Page 4 of 24
PA6.1 | Neoplasia — Definitions, Nomenclature & Characteristics — SDL Guide (Part 4)
Metastasis — The Defining Feature of Malignancy
Metastasis is the dissemination of tumour cells from the primary site to a distant site where they establish secondary growths. It is the single most reliable criterion of malignancy — no benign tumour metastasises.
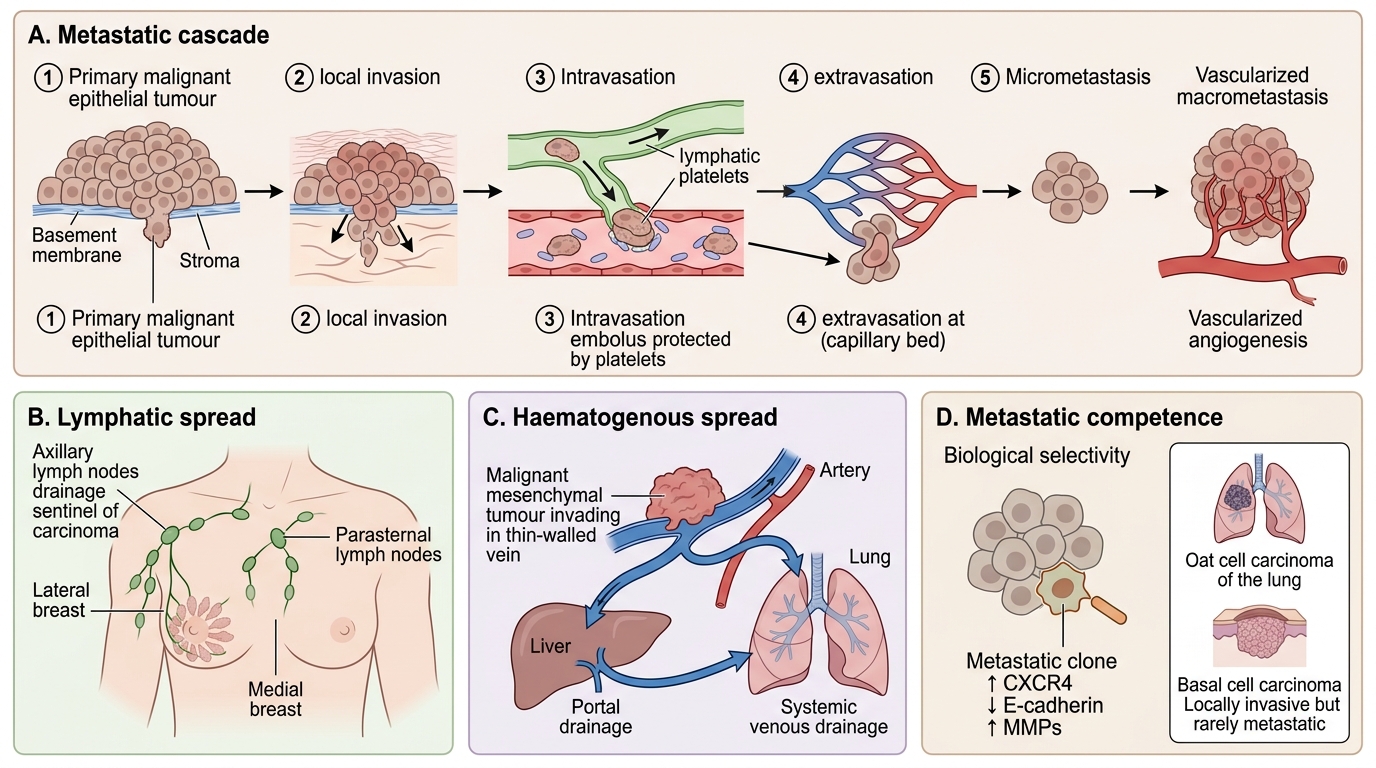
The metastatic cascade involves:
1. Local invasion through basement membrane
2. Intravasation — entry into blood vessels or lymphatics
3. Survival in the circulation (tumour cells evade immune destruction; form tumour emboli with platelets)
4. Extravasation — exit from circulation at distant site
5. Formation of micrometastases, then macrometastases (requires angiogenesis)
Not all malignant cells are equally capable of metastasis — only a subpopulation with specific properties (↑ CXCR4, ↓ E-cadherin, ↑ MMPs) can complete the cascade. This explains why some tumours metastasise early (oat cell carcinoma of lung) and others rarely do (basal cell carcinoma of skin — locally invasive but rarely metastasises).
