Page 16 of 24
PA6.7 | Benign vs Malignant Morphology — Practical — SDL Guide (Part 2)
Step 4 — Invasion and the Basement Membrane: In Situ vs Invasive
The single most important criterion separating a carcinoma in situ from an invasive carcinoma is integrity of the basement membrane (BM).
Carcinoma in situ (CIS)
Malignant cytologic features are present — pleomorphism, hyperchromasia, atypical mitoses — but the cells have not broken through the BM. The tumour is confined to the epithelial compartment. CIS is by definition non-metastatic (no access to lymphatics or vessels). Examples: ductal carcinoma in situ (DCIS) of breast, cervical intraepithelial neoplasia (CIN) grade 3, carcinoma in situ of bladder.
Invasive carcinoma
Once malignant cells secrete proteases (matrix metalloproteinases, cathepsins) and disrupt the BM, they enter the stroma. This is the point of no return for metastatic potential. On H&E, you see irregular nests and cords of carcinoma cells within a reactive stroma (often desmoplastic — dense fibrous tissue laid down in response to tumour invasion).
Lymphovascular invasion (LVI)
LVI is identified as cohesive carcinoma emboli within endothelium-lined spaces (distinguished from retraction artefact by the presence of red cells or smooth muscle in the vessel wall). LVI predicts regional lymph node metastasis and is a key adverse prognostic feature reported in surgical specimens.
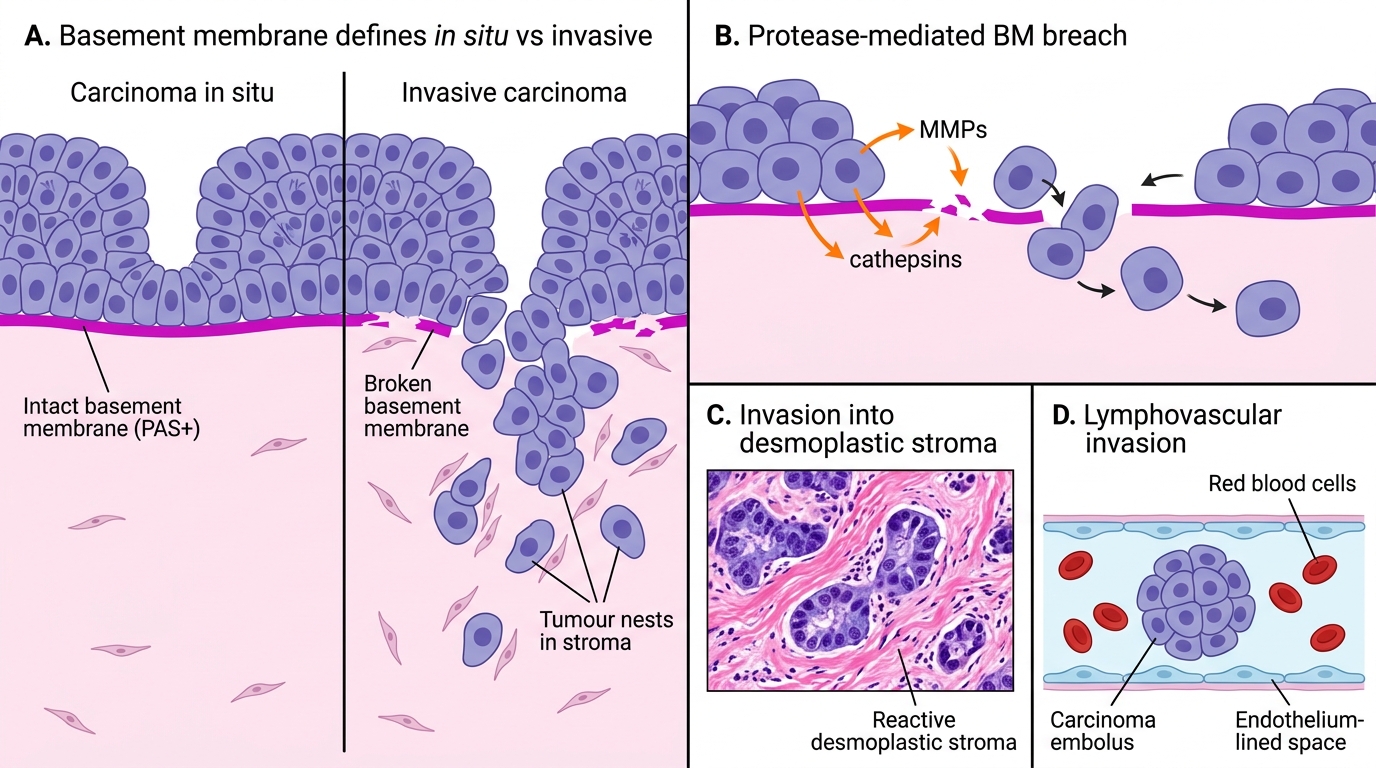
Basement Membrane Breach: In Situ vs Invasive Carcinoma
SELF-CHECK
A cervical biopsy shows full-thickness replacement of the squamous epithelium by cells with high N:C ratio, numerous mitoses (including atypical), and loss of surface maturation. There is no extension beyond the basement membrane. What is the correct diagnosis?
