Page 3 of 24
PA6.1 | Neoplasia — Definitions, Nomenclature & Characteristics — SDL Guide (Part 3)
Differentiation and Anaplasia
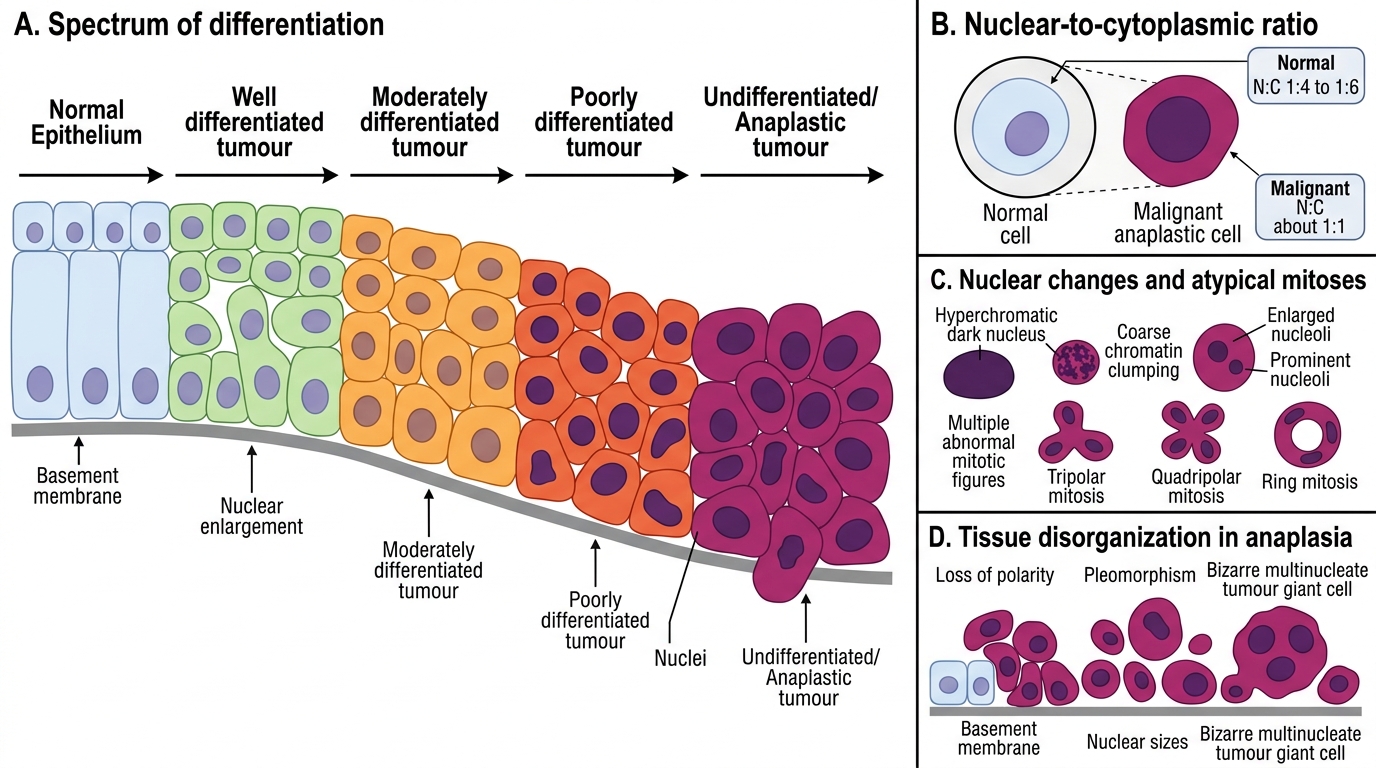
Differentiation refers to the extent to which neoplastic parenchymal cells resemble their normal counterparts morphologically and functionally.
