Page 1 of 24
PA6.1 | Neoplasia — Definitions, Nomenclature & Characteristics — SDL Guide
Learning Objectives
- Define neoplasia using Willis's definition and identify its two structural components
- Apply correct nomenclature to classify benign and malignant tumours from epithelial, mesenchymal, and other tissue origins
- Recognise the important exceptions where the '-oma' suffix denotes malignancy
- Compare benign and malignant tumours across the four key characteristics: differentiation/anaplasia, rate of growth, local invasion, and metastasis
- Describe the cytological features of anaplasia
- List the three main routes of metastasis and correlate them with tumour type
- Distinguish carcinoma in situ from invasive carcinoma
INSTRUCTIONS
Understanding tumour nomenclature and the biological differences between benign and malignant neoplasms is the essential foundation for all of surgical pathology. Every diagnosis you write as a clinician — and every histopathology report you interpret — depends on the framework in this module. Master the language and the four key characteristics before proceeding to oncogenesis and molecular pathology.
References
- Robbins & Kumar: Basic Pathology, 11th ed., Ch 5 — Neoplasia (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 6 — Neoplasia (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old woman presents with a lump in her breast. The radiologist calls it a 'mass'. The surgeon calls it a 'tumour'. The histopathologist calls it a 'neoplasm'. Are they describing the same thing? More importantly — is it benign or malignant? The answer lies not in