Three main routes of metastasis:
1. Lymphatic spread — preferred route of carcinomas (epithelial tumours)
- Follows regional lymph node drainage
- First lymph node encountered = sentinel lymph node (SLN biopsy in breast cancer)
- Classic example: medial breast carcinoma → parasternal nodes; lateral breast → axillary nodes
2. Haematogenous spread — preferred route of sarcomas (mesenchymal tumours)
- Veins are invaded more than arteries (thinner walls, lower pressure)
- Portal vein drainage → liver (commonest site of haematogenous metastasis overall)
- Systemic venous drainage → lungs (second commonest site)
- 'Cannon ball' metastases in lung on chest X-ray: renal cell carcinoma, choriocarcinoma
- Batson's vertebral venous plexus explains vertebral metastases from prostate/breast (retrograde flow bypassing the IVC)
3. Transcoelomic / seeding — spread across body cavities
- Peritoneal cavity: ovarian carcinoma seeds peritoneum → Krukenberg tumour (gastric carcinoma → ovarian metastasis via transcoelomic route)
- Pleural cavity: lung/breast carcinomas → malignant pleural effusion
- CSF seeding: medulloblastoma 'drop metastases' along spinal cord
Metastasis: Defining Feature of Malignancy
CLINICAL PEARL
'Skip metastases' and Virchow's node: Regional lymph node involvement usually follows an orderly anatomical sequence — but aggressive tumours can 'skip' regional nodes and appear directly in distant nodes. The classic example is Virchow's node (left supraclavicular lymphadenopathy) from gastric carcinoma — lymphatics from the abdomen drain via the thoracic duct into the left subclavian vein, enlarging the Troisier sign node. A hard, fixed left supraclavicular node in an older patient warrants immediate upper GI endoscopy.
Organ Tropism in Metastasis
Organ Tropism in Metastasis
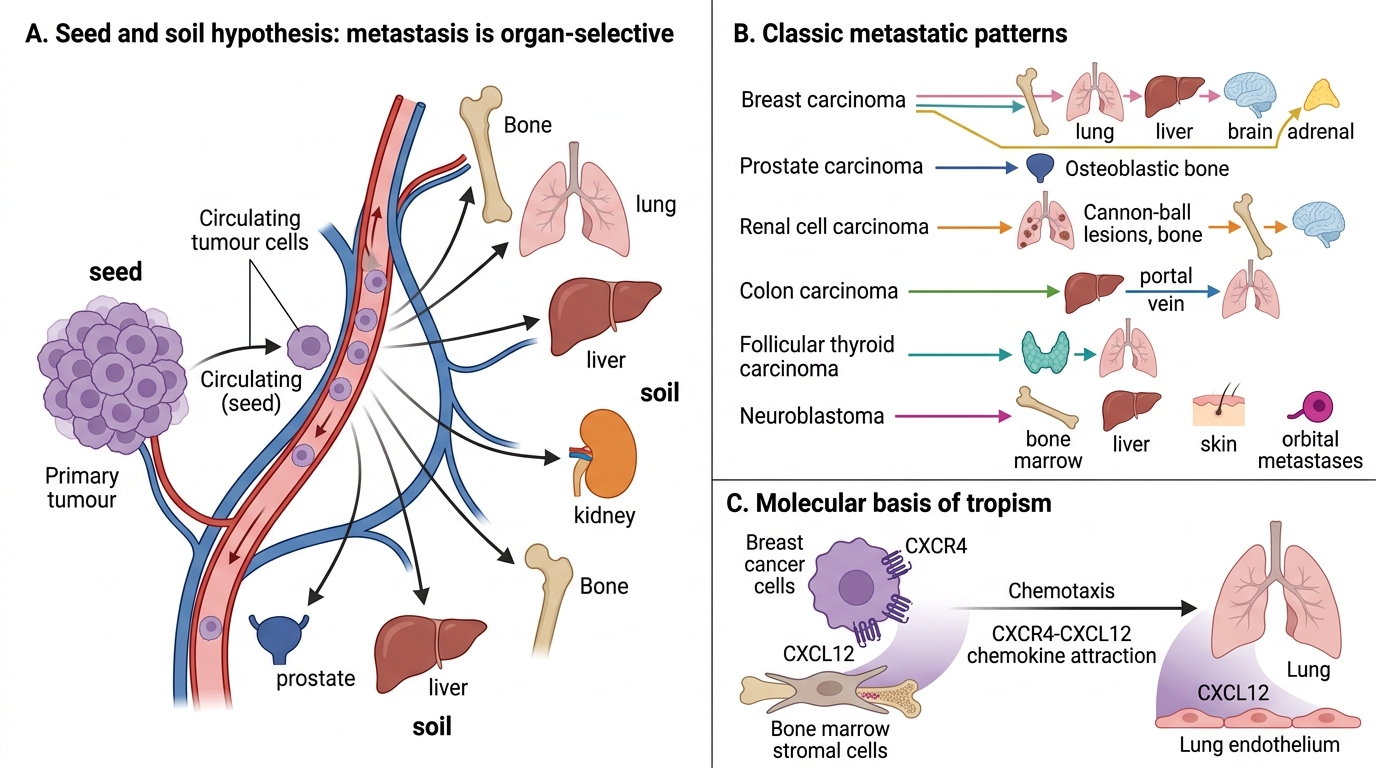
Metastatic deposits do NOT distribute randomly to all organs. 'Seed and soil' hypothesis (Paget, 1889): the tumour cell ('seed') preferentially grows in tissues ('soil') that provide a permissive microenvironment.
Classic organ-tropism patterns:
| Primary tumour | Preferred metastatic site(s) |
|---|---|
| Breast carcinoma | Bone (lytic/blastic), lung, liver, brain, adrenal |
| Prostate carcinoma | Bone (osteoblastic — sclerotic on X-ray) |
| Renal cell carcinoma | Lung ('cannon ball'), bone, brain |
