignancy. This module teaches you to read both jars and slides the way a pathologist does: systematically, quickly, and with confidence.
WHY THIS MATTERS
PA6.7 is examined in every undergraduate practical and OSPE. More importantly, the same pattern-recognition skill applies throughout your clinical career — the surgeon needs to know whether to take a wide margin, the oncologist needs a grade, and the patient needs an honest prognosis. Understanding morphology is not memorising lists; it is developing an eye that works on any tissue, any tumour.
RECALL
From your Year-1 Cell Biology and this cluster's earlier SDLs, you should already be able to answer:
- What is a neoplasm, and how does it differ from hyperplasia?
- What is a proto-oncogene, and what happens when it mutates?
- What do the terms differentiation and anaplasia mean at the cellular level?
- What is the role of the basement membrane in separating in situ from invasive cancer?
If any of these feel shaky, spend five minutes reviewing SDL 1 (Hallmarks of Cancer) before continuing.
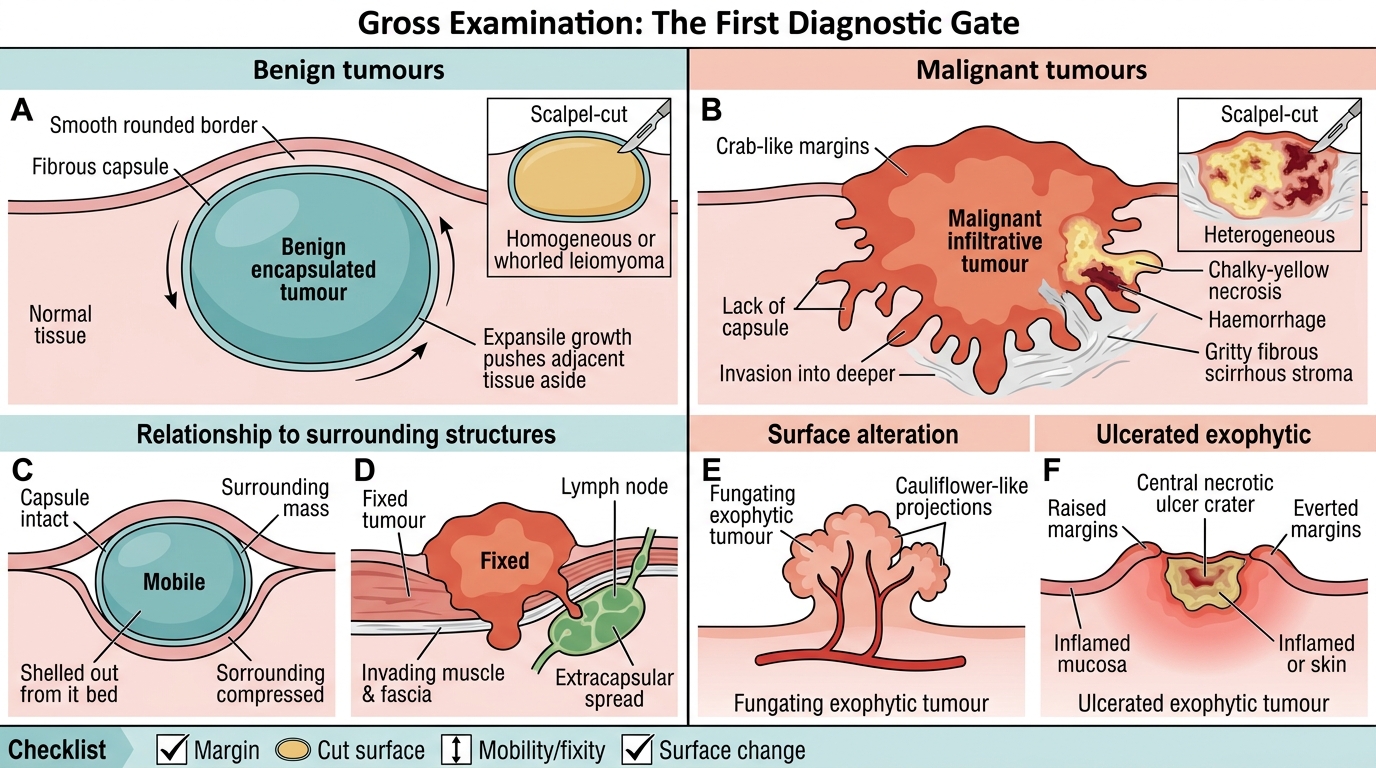
Step 1 — Gross Examination: The First Diagnostic Gate
Before a slide is ever cut, the gross specimen tells a story. Train yourself to assess four parameters on every specimen:
1. Margin character
Benign tumours grow by expansion — they push surrounding tissue aside and develop a smooth, rounded border. Many are enclosed within a fibrous capsule (e.g., lipoma, uterine leiomyoma). Malignant tumours grow by infiltration — irregular, poorly defined margins that blend into adjacent tissue, sometimes described as crab-like (cancer derives from the Greek word for crab).