- Well-differentiated tumours closely resemble normal tissue (e.g., a well-differentiated thyroid follicular carcinoma that still produces thyroglobulin)
- Moderately differentiated tumours show intermediate features
- Poorly differentiated tumours show minimal resemblance to normal tissue
- Undifferentiated / anaplastic tumours show no resemblance; cells appear primitive
Anaplasia (Greek: ana = backward; plasis = formation) is the hallmark of malignancy. It comprises:
1. Pleomorphism — variation in cell size and shape; cells and nuclei vary markedly in size
2. Nuclear changes — the most important diagnostic features:
- Increased nuclear-to-cytoplasmic (N:C) ratio (normal 1:4 to 1:6; malignant cells may be 1:1)
- Hyperchromasia — dark-staining nuclei due to excess DNA/chromatin clumping
- Prominent nucleoli (often multiple, enlarged); indicates increased rRNA synthesis
- Abnormal mitotic figures — tripolar, quadripolar, or ring mitoses (NOT just increased mitoses)
3. Loss of polarity — cells lose their normal orientation relative to basement membrane and to each other
4. Tumour giant cells — bizarre multinucleate giant cells formed by failed cytokinesis
NOTE: Increased mitoses alone are seen in benign rapidly-growing tissues (e.g., bone marrow, intestinal epithelium). It is the atypical mitotic figures that are pathognomonic of malignancy.
Differentiation and Anaplasia in Neoplasia
CLINICAL PEARL
Exam trap — 'well-differentiated' does NOT mean 'benign'. A well-differentiated follicular carcinoma of the thyroid looks almost identical to normal thyroid follicles on histology — yet it invades capsular blood vessels and metastasises haematogenously to bone and lung. Always correlate differentiation grade with invasion and metastasis status before making a final call.
