Page 2 of 24
PA6.1 | Neoplasia — Definitions, Nomenclature & Characteristics — SDL Guide (Part 2)
Critical Exceptions — Malignant Tumours with '-oma' Suffix
The most examination-critical exceptions are malignant neoplasms that carry the '-oma' suffix — a historical accident that now demands rote memorisation:
| Tumour name | Why it looks benign | Actual behaviour |
|---|---|---|
| Melanoma (malignant melanoma) | -oma suffix; once called 'naevocarcinoma' | Highly aggressive; metastasises early |
| Lymphoma | -oma suffix | Malignant haematopoietic neoplasm |
| Seminoma | -oma suffix | Malignant germ cell tumour of testis |
| Mesothelioma | -oma suffix | Malignant tumour of pleura/peritoneum |
| Hepatoma | -oma suffix; also called hepatocellular carcinoma | Malignant |
| Glioma (glioblastoma multiforme) | -oma suffix | Malignant CNS tumour |
Memory hook: 'MLSMH-G' — Melanoma, Lymphoma, Seminoma, Mesothelioma, Hepatoma, Glioma.
Special Tumour Categories
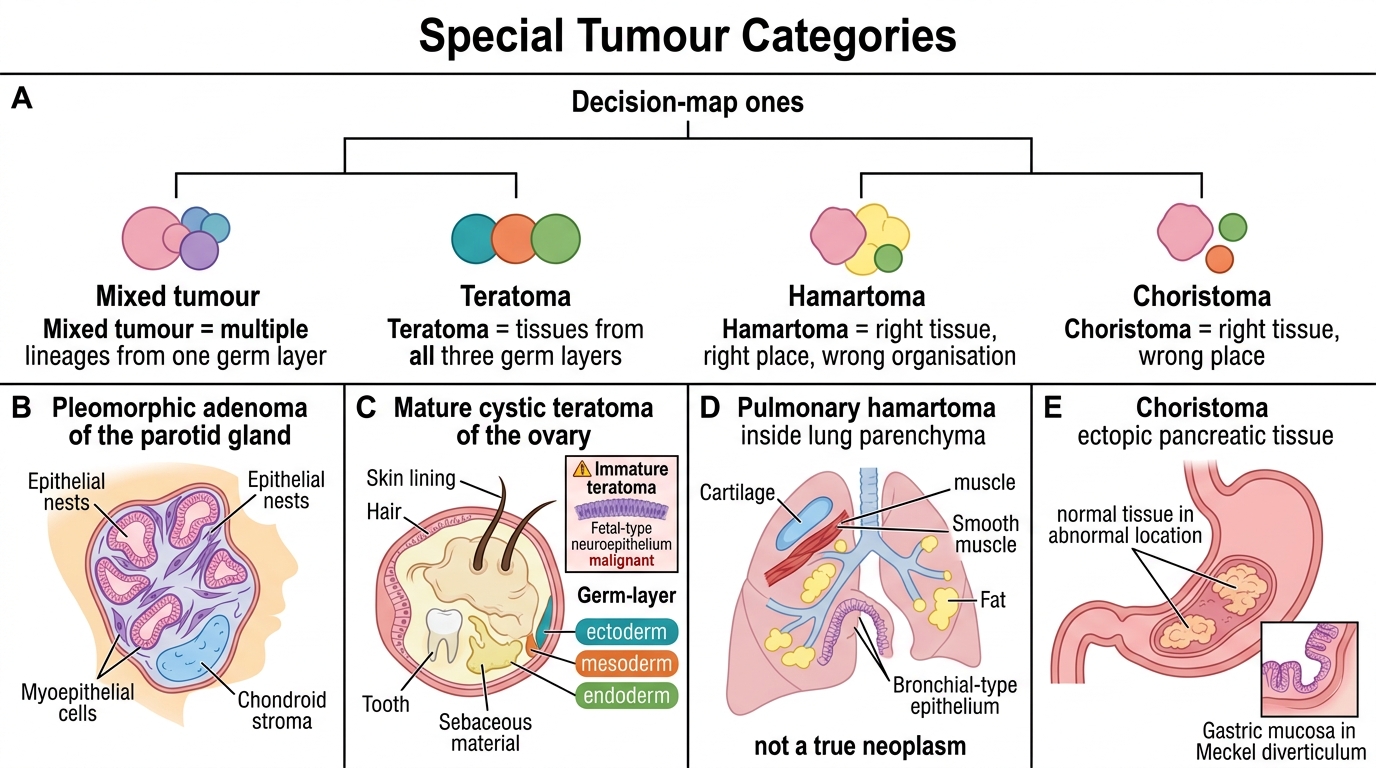
Special Tumour Categories
Mixed tumours contain two or more cell lineages arising from one germ layer (e.g., pleomorphic adenoma of the parotid = epithelial + myoepithelial + chondroid stroma; benign but locally recurrent).
Teratoma arises from totipotent germ cells and contains tissues derived from all three germ layers (ectoderm, mesoderm, endoderm). The classic example is the mature cystic teratoma (dermoid cyst) of the ovary — benign, contains hair/teeth/skin. Immature teratomas (containing fetal-type neuroepithelium) are malignant. Teratomas of the testis tend to be malignant regardless of maturity.
Hamartoma — a disorganised but non-neoplastic overgrowth of normal tissue elements native to a given organ (e.g., pulmonary hamartoma with cartilage + muscle + fat in the lung). It is NOT a true neoplasm.