A. Invasive squamous cell carcinoma
B. Koilocytic atypia (HPV effect)
C. Squamous cell carcinoma in situ (CIN 3)
D. Severe reactive atypia
Reveal Answer
Answer: C. Squamous cell carcinoma in situ (CIN 3)
Full-thickness epithelial atypia with atypical mitoses and loss of maturation, confined to the epithelium above an intact basement membrane, is CIN 3 / squamous carcinoma in situ. The key differentiating point from invasive carcinoma is the intact BM — no stromal invasion means no metastatic potential yet. Reactive atypia shows preserved maturation and polarity; koilocytic atypia is characterised by perinuclear haloes and raisinoid nuclei (HPV cytopathic effect).
Step 5 — Tumour Differentiation Grading
Tumour Differentiation Grading
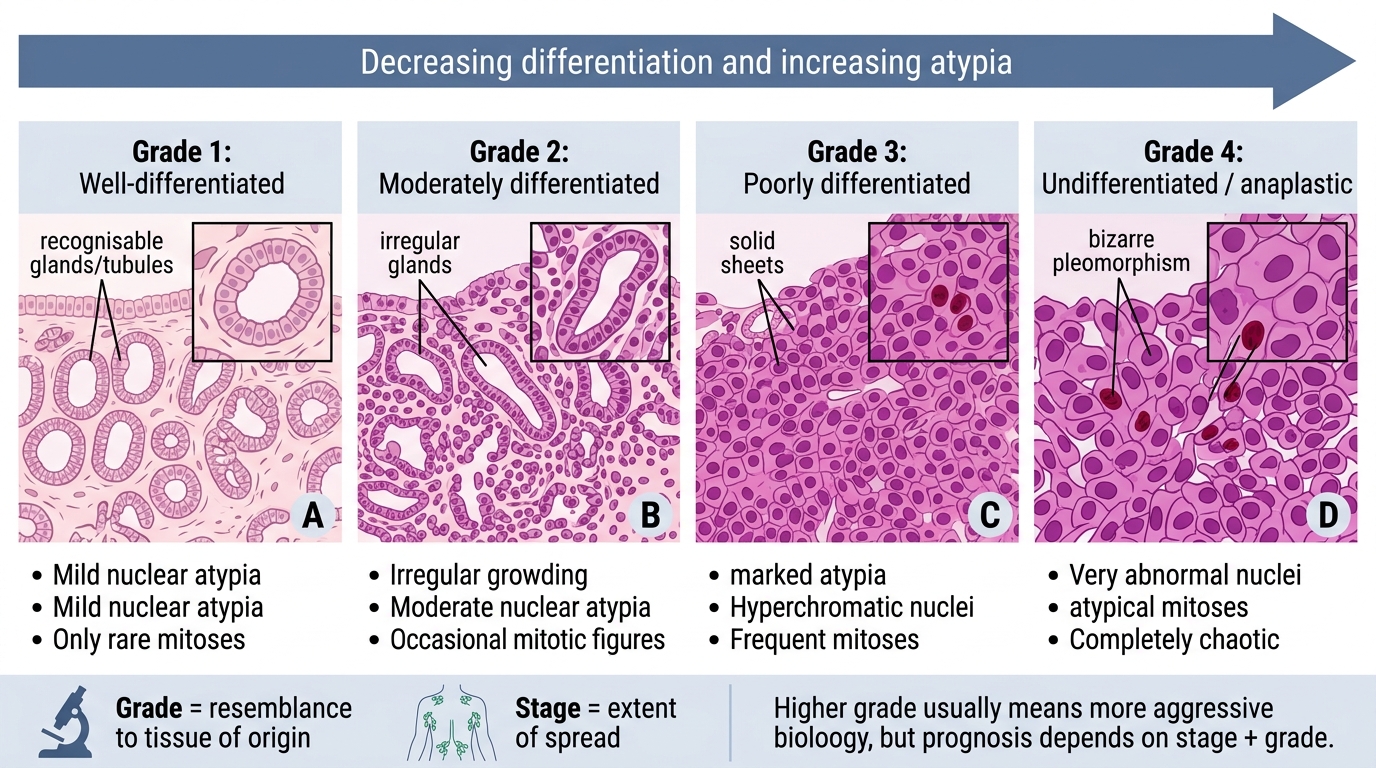
Differentiation refers to how closely a tumour resembles its tissue of origin, both structurally and functionally. Grading quantifies this resemblance.
