Page 10 of 24
PA6.4-6 | Tumour Effects, Immunology & Laboratory Diagnosis — SDL Guide
Learning Objectives
- Describe the local and systemic effects of tumours on the host, including cachexia and paraneoplastic syndromes with their associated tumour types.
- Explain the immunological basis of tumour surveillance, tumour antigen categories (TSA/TAA), and mechanisms by which tumours evade immune destruction.
- Outline the principles and clinical applications of laboratory methods used to diagnose cancer: histopathology, cytology, immunohistochemistry, tumour markers, and molecular techniques.
- Distinguish grading from staging and apply the TNM framework to communicate tumour extent.
INSTRUCTIONS
Cancer is not just a local growth — it reshapes the entire body. A patient with small-cell lung carcinoma may first present with Cushing syndrome; a pancreatic tumour may announce itself through migratory thrombophlebitis. Understanding why these systemic effects occur, how the immune system fights (and loses to) tumours, and how the laboratory confirms the diagnosis are three pillars of clinical pathology you will use every day. This module draws together Cluster G4's final thread — from bedside signs back to the bench.
References
- Robbins & Kumar: Basic Pathology, 11th ed., Ch 6 (Neoplasia) (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 8 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man presents with proximal muscle weakness, moon face, central obesity, and hypertension. Chest X-ray reveals a hilar mass. Serum cortisol is grossly elevated and does not suppress with dexamethasone. His adrenal glands are normal on CT. What is causing Cushing syndrome in a patient without an adrenal or pituitary lesion — and how does this illuminate the systemic reach of a tumour that has not yet spread beyond the thorax?
WHY THIS MATTERS
Paraneoplastic syndromes are under-recognised and frequently misattributed to other causes, delaying cancer diagnosis by months. Tumour markers guide surveillance protocols you will order daily as a clinician. Immunotherapy — built on the science of tumour immunology — has transformed oncology in the past decade. The laboratory workup you order (biopsy type, IHC panel, molecular assay) directly determines treatment eligibility. This module bridges basic pathology to the real clinical decisions that follow a cancer diagnosis.
RECALL
Before starting, confirm you can answer these from Cluster G4 SDL 1 & 2:
- What is the difference between a benign and malignant neoplasm in terms of invasion and metastasis?
- Name two oncogenes and two tumour suppressor genes.
- What does 'differentiation' mean when applied to a tumour?
- List the routes of metastatic spread.
If any of these are uncertain, revisit SDL 1 before continuing — the concepts here build directly on them.
Local Effects of Tumours on the Host
Local Effects of Tumours on the Host