Choristoma — a congenital rest of normal tissue in an abnormal location (e.g., pancreatic tissue in the stomach wall; gastric mucosa in Meckel's diverticulum). Also not a neoplasm.
Key distinction: Hamartoma = right tissue, right place, wrong organisation. Choristoma = right tissue, wrong place.
SELF-CHECK
A 35-year-old woman has a painless testicular mass. Biopsy shows a tumour with sheets of large uniform cells with clear cytoplasm and prominent nucleoli, resembling spermatocytes. The tumour is called a 'seminoma'. Which statement is MOST accurate?
A. It is benign because it carries the '-oma' suffix
B. It is a malignant germ cell tumour despite the '-oma' suffix
C. It is a mixed germ cell tumour arising from all three germ layers
D. It is a hamartoma of testicular tissue
Reveal Answer
Answer: B. It is a malignant germ cell tumour despite the '-oma' suffix
Seminoma is a classic exception — a malignant germ cell tumour of the testis that carries the misleading '-oma' suffix. It is exquisitely radiosensitive and carries a good prognosis if detected early, but it is unequivocally malignant. Options A and D are wrong by definition; option C describes a teratoma, not a seminoma.
Characteristics of Benign vs Malignant Tumours — Overview
The distinction between benign and malignant neoplasms rests on four fundamental characteristics. None is absolute on its own — the diagnosis is always a combination of histological and clinical features.
| Characteristic | Benign | Malignant |
|---|---|---|
| Differentiation / Anaplasia | Well-differentiated; resembles parent tissue | Variable; often poorly differentiated or anaplastic |
| Rate of growth | Slow; few mitoses | Rapid; many mitoses (often abnormal) |
| Local invasion | Non-invasive; often encapsulated | Invasive; infiltrates surrounding tissue |
| Metastasis | Absent | Present (defining feature of malignancy) |
IMPORTANT: Metastasis is the single most reliable criterion for malignancy. A tumour that has metastasised is by definition malignant — there are no exceptions.
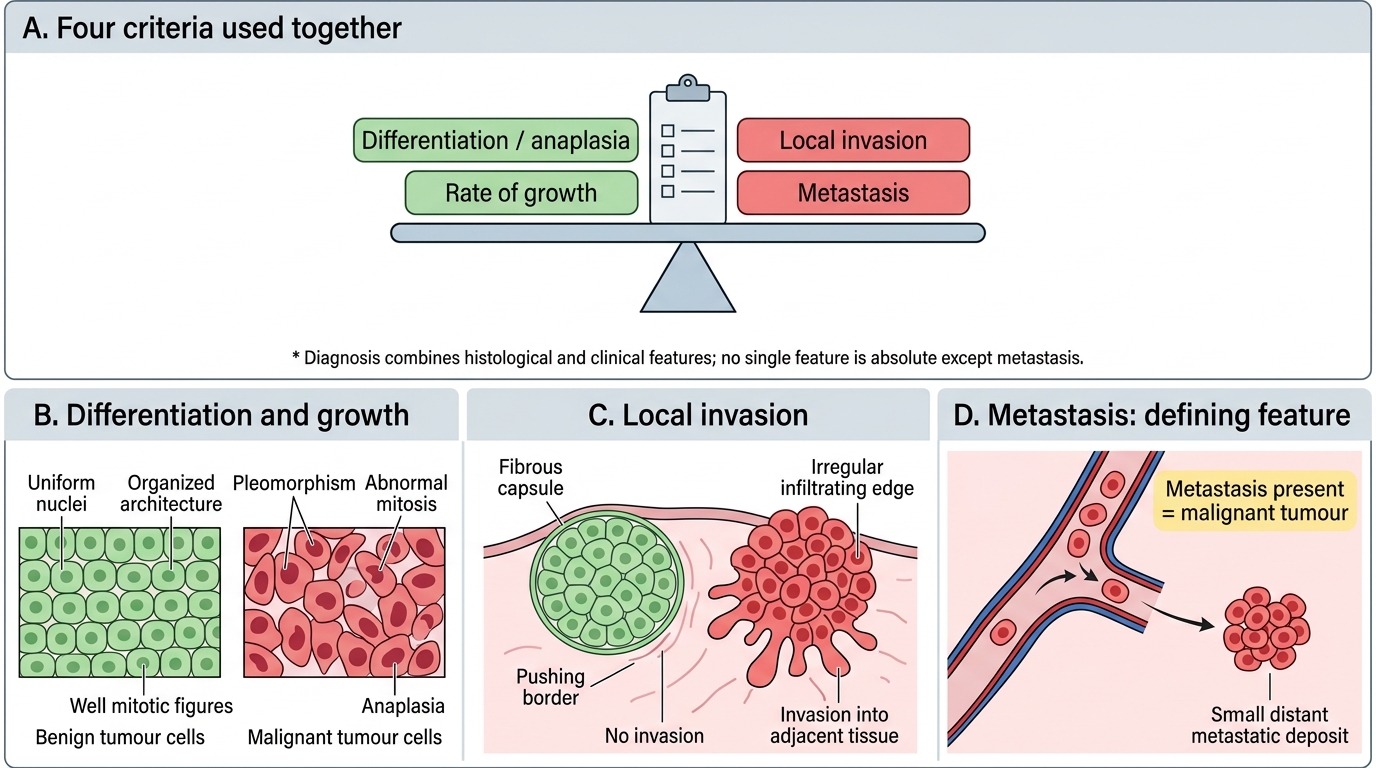
Benign vs Malignant Tumours: Core Diagnostic Features