Rate of Growth
Rate of Growth in Benign and Malignant Tumours
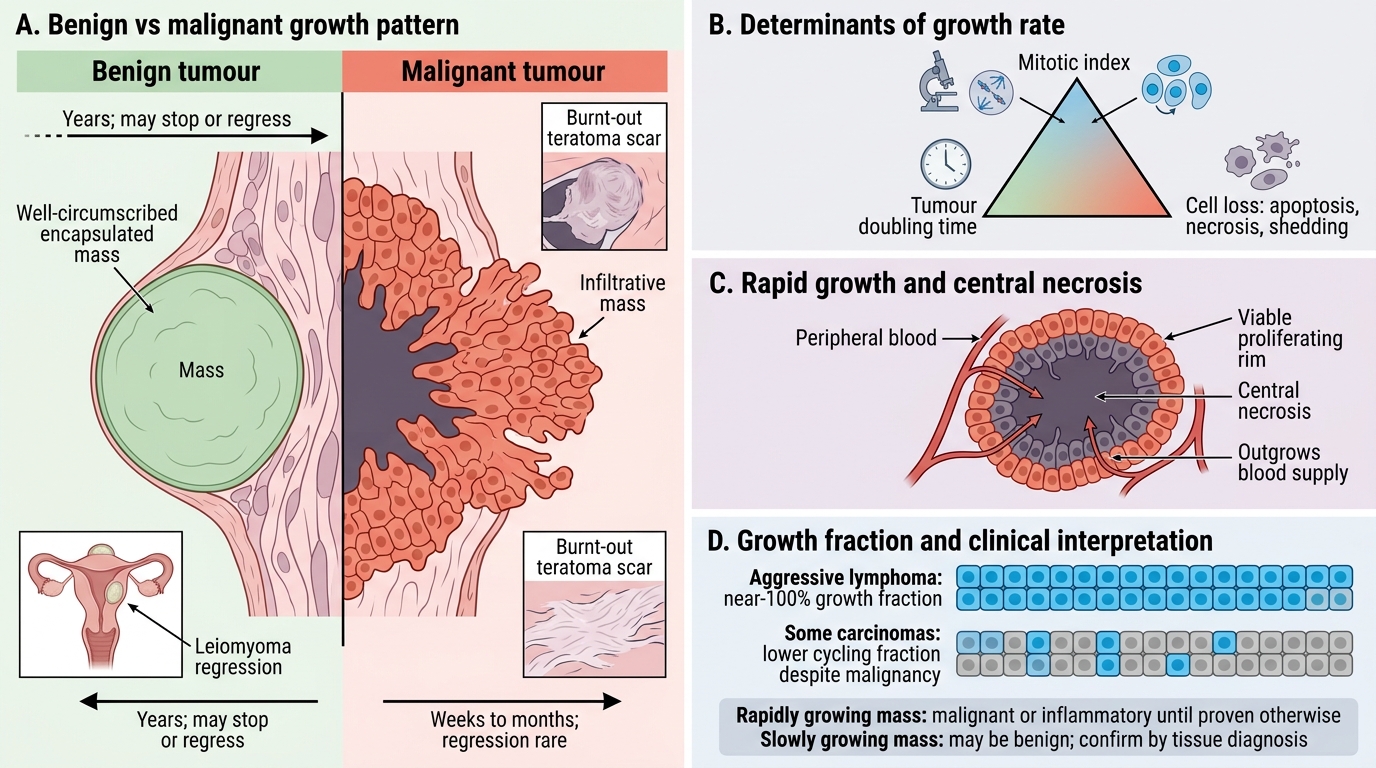
Malignant tumours generally grow faster than benign tumours, but there is significant overlap:
- Benign tumours grow slowly over years; many stop growing spontaneously (e.g., uterine leiomyomas often regress after menopause)
- Malignant tumours grow progressively; regression is rare and clinically significant (testicular teratomas occasionally regress, leaving a 'burnt-out' scar)
Growth rate correlates with:
1. Mitotic index — number of mitotic figures per 10 high-power fields
2. Tumour doubling time — varies from 20 days (Burkitt's lymphoma) to 200 days (some breast carcinomas)
3. Balance between cell production and cell loss (apoptosis, necrosis, shedding): a rapidly growing tumour may have massive central necrosis (outgrows its blood supply)
The growth fraction — proportion of cells actively cycling — is a better predictor of growth rate than mitotic count alone. Aggressive lymphomas have near-100% growth fractions; some carcinomas cycle slowly despite high malignant potential.
Clinically, a rapidly growing mass (days to weeks) is more likely malignant or inflammatory (abscess). A slowly growing mass (years) may be benign — but never assume so without tissue diagnosis.
Local Invasion
Local Invasion and Basement Membrane Breach
Local invasion is the second most important indicator of malignancy (after metastasis).
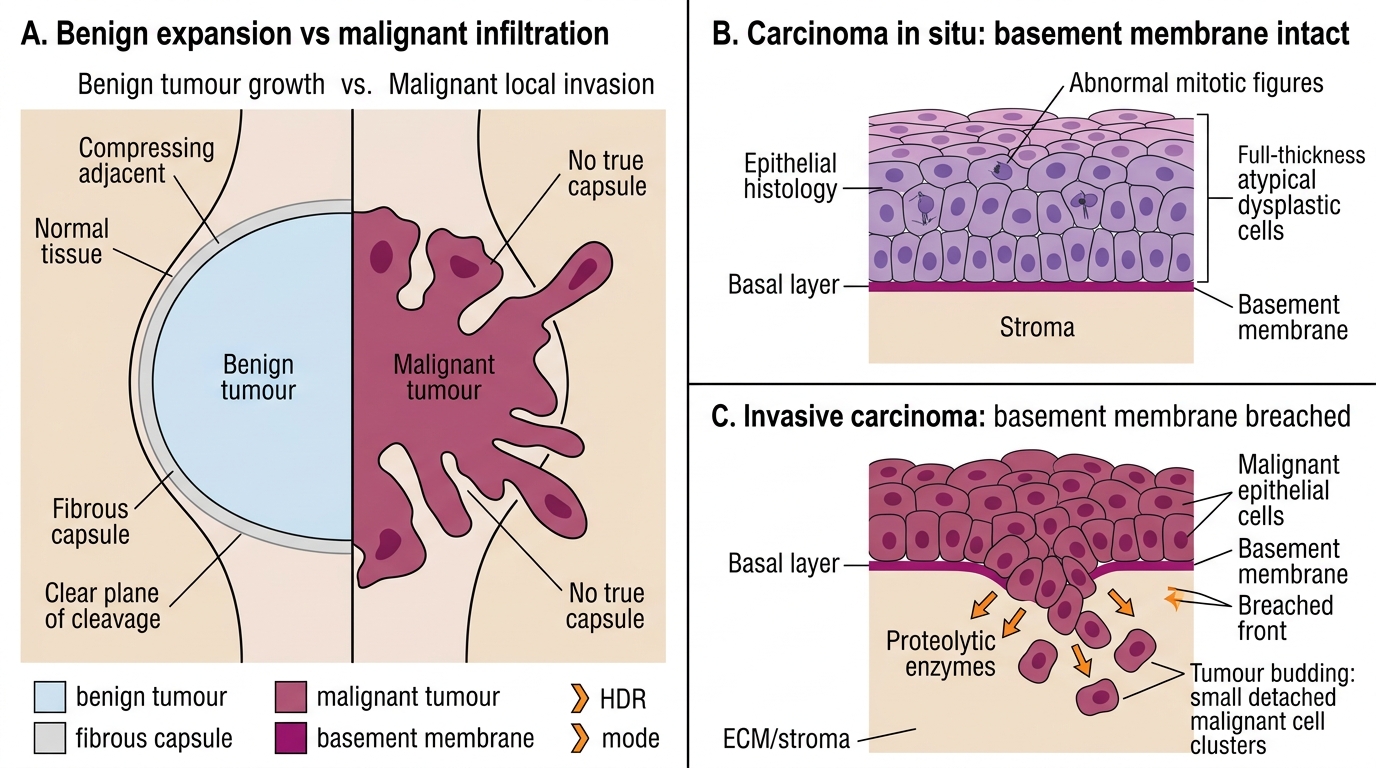
Benign tumours:
- Grow by expansion, compressing surrounding tissue
- Often develop a fibrous capsule (compressed stroma at the periphery)
- The capsule is a plane of cleavage — surgeons can 'shell out' a benign tumour
