Page 12 of 24
PA6.4-6 | Tumour Effects, Immunology & Laboratory Diagnosis — SDL Guide (Part 3)
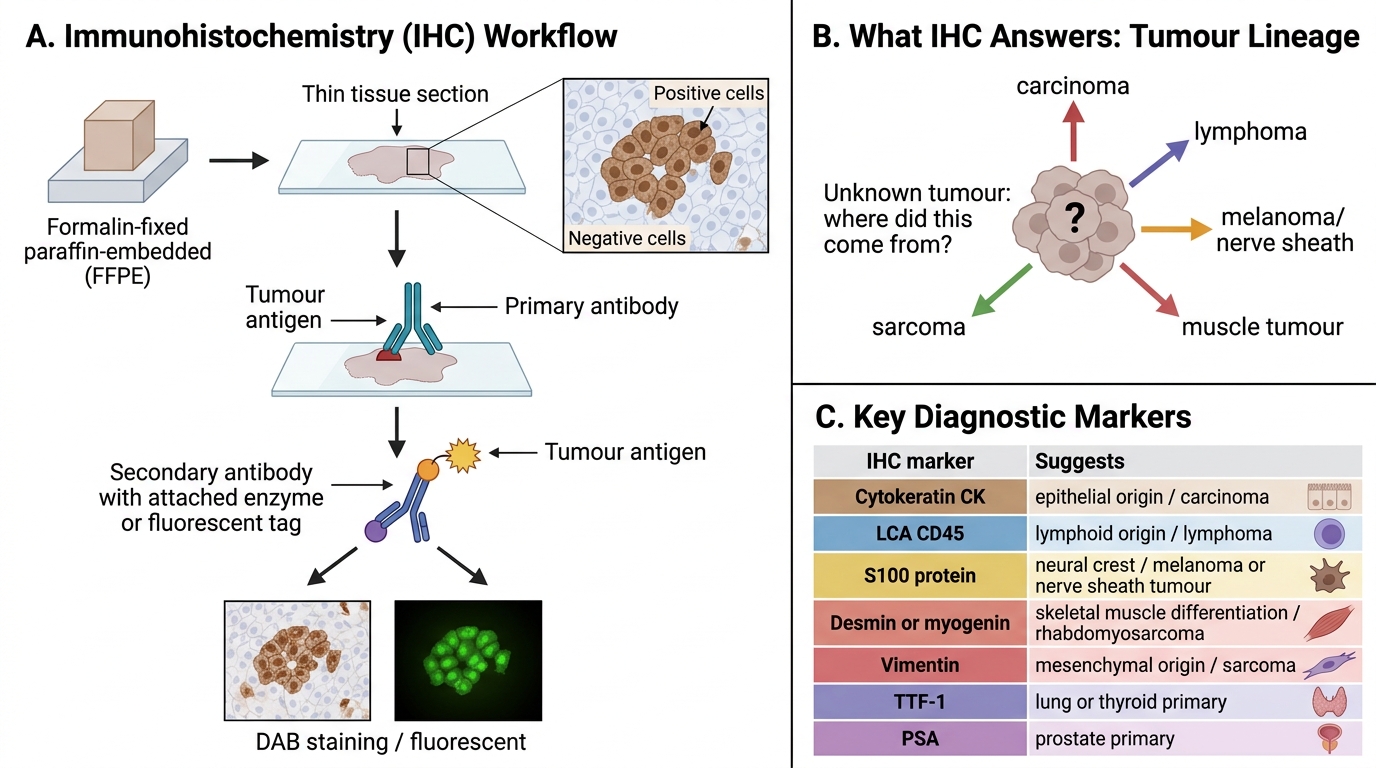
Immunohistochemistry (IHC)
Immunohistochemistry uses specific antibodies applied to formalin-fixed, paraffin-embedded (FFPE) tissue sections to detect antigens in situ. Chromogen (DAB — brown) or fluorescent tag visualises the result.
IHC solves critical diagnostic problems:
- Tumour lineage (where did this come from?):
| Marker | Cell/tumour type identified |
|---|---|
| Cytokeratin (CK) | Epithelial origin (carcinomas) |
| LCA (CD45) | Lymphoid origin (lymphomas) |
| S100 protein | Neural crest — melanoma, nerve sheath tumours |
| Desmin / myogenin | Muscle tumours (rhabdomyosarcoma) |
| Vimentin | Mesenchymal origin (sarcomas) |
| TTF-1 | Lung or thyroid primary |
| PSA | Prostate carcinoma |
- Identifying cancer of unknown primary (CUP): IHC panel (CK7/CK20/TTF-1/CDX2/PSA) narrows the primary site when metastasis presents first.
3. Prognostic/predictive markers that guide therapy:
• ER/PR (oestrogen/progesterone receptor) in breast cancer → eligibility for hormonal therapy.
• HER2 (ERBB2) in breast/gastric cancer → eligibility for trastuzumab.
• Ki-67 — proliferation index; high Ki-67 = aggressive tumour.
• PD-L1 — predicts response to checkpoint inhibitors.
Immunohistochemistry: Detecting Tumour Lineage
SELF-CHECK
A 55-year-old woman presents with a 2-cm lymph node mass. Biopsy shows large atypical cells. IHC reveals: CK-positive, LCA-negative, S100-negative. What is the most likely cell lineage?
A. Lymphoma (B-cell origin)
B. Melanoma (neural crest origin)
C. Carcinoma (epithelial origin)
D. Rhabdomyosarcoma (muscle origin)
Reveal Answer
Answer: C. Carcinoma (epithelial origin)
Cytokeratin (CK) positivity marks epithelial origin — i.e., a carcinoma (likely metastatic). LCA (CD45) positivity would indicate lymphoma; S100 positivity would suggest melanoma or nerve sheath tumour. This IHC profile is classic for metastatic carcinoma in a lymph node.
Tumour Markers
Tumour markers are molecules — proteins, hormones, or enzymes — produced by tumour cells or by the host in response to the tumour, detectable in blood (or other fluids).
Critical principle: Tumour markers are generally NOT reliable for screening (low specificity — raised in benign conditions) but are highly valuable for monitoring treatment response and detecting recurrence after therapy.