the gross appearance alone, but in a precise biological language that pathologists have spent over a century developing. By the end of this module, you will read any histopathology report and immediately decode what the tumour is, where it came from, and how it is likely to behave.
WHY THIS MATTERS
PA6.1 is a core competency that underpins every other topic in tumour pathology. Misclassifying a tumour — calling a malignant melanoma a 'benign naevus', or confusing a leiomyosarcoma with a leiomyoma — can have fatal clinical consequences. The NMC expects you to demonstrate this competency in written examinations, viva voce, and at the bedside when correlating clinical findings with pathology reports.
RECALL
Before you begin, ask yourself:
• What is the difference between a 'tumour' and a 'cyst'? (Year-1 General Pathology)
• Name the two main tissue origins of body cells — epithelial and mesenchymal. Which organs are lined by epithelium?
• What does 'differentiation' mean in the context of embryology? Can a cell be 'undifferentiated'?
• Recall from Biochemistry: what controls the cell cycle? Which checkpoints prevent uncontrolled growth?
If any of these are hazy, spend 5 minutes reviewing before proceeding — they are the scaffolding for everything in this module.
Definition of Neoplasia
Definition and Components of Neoplasia
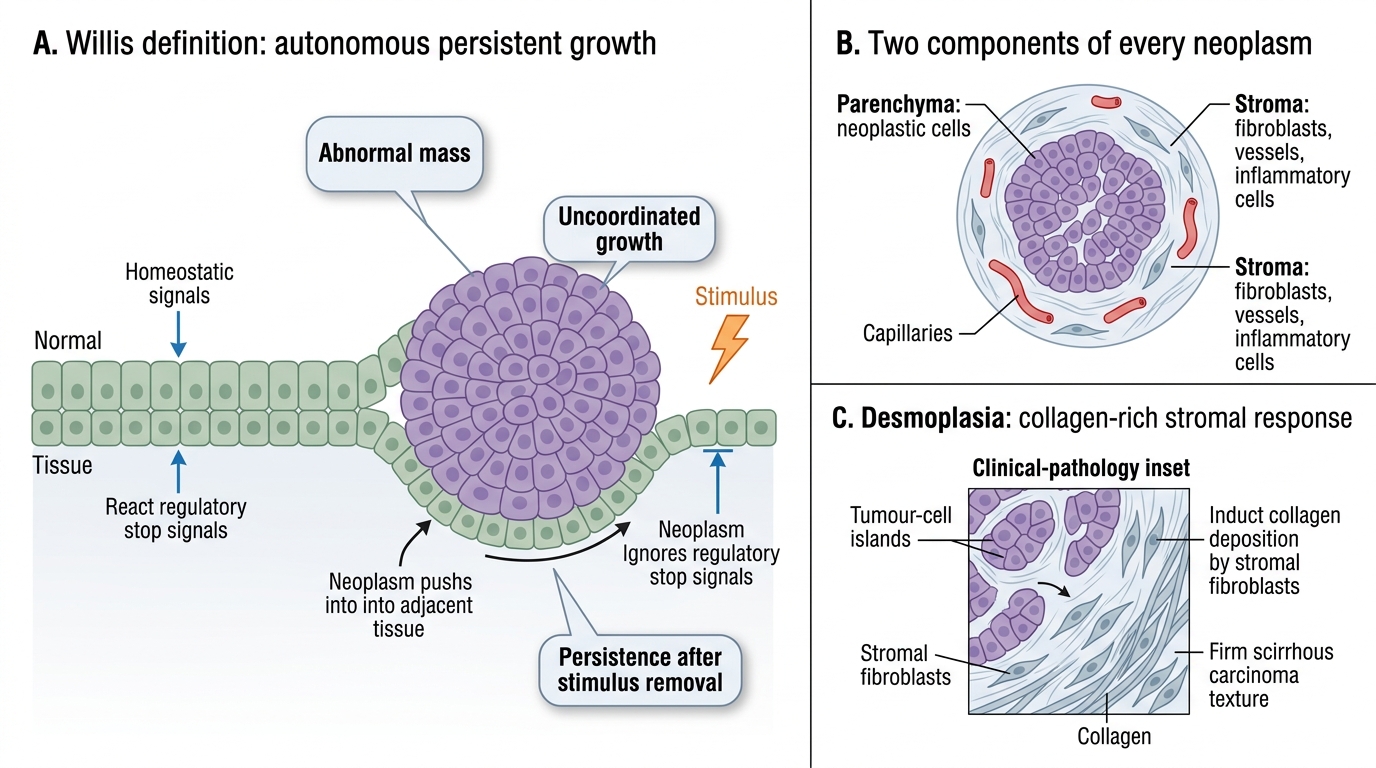
The most authoritative definition remains that of Willis (1952):
> "A neoplasm is an abnormal mass of tissue, the growth of which exceeds and is uncoordinated with that of the normal tissues, and persists in the same excessive manner after cessation of the stimuli which evoked the change."