2. Consistency and cut-surface
Benign tumours tend to be homogeneous on cut surface — a lipoma is uniformly yellow-tan, a leiomyoma shows a characteristic whorled pattern of interlacing smooth muscle fascicles. Malignant tumours are heterogeneous: areas of necrosis (soft, chalky-white or yellow) and haemorrhage (dark red) reflect outgrowth of the blood supply. An invasive breast carcinoma cuts with a gritty resistance (scirrhous quality) due to abundant fibrous stroma.
3. Relationship to surrounding structures
Benign tumours are freely mobile — you can shell them out of their bed. Malignant tumours are fixed to deeper structures because they have grown into them. A clinically fixed axillary node signals not just malignancy but extracapsular spread.
4. Surface alterations in exophytic tumours
When a tumour outgrows its blood supply on the surface it becomes fungating (cauliflower-like projections) or ulcerated (central ischaemic necrosis creates a crater). Both patterns are strongly associated with surface malignancies (skin, gastrointestinal tract, cervix).
Gross Clues to Benign and Malignant Tumours
| Feature | Benign | Malignant |
|---|---|---|
| Margins | Well-circumscribed, encapsulated | Irregular, infiltrative |
| Cut surface | Homogeneous | Necrosis + haemorrhage |
| Mobility | Freely mobile | Fixed |
| Surface | Smooth or pedunculated | Fungating or ulcerated |
SELF-CHECK
A 35-year-old woman has a 4 cm uterine mass. Grossly it is white, firm, and shows a whorled pattern on cut section with no haemorrhage or necrosis. The overlying serosa is smooth. What is the most likely diagnosis?
A. Uterine leiomyoma
B. Uterine leiomyosarcoma
C. Endometrial carcinoma invading myometrium
D. Rhabdomyosarcoma
Reveal Answer
Answer: A. Uterine leiomyoma
The whorled cut surface, sharp circumscription, homogeneous appearance, and absence of necrosis or haemorrhage are classic gross features of a benign leiomyoma (fibroid). Leiomyosarcoma, the malignant counterpart, would show haemorrhage, necrosis, and irregular margins. Endometrial carcinoma arises from the mucosa and invades inward; rhabdomyosarcoma is a skeletal-muscle tumour not expected here.
Step 2 — Low-Power Microscopy: Architecture First
When you place the slide on the stage, always start at scanning power (×4 or ×10) before moving to high power. Architecture — the spatial organisation of cells — is often more informative than individual cell details.
Benign tumour architecture
Benign tumours reproduce the architecture of their tissue of origin. A benign glandular tumour (adenoma) forms recognisable glands lined by orderly, uniform cells. Smooth muscle cells in a leiomyoma are arranged in intersecting fascicles that mirror normal myometrium. There is maintained polarity — cells know which way is 'up' (apical) and which way is 'down' (basal).
Malignant tumour architecture
Malignant tumours show loss of normal architecture proportional to their degree of malignancy. In a well-differentiated carcinoma you can still recognise gland-like structures; in a poorly differentiated carcinoma the cells grow in solid sheets with no glandular organisation; in an undifferentiated (anaplastic) carcinoma even the cell lineage may be unclear without special stains.
