Page 13 of 24
PA6.4-6 | Tumour Effects, Immunology & Laboratory Diagnosis — SDL Guide (Part 4)
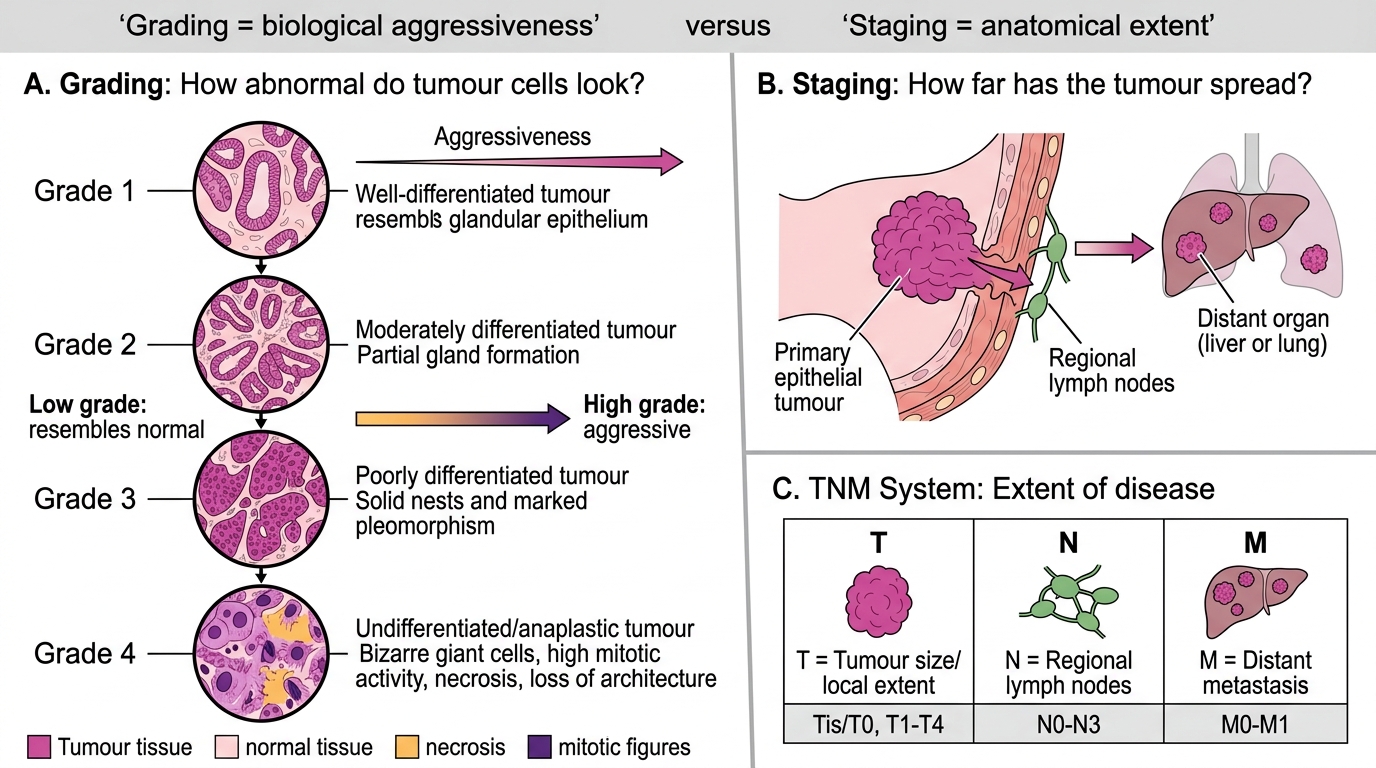
Grading vs Staging — TNM System
Two distinct frameworks communicate very different information about a tumour:
Grading (histological) — how differentiated is the tumour?
- Reflects biological aggressiveness (degree of dedifferentiation, mitotic activity, nuclear pleomorphism, necrosis).
- Determined by the pathologist on biopsy/resection specimen.
- Scale: Grade 1 (well-differentiated) → Grade 3 (poorly differentiated) → Grade 4 (undifferentiated/anaplastic).
- Low grade = more closely resembles normal tissue = less aggressive. High grade = anaplastic = rapidly growing, aggressive.
Staging (clinical/radiological/pathological) — how far has the tumour spread?
- Reflects extent of disease — is it confined to the primary site, lymph nodes, or distant organs?
- Determined by imaging + surgical findings + pathology combined.
- TNM system (AJCC/UICC):
| Component | Assesses | Scale |
|---|---|---|
| T (Tumour) | Size/local extent of primary | T1–T4 (+ Tis = in situ, T0 = no evidence) |
| N (Node) | Regional lymph node involvement | N0 (none) → N1–N3 (increasing involvement) |
| M (Metastasis) | Distant metastasis | M0 (absent) → M1 (present) |
TNM groupings → Stage I–IV:
• Stage I: Small, localised (T1N0M0) — best prognosis.
• Stage IV: Any M1 — distant metastasis — worst prognosis.
Grading vs Staging: TNM System
Practical distinction: A Grade 3 tumour may still be Stage I (small, no spread) and curable with surgery; a Grade 1 tumour may be Stage IV (already metastasised) and incurable. Grading and staging are independent and complementary.
SELF-CHECK
Histopathology of a resected colon tumour shows poorly differentiated adenocarcinoma with marked nuclear pleomorphism. Post-operative staging reveals: tumour invades through the muscularis propria (T3), 4 regional lymph nodes positive (N2), no distant metastasis (M0). What are the correct grade and stage grouping?
A. Grade 1, Stage II
B. Grade 3, Stage III
C. Grade 2, Stage IV
D. Grade 3, Stage IV
Reveal Answer
Answer: B. Grade 3, Stage III
Poorly differentiated = Grade 3 (high grade). T3N2M0 places this tumour in Stage III (regional lymph node involvement, no distant metastasis). Stage IV requires M1 (distant metastasis), which is absent here. This distinction matters: Stage III colon cancer is treated with surgery + adjuvant chemotherapy; Stage IV requires palliative/systemic therapy.
CLINICAL PEARL
The term 'staging laparotomy' — once routine in Hodgkin lymphoma — is largely obsolete since PET-CT provides non-invasive staging. But the concept it embodied (staging must reflect ALL sites of disease) remains essential. A surgeon who grades a tumour 'low' on biopsy but fails to stage it properly may offer curative surgery to a patient who already has micrometastases — a significant under-treatment error.