| Colon carcinoma | Liver (via portal vein), then lung |
| Thyroid carcinoma (follicular) | Bone, lung |
| Neuroblastoma | Bone marrow, liver, skin (orbital metastases — 'raccoon eyes') |
Molecular basis: chemokine receptor–ligand pairs (e.g., CXCR4 on breast cancer cells is attracted to CXCL12 abundant in bone marrow and lung endothelium).
SELF-CHECK
A 60-year-old man with known carcinoma of the prostate presents with severe lower back pain. X-ray shows increased bone density (sclerosis) at L3 and L4 vertebrae. Which route of spread is MOST likely responsible?
A. Transcoelomic spread via the peritoneal cavity
B. Haematogenous spread via Batson's vertebral venous plexus
C. Lymphatic spread via para-aortic lymph nodes
D. Direct extension from the rectum
Reveal Answer
Answer: B. Haematogenous spread via Batson's vertebral venous plexus
Prostate carcinoma characteristically spreads to the vertebral column via Batson's vertebral venous plexus — a valveless network that allows retrograde flow from the pelvic veins to the vertebral bodies, bypassing the inferior vena cava and lungs. The osteoblastic (sclerotic) pattern of bone metastasis is also classic for prostate carcinoma (compared to the lytic pattern of most other metastases). Transcoelomic spread is for tumours within body cavities; lymphatic and direct extension would not produce this pattern.
Summary — Benign vs Malignant: The Full Comparison
| Feature | Benign | Malignant |
|---|---|---|
| Differentiation | Well-differentiated; resembles parent tissue | Variable; may be anaplastic |
| Pleomorphism | Minimal | Marked |
| Nuclear changes | Normal N:C ratio; normochromatic | ↑ N:C ratio; hyperchromatic; prominent nucleoli |
| Mitotic figures | Rare; normal | Frequent; atypical forms |
| Growth rate | Slow | Rapid |
| Capsule | Often present | Absent or pseudocapsule with infiltrating margins |
| Local invasion | Non-invasive | Invasive; destroys surrounding tissue |
| Metastasis | Absent | Present (pathognomonic) |
| Recurrence after surgery | Rare | Common |
| Effect on patient | Local pressure effects | Local + systemic effects; cachexia; death if untreated |
Note: Some benign tumours have exceptions (e.g., craniopharyngioma — benign histology, life-threatening location). Clinical context always matters.