Grading system (WHO/NMC standard)
| Grade | Term | Morphologic criteria |
|---|---|---|
| Grade 1 | Well-differentiated | Closely resembles normal tissue; recognisable glands/tubules; minimal atypia; few mitoses |
| Grade 2 | Moderately differentiated | Partial resemblance; irregular glands; moderate atypia; moderate mitoses |
| Grade 3 | Poorly differentiated | Difficult to recognise tissue of origin; solid sheets; marked atypia; frequent mitoses |
| Grade 4 | Undifferentiated (anaplastic) | No resemblance to any normal tissue; bizarre pleomorphism; rampant atypical mitoses |
Clinical correlation
Higher grade = more aggressive biology = worse prognosis (generally). However, grade must always be interpreted alongside stage. A Grade 1 carcinoma already metastatic to multiple nodes (Stage IV) carries a worse prognosis than a Grade 3 carcinoma confined to the primary site (Stage I). Grade and stage are complementary — not interchangeable.
Tumour-specific grading systems
Many tumours have disease-specific grading: Gleason score (prostate), Scarff–Bloom–Richardson (breast), Fuhrman (renal cell). These refine the 4-tier WHO framework using additional morphologic parameters. You will encounter them in applied pathology.
CLINICAL PEARL
The gritty, stellate breast lump — scirrhous (fibrotic) carcinoma — is one of the most recognisable gross patterns. The gritty resistance on cutting comes from calcium deposits within necrotic tumour foci and from dense desmoplastic collagen. When you feel this while cutting, pause and dictate: 'ill-defined, stellate, grey-white, gritty, 3 cm mass with no capsule, invading adjacent fat.' That single sentence already communicates malignancy to the reporting pathologist even before any slide is read.
H5P Image Hotspots Activity — Four-Panel Morphology Grid
The following image should be used as an H5P Image Hotspots interactive activity. Each panel hosts two or three clickable hotspots that pop up with the feature name and a brief teaching note. Study the composite before attempting the identification quiz below.
