Page 17 of 24
PA6.7 | Benign vs Malignant Morphology — Practical — SDL Guide (Part 3)
Putting It All Together: The Systematic Reading Protocol
Use this sequence every time you approach a specimen or slide. Do not skip steps.
Gross protocol (specimen in jar)
1. Identify the organ/tissue
2. Measure and describe the mass
3. Assess margins: circumscribed vs infiltrative
4. Describe cut surface: homogeneous / whorled / necrosis / haemorrhage / gritty
5. Assess mobility: encapsulated vs fixed
6. Note surface changes: smooth / fungating / ulcerated
7. Provisional gross conclusion: benign (expansile, encapsulated) or malignant (infiltrative, heterogeneous)
Micro protocol (H&E slide)
1. ×4 scan: overall architecture — is tissue organisation maintained?
2. ×10 tumour edge: capsule or invasion? Perineural invasion? LVI?
3. ×20 architecture: gland/tubule formation → estimate differentiation grade
4. ×40 cytology: pleomorphism, N:C ratio, hyperchromasia, nucleoli, mitoses — count atypical mitoses
5. Return to ×10: basement membrane intact (CIS) or breached (invasive)?
6. Final diagnosis: benign vs malignant + grade (if malignant) + invasion status
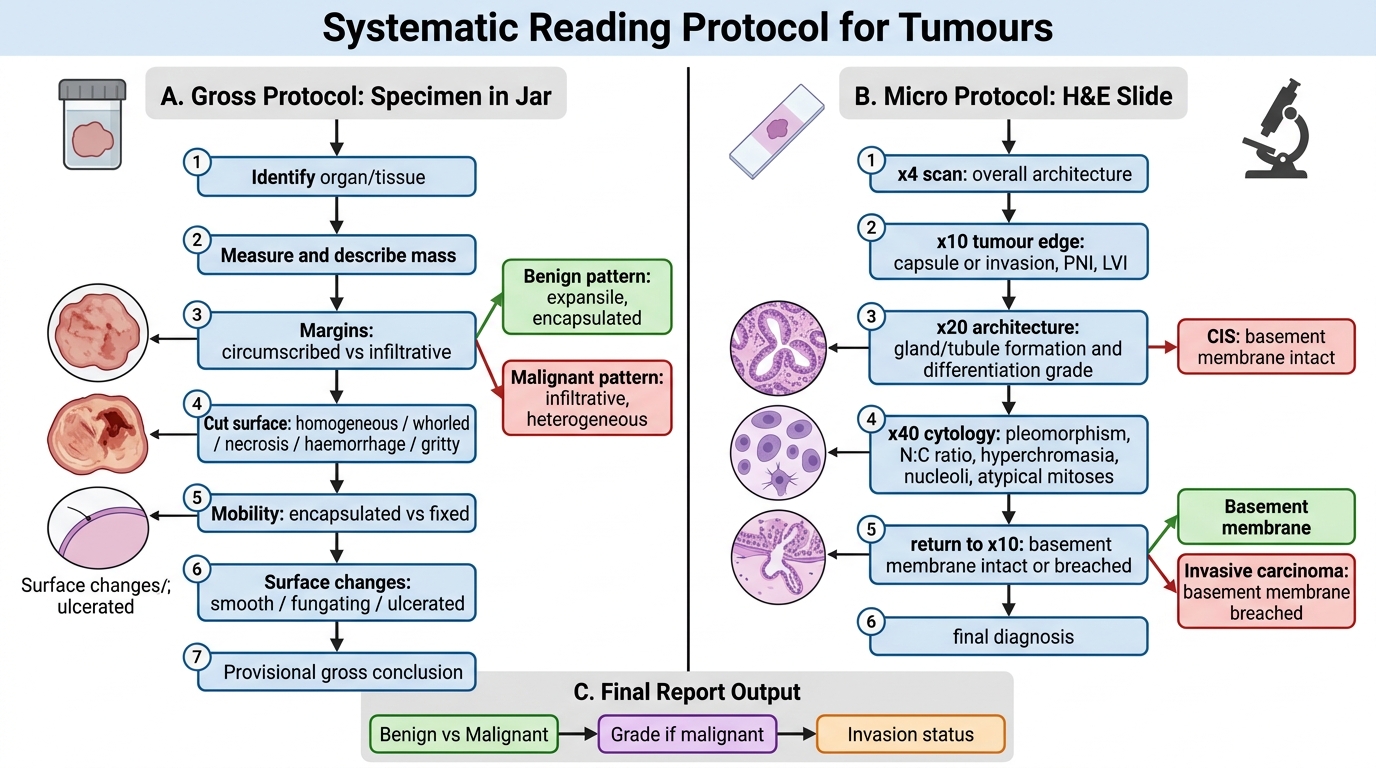
Systematic Reading Protocol for Tumours
SELF-CHECK
In the systematic micro reading protocol, at which magnification step would you first reliably identify lymphovascular invasion?
A. ×4 overall scan of architecture
B. ×10 examination of the tumour edge
C. ×40 cytologic assessment
D. ×20 gland formation estimate
Reveal Answer
Answer: B. ×10 examination of the tumour edge
Lymphovascular invasion is first reliably identified at ×10 when examining the tumour periphery — you need to see the intact endothelial-lined space and the carcinoma emboli within it, which is best appreciated at this power where you can see both the vessel structure and the surrounding context. At ×4 the tissue is too small to resolve individual vessel-tumour relationships. ×40 is used for cytologic criteria; ×20 for gland architecture.
CLINICAL PEARL
Retraction artefact vs true LVI — one of the most common practical pitfalls. Retraction during tissue processing creates clear spaces around tumour nests that mimic vascular invasion. True LVI is distinguished by: (1) endothelial lining of the space, (2) presence of red blood cells or valvular smooth muscle, (3) irregular contour of the space following the vascular wall rather than the tumour nest. When in doubt, an immunostain for D2-40 (lymphatics) or CD31/CD34 (blood vessels) resolves the question.
SELF-CHECK
A 60-year-old man has a 6 cm colonic mass. Microscopy shows glands recognisable as colonic-type but with irregular contours, moderate nuclear atypia, and 4 mitoses per 10 high-power fields. There is invasion through the muscularis propria. What is the correct grade?
A. Grade 1 — Well-differentiated
B. Grade 3 — Poorly differentiated
C. Grade 2 — Moderately differentiated
D. Grade 4 — Undifferentiated
Reveal Answer
Answer: C. Grade 2 — Moderately differentiated
Grade 2 (Moderately differentiated) — recognisable but irregular glands with moderate atypia and a moderate mitotic count places this squarely in the middle-tier. Grade 1 would require well-formed regular glands with minimal atypia. Grade 3 requires solid sheet growth with loss of glandular architecture. Grade 4 (undifferentiated) would show no recognisable tissue pattern whatsoever. The invasion through muscularis propria is a staging criterion (pT2 minimum), not a grading criterion.