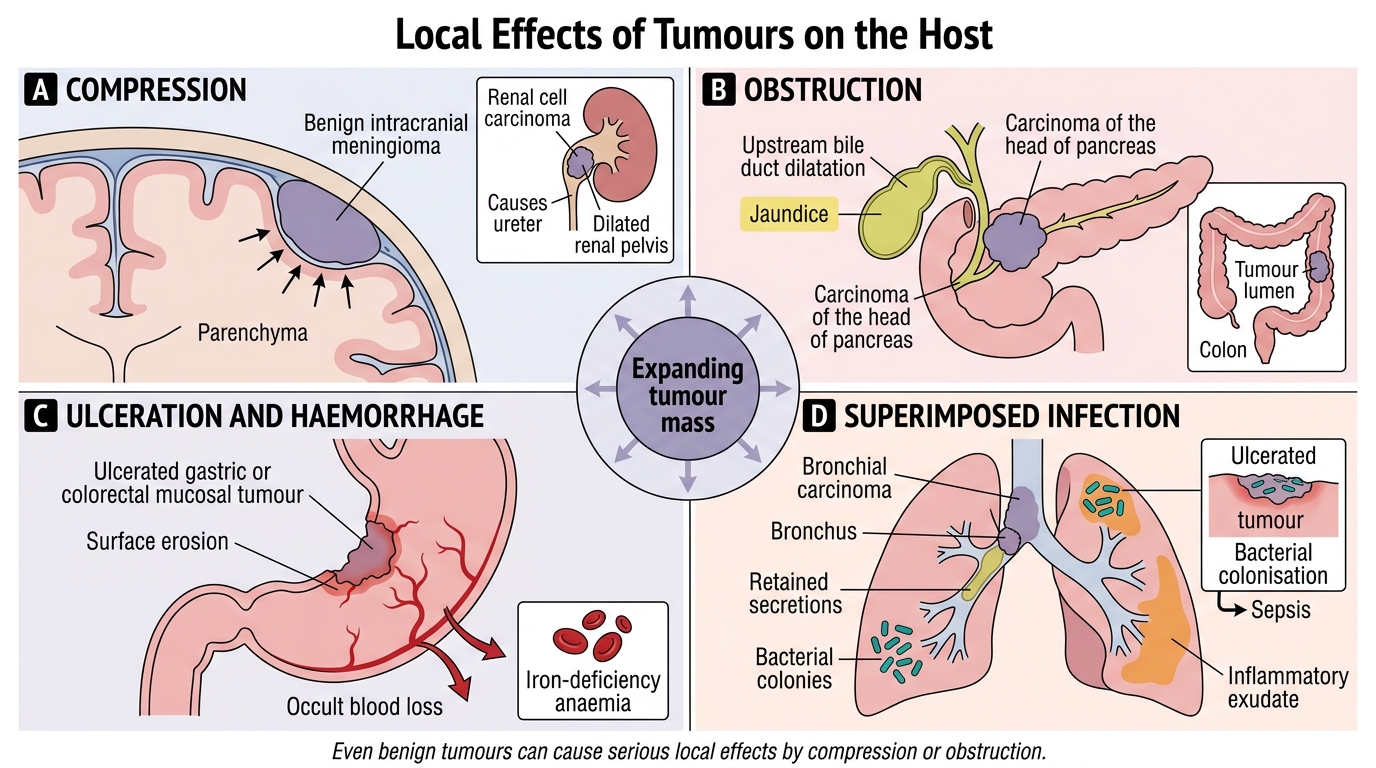
Tumours cause local damage by four main mechanisms:
- Compression: A slowly growing meningioma compresses adjacent brain parenchyma; a renal cell carcinoma compresses the ureter, causing hydronephrosis. Even benign tumours cause serious local compression.
- Obstruction: Carcinoma of the head of pancreas obstructs the common bile duct → obstructive jaundice; carcinoma of the colon obstructs the lumen → large-bowel obstruction.
- Ulceration and haemorrhage: Gastric carcinoma and colorectal carcinoma commonly ulcerate their mucosal surface, leading to chronic iron-deficiency anaemia from occult blood loss, or acute haemorrhage.
- Superimposed infection: Tumour-induced obstruction (bronchial carcinoma blocking a bronchus) creates a stagnant column of secretions — an ideal medium for bacterial pneumonia. Similarly, ulcerated tumours become colonised, causing sepsis in advanced disease.
Ectopic hormone/product secretion by the tumour (discussed under paraneoplastic syndromes) constitutes an additional local-to-systemic bridge.
Cancer Cachexia
Cancer Cachexia: Cytokine-Driven Catabolism
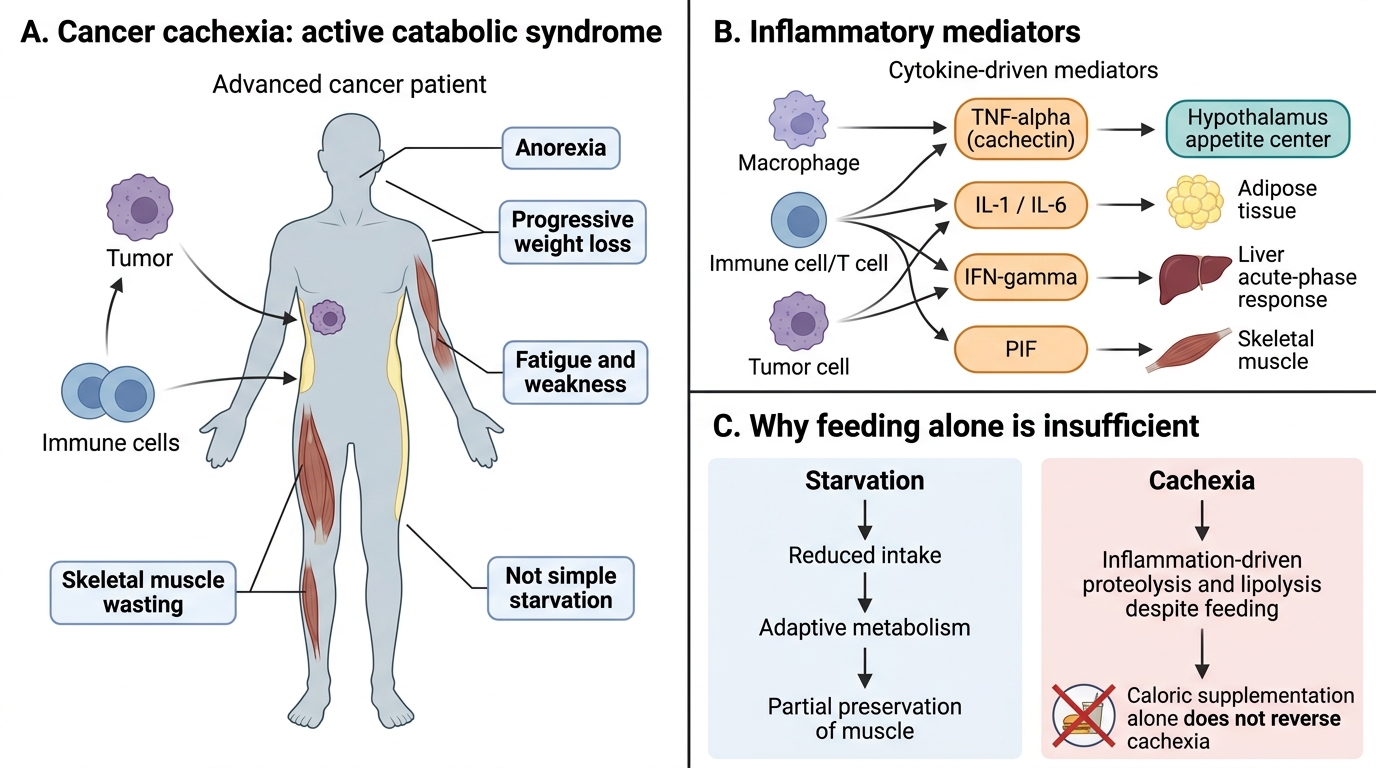
Cachexia is a profound metabolic syndrome characterised by anorexia, progressive weight loss, skeletal muscle wasting, fatigue, and weakness. It affects ~50–80% of advanced cancer patients and is directly responsible for ~20% of cancer deaths — not the tumour itself.