Invasion at low power
At the tumour edge, look for:
- Tongues of malignant cells pushing into stroma without a capsule
- Perineural invasion — tumour cells wrapping around nerve bundles (a key gross stage feature in pancreatic and prostate cancer)
- Lymphovascular invasion (LVI) — cohesive clusters of malignant cells within endothelium-lined vascular or lymphatic spaces
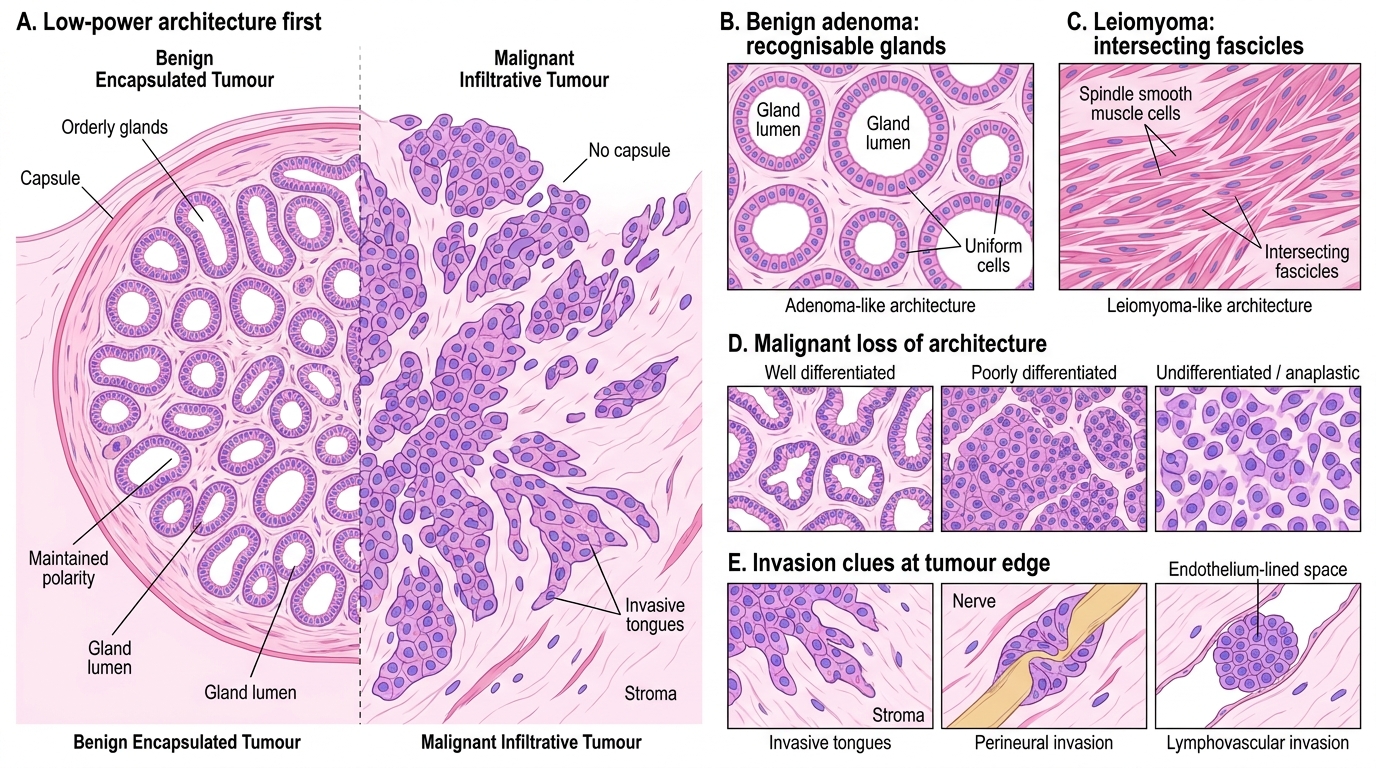
Low-Power Microscopy: Architecture and Invasion in Tumours
Step 3 — High-Power Microscopy: Cytologic Features of Malignancy (Anaplasia)
Switch to ×20–×40 for cytologic detail. The six hallmarks of anaplasia (cellular dedifferentiation) are the microscopic signature of malignancy:
1. Pleomorphism
Cellular pleomorphism means variation in cell size and shape within the same tumour. Benign cells are monomorphic (uniform). In an anaplastic tumour you may see cells five times the size of their neighbours. Nuclear pleomorphism — variation in nuclear size, shape, and contour — is particularly significant.
2. Increased nuclear-to-cytoplasmic (N:C) ratio
Normal epithelial cells have a small nucleus relative to abundant cytoplasm. Malignant cells have enlarged nuclei that dominate the cell, producing a high N:C ratio (the nucleus looks too big for the cell).
3. Hyperchromasia
Malignant nuclei stain darkly with haematoxylin (hyperchromatic) due to increased DNA content and condensed chromatin. The nucleus appears deeply purple rather than the pale vesicular appearance of a normal resting cell.
4. Prominent and irregular nucleoli
Active transcription in rapidly proliferating cells produces large, prominent nucleoli. In malignancy, nucleoli are often irregular in number and shape — 'owl-eye' nucleoli (Reed–Sternberg cells) are a dramatic example.
5. Abnormal and atypical mitoses
All dividing cells have mitoses, but malignant mitoses are abnormal: tripolar spindles, ring-form mitoses, asymmetric division. A single unequivocal atypical mitosis in a section is strong evidence of malignancy. Even the number of normal mitoses matters — many malignant tumours have elevated mitotic counts (expressed as mitoses per 10 high-power fields).