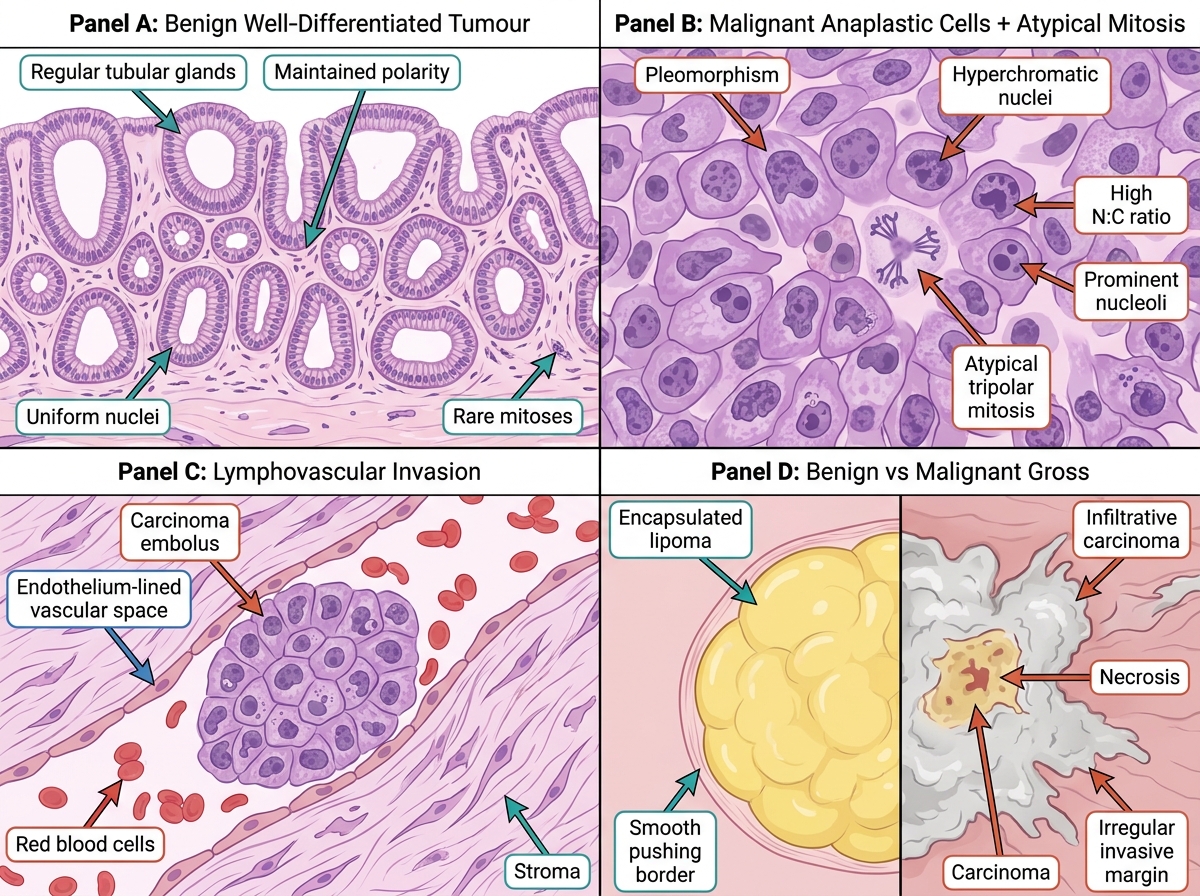
Morphological Features of Benign and Malignant Neoplasms
For the hotspot activity, configure the following interaction points:
- Panel A: Hotspot at gland lumen → 'Regular tubular glands: maintained architecture = well-differentiated benign'; Hotspot at epithelial layer → 'Uniform basal nuclei, maintained polarity — compare with Panel B'
- Panel B: Hotspot at atypical mitosis → 'Atypical (tripolar) mitosis: specific for malignancy'; Hotspot at large pleomorphic nucleus → 'Pleomorphism + hyperchromasia: two of the six anaplasia criteria'
- Panel C: Hotspot at carcinoma cluster → 'Lymphovascular invasion: predicts nodal metastasis — must be reported in surgical specimen'
- Panel D: Hotspot at encapsulated lipoma → 'Capsule + smooth margin: benign gross pattern'; Hotspot at infiltrating carcinoma → 'Stellate margin + necrosis: malignant gross pattern'
SELF-CHECK
Looking at Panel B of the morphology grid, you identify cells with a tripolar mitotic figure, hyperchromatic nuclei, and a high N:C ratio. The pathologist reports this as 'Grade 3 invasive ductal carcinoma.' What additional feature in Panel C is the most important adverse prognostic finding to include in the report?
A. Desmoplastic stromal reaction
B. Tumour necrosis
C. High mitotic count
D. Lymphovascular invasion
Reveal Answer
Answer: D. Lymphovascular invasion
Lymphovascular invasion (LVI) is the most important adverse prognostic feature in Panel C because it provides a direct anatomical route for metastatic spread to regional lymph nodes and beyond. Its presence upgrades nodal risk assessment and influences decisions about adjuvant therapy. Desmoplasia, necrosis, and high mitotic count are all adverse features, but LVI has the strongest independent prognostic impact on nodal and distant metastasis in carcinomas.