Mediators (cytokine-driven):
| Mediator | Source | Key effect |
|---|---|---|
| TNF-α (cachectin) | Macrophages, tumour | Suppresses appetite (anorexia), promotes lipolysis |
| IL-1, IL-6 | Immune cells | Anorexia, acute-phase response, muscle catabolism |
| IFN-γ | T cells | Amplifies lipolysis and proteolysis |
| Proteolysis-inducing factor (PIF) | Tumour itself | Directly degrades skeletal muscle |
Cachexia is NOT simply starvation — it is an active catabolic process driven by inflammatory mediators. Caloric supplementation alone does not reverse it. Recognising this guides realistic nutritional counselling in oncology.
SELF-CHECK
A patient with advanced colorectal cancer loses 10 kg despite normal caloric intake. Which mediator is MOST responsible for the active muscle wasting seen in cancer cachexia?
A. Erythropoietin
B. TNF-α (cachectin)
C. Aldosterone
D. Thyroxine
Reveal Answer
Answer: B. TNF-α (cachectin)
TNF-α, also called cachectin, suppresses appetite and promotes lipolysis and protein catabolism. Cachexia is cytokine-driven, not merely nutritional, explaining why caloric supplementation alone fails to reverse it.
Paraneoplastic Syndromes
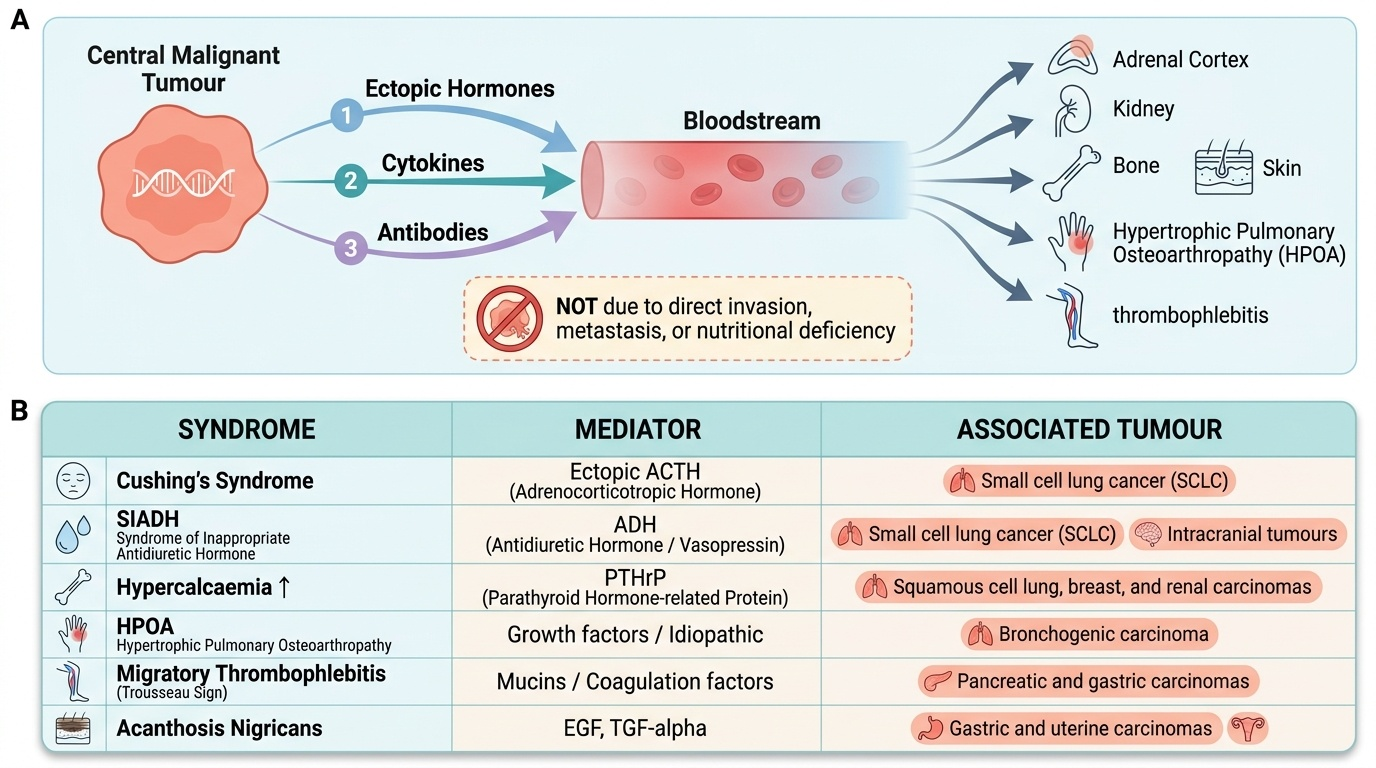
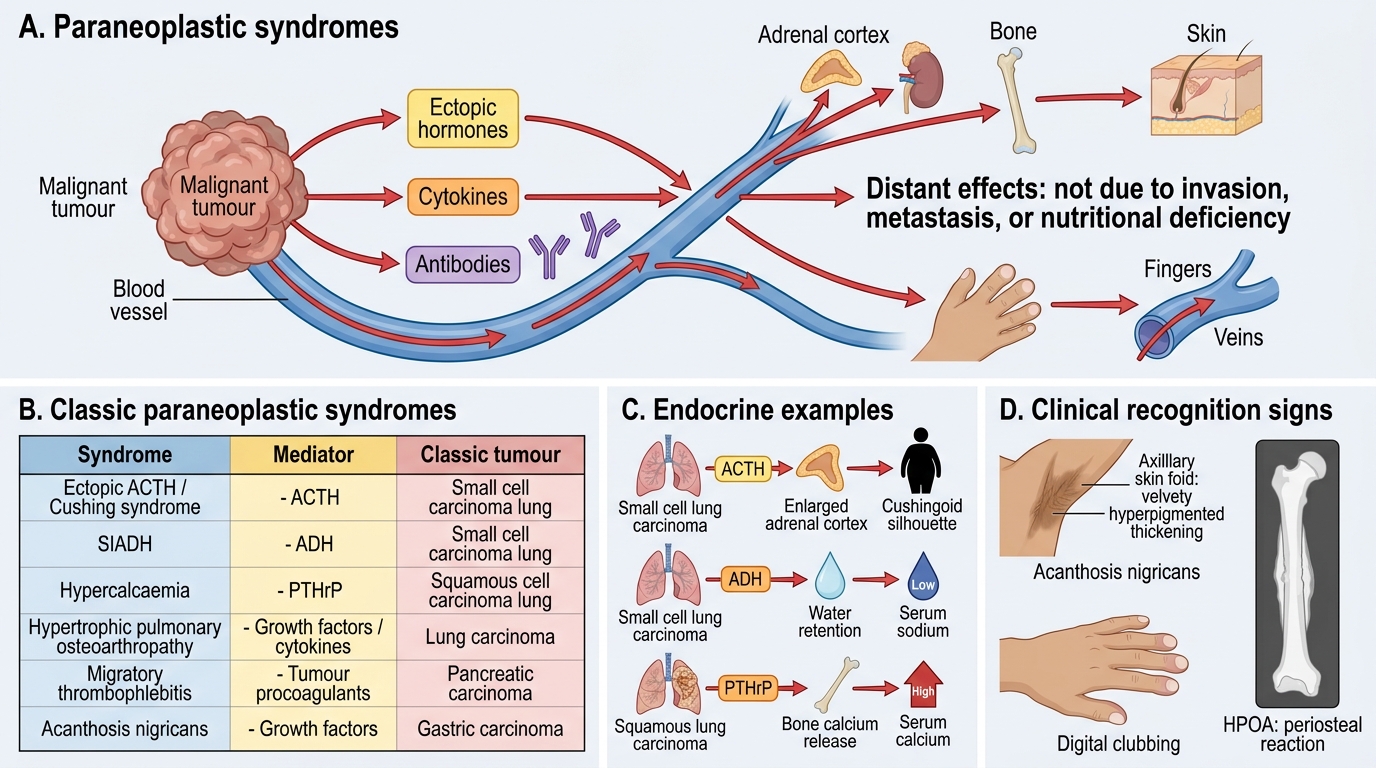
Paraneoplastic syndromes are clinical manifestations caused by tumour products (hormones, cytokines, antibodies) acting at a distance — NOT explained by direct tumour invasion, metastasis, or nutritional deficiency.