6. Tumour giant cells
Fusion of anaplastic cells or failure of cytokinesis produces mononucleate or multinucleate tumour giant cells — large cells with bizarre, hyperchromatic nuclei. Distinct from inflammatory giant cells (osteoclast-type, foreign-body type).
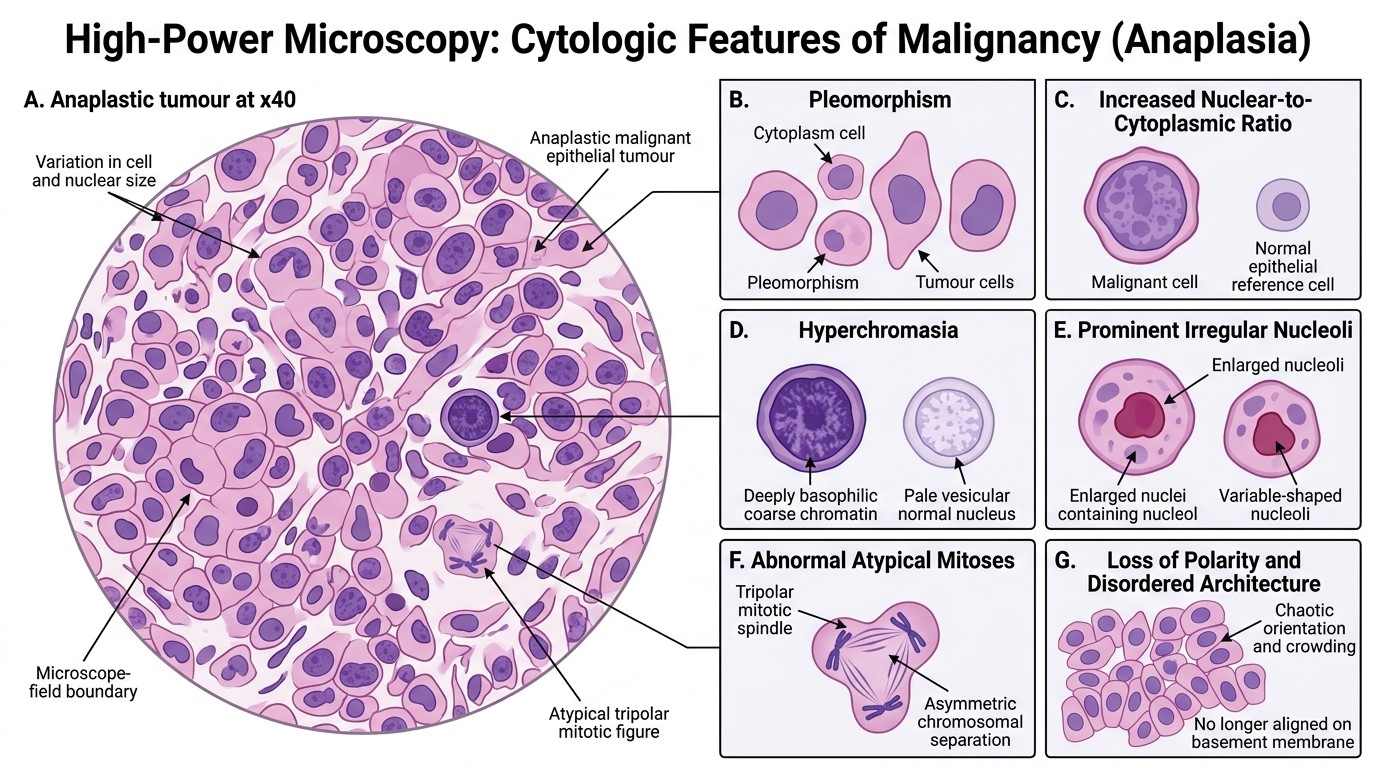
Cytologic Features of Malignancy: Anaplasia
SELF-CHECK
On high-power examination of a breast mass biopsy, you see marked variation in cell size and shape, deeply hyperchromatic nuclei, prominent irregular nucleoli, and a tripolar mitotic figure. The most specific indicator of malignancy in this list is:
A. Deeply hyperchromatic nuclei
B. Tripolar (atypical) mitotic figure
C. Variation in cell size
D. Prominent nucleoli
Reveal Answer
Answer: B. Tripolar (atypical) mitotic figure
An atypical mitotic figure (tripolar, ring-form, asymmetric) is the most specific single feature because normal cells never produce structurally abnormal spindles — it is direct evidence of chromosomal instability that accompanies malignant transformation. Hyperchromasia, pleomorphism, and prominent nucleoli can each occur in reactive or regenerating benign tissues; an atypical mitosis cannot.