Three elements of this definition deserve emphasis:
1. Abnormal mass — structurally distinct from surrounding normal tissue
2. Uncoordinated growth — the tumour obeys its own autonomous programme, not the body's homeostatic signals
3. Persistence — unlike a healing wound or a reactive proliferation (e.g., granulation tissue), the growth does not stop when the inciting stimulus is removed
The word tumour originally meant any swelling (Latin: tumor = swelling). It is now used synonymously with neoplasm. The word cancer is a colloquial term for any malignant neoplasm.
Two Components of Every Neoplasm
Two Components of Every Neoplasm
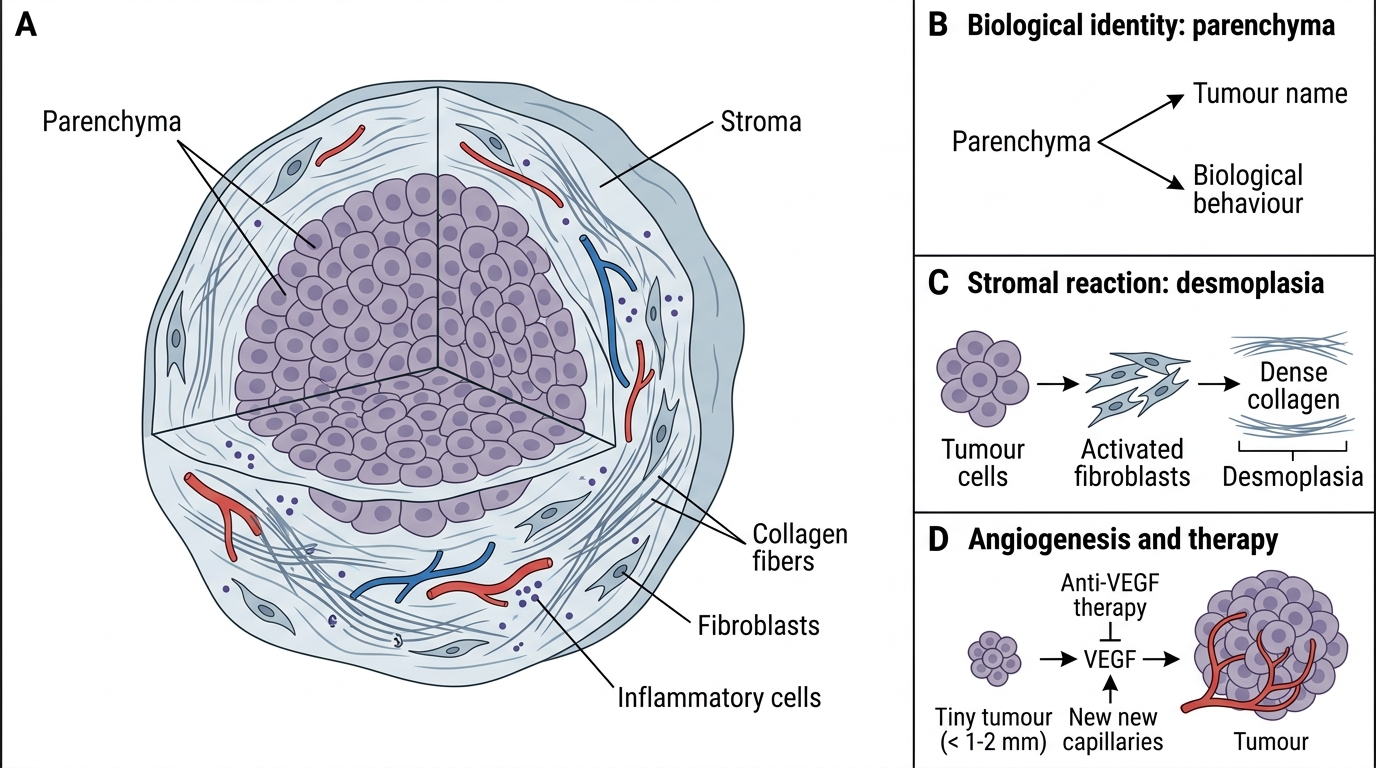
Every neoplasm — regardless of type — has exactly two components:
1. Parenchyma — the proliferating neoplastic cells themselves. This component determines the biological behaviour and the name of the tumour.
2. Stroma — the supporting connective tissue and blood vessels that the tumour induces the host to provide. Stroma consists of fibroblasts, myofibroblasts, inflammatory cells, and new capillaries.
When tumour cells stimulate abundant collagen deposition by stromal fibroblasts, the result is desmoplasia — the characteristic hard, 'scirrhous' feel of many carcinomas (e.g., scirrhous carcinoma of the breast). Desmoplasia is a stromal reaction, not part of the parenchyma.
Importance: A tumour cannot grow beyond 1–2 mm without inducing its own blood supply (angiogenesis via VEGF). Targeting the stroma (anti-VEGF therapy) is one mechanism of modern cancer treatment.