- Exception: some benign tumours (e.g., haemangiomas, aggressive fibromatosis/desmoid tumours) are NOT encapsulated and locally infiltrate without metastasising
Malignant tumours:
- Grow by infiltration — tumour cells invade adjacent normal tissue
- Rarely encapsulated; when a pseudocapsule forms, tumour 'fingers' extend beyond it
- Require proteolytic enzymes (matrix metalloproteinases, cathepsins) to degrade basement membrane and ECM
- Generate tumour budding at the invasive front (prognostic factor in colorectal carcinoma)
Carcinoma in situ (CIS): A malignant transformation where cells show all cytological features of malignancy (anaplasia, abnormal mitoses) but have NOT yet penetrated the basement membrane. CIS is fully curable by surgical excision. Once the basement membrane is breached → invasive carcinoma → metastatic risk.
SELF-CHECK
Histology of a cervical biopsy shows full-thickness dysplastic changes with abnormal mitoses extending to the epithelial surface. The basement membrane is intact. The MOST appropriate diagnosis is:
A. Cervical intraepithelial neoplasia grade 1 (CIN 1) — mild dysplasia
B. Invasive squamous cell carcinoma
C. Carcinoma in situ (CIS) / CIN 3 — basement membrane intact
D. Adenocarcinoma of the endocervix
Reveal Answer
Answer: C. Carcinoma in situ (CIS) / CIN 3 — basement membrane intact
Full-thickness dysplasia with intact basement membrane is the definition of carcinoma in situ (CIN 3 / CIS). The key distinguishing feature from invasive carcinoma is the intact basement membrane — once it is breached, the diagnosis becomes invasive carcinoma with metastatic potential. CIN 1 has only one-third thickness dysplasia. Adenocarcinoma is glandular, not squamous.