Provided image
They are important because:
1. They may be the first clinical presentation of an occult cancer.
2. They may mimic metastatic disease (e.g., hypercalcaemia without bone secondaries).
3. Treating the tumour resolves the syndrome.
Endocrine paraneoplastic syndromes are the most common and result from ectopic hormone production — tumour cells expressing genes normally silent in non-endocrine tissue.
Paraneoplastic Syndromes: Mediators, Tumours, and Clinical Clues
Key endocrine syndromes:
| Syndrome | Mediator | Classic Tumour |
|---|---|---|
| Ectopic ACTH / Cushing syndrome | ACTH-like peptide | Small-cell lung carcinoma |
| SIADH (hyponatraemia) | ADH-like peptide | Small-cell lung carcinoma |
| Hypercalcaemia (no bone mets) | PTHrP (PTH-related protein) | Squamous cell carcinoma of lung, renal cell carcinoma |
| Hypoglycaemia | IGF-2 | Hepatocellular carcinoma, fibrosarcoma |
| Polycythaemia | Erythropoietin | Renal cell carcinoma, hepatocellular carcinoma |
Non-endocrine paraneoplastic syndromes:
- Haematologic: Migratory thrombophlebitis (Trousseau sign — thrombophlebitis in one site resolves and appears elsewhere; classic with pancreatic carcinoma and mucin-secreting adenocarcinomas due to tumour procoagulant factors). Anaemia of chronic disease (many solid tumours).
- Neurologic: Subacute cerebellar degeneration, peripheral neuropathy, Eaton-Lambert syndrome — autoimmune, antibody-mediated.
- Dermatologic: Acanthosis nigricans — velvety, hyperpigmented plaques in axilla/groin; associated with gastric carcinoma and other adenocarcinomas. Dermatomyositis (muscle inflammation + skin rash) — triggers cancer workup in adults >50 years.
- Skeletal: Hypertrophic pulmonary osteoarthropathy (HPOA) — periosteal new bone formation in long bones + finger clubbing; associated with bronchogenic carcinoma.
CLINICAL PEARL
Small-cell lung carcinoma (SCLC) is the paraneoplastic 'overachiever' — it can produce ectopic ACTH (Cushing), ADH (SIADH), and anti-neuronal antibodies (cerebellar degeneration) all in the same patient. SCLC arises from neuroendocrine Kulchitsky cells which retain the capacity to express many peptide-hormone genes. If you see a hilar mass with Cushing syndrome or hyponatraemia, think SCLC until proven otherwise.
SELF-CHECK
A 62-year-old smoker presents with hyponatraemia (Na 118 mEq/L), euvolaemia, and urine osmolality > serum osmolality. Chest CT shows a central lung mass. Which paraneoplastic mechanism is most likely?
A. Ectopic PTHrP secretion by squamous cell carcinoma
B. Ectopic ADH (SIADH) from small-cell lung carcinoma
C. Ectopic ACTH from carcinoid tumour
D. Erythropoietin excess from renal cell carcinoma
Reveal Answer
Answer: B. Ectopic ADH (SIADH) from small-cell lung carcinoma
Euvolaemic hyponatraemia with urine osmolality > serum osmolality is SIADH. Small-cell lung carcinoma is the classic cause via ectopic ADH-like peptide production. PTHrP causes hypercalcaemia (not hyponatraemia) and is associated with squamous cell carcinoma.