Nomenclature — The Language of Tumours
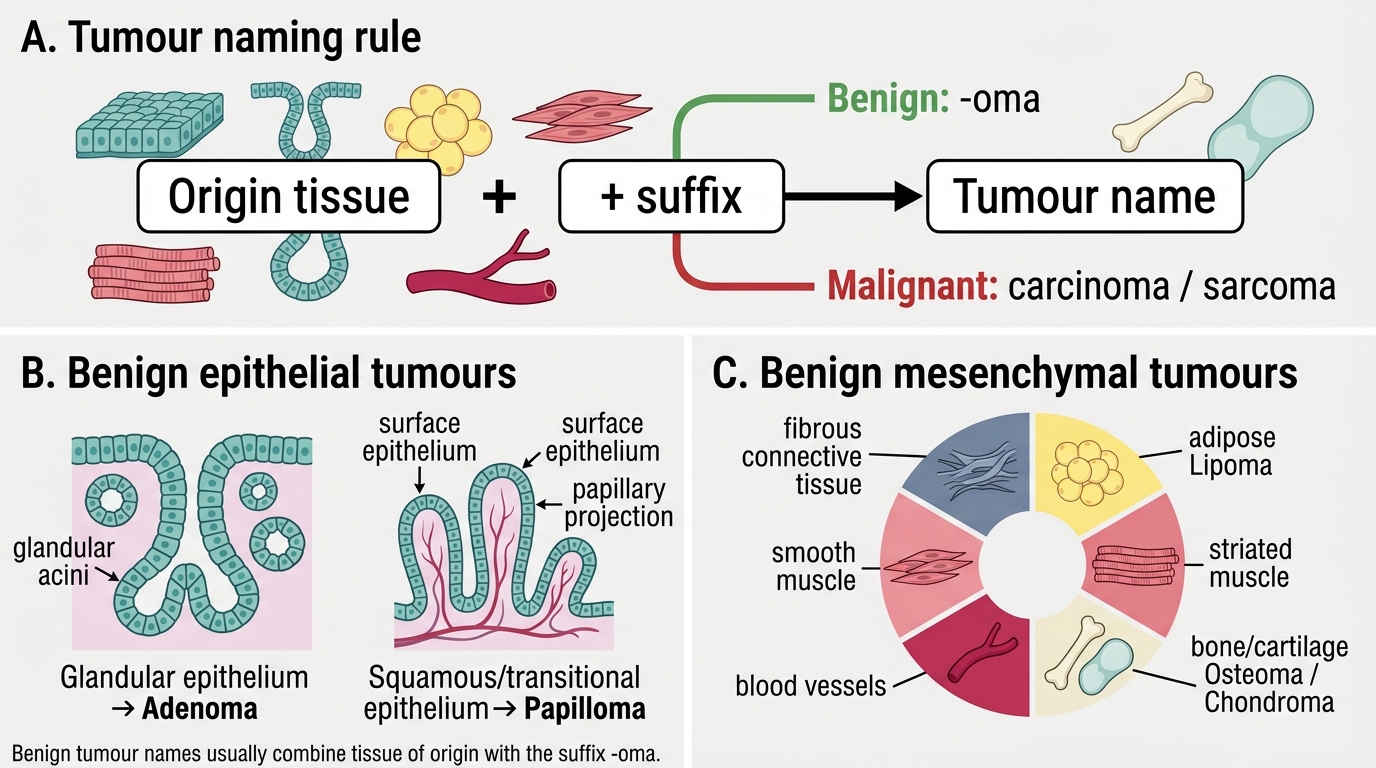
Tumour nomenclature is systematic: origin tissue + suffix indicates benign or malignant.
Benign tumours carry the suffix -oma:
| Origin tissue | Benign tumour name |
|---|---|
| Glandular epithelium | Adenoma |
| Squamous/transitional epithelium (surface projections) | Papilloma |
| Fibrous connective tissue | Fibroma |
| Adipose tissue | Lipoma |
| Smooth muscle | Leiomyoma |
| Striated muscle | Rhabdomyoma |
| Blood vessels | Haemangioma |
| Bone | Osteoma |
| Cartilage | Chondroma |
Malignant tumours follow a different logic:
- Malignant tumour of epithelial origin → carcinoma (e.g., adenocarcinoma, squamous cell carcinoma)
- Malignant tumour of mesenchymal origin → sarcoma (e.g., fibrosarcoma, liposarcoma, leiomyosarcoma, osteosarcoma)
- Malignant tumour of embryonal/primitive cells → -blastoma (e.g., neuroblastoma, retinoblastoma, nephroblastoma/Wilms' tumour, hepatoblastoma)
- Malignant tumour of haematopoietic cells → leukaemia or lymphoma
IMPORTANT — eponymous tumours: Ewing's sarcoma (malignant; primitive neuroectodermal), Hodgkin's lymphoma (malignant; B-cell lineage) — these carry the discoverer's name, not a tissue-derived name.
Tumour Nomenclature: Origin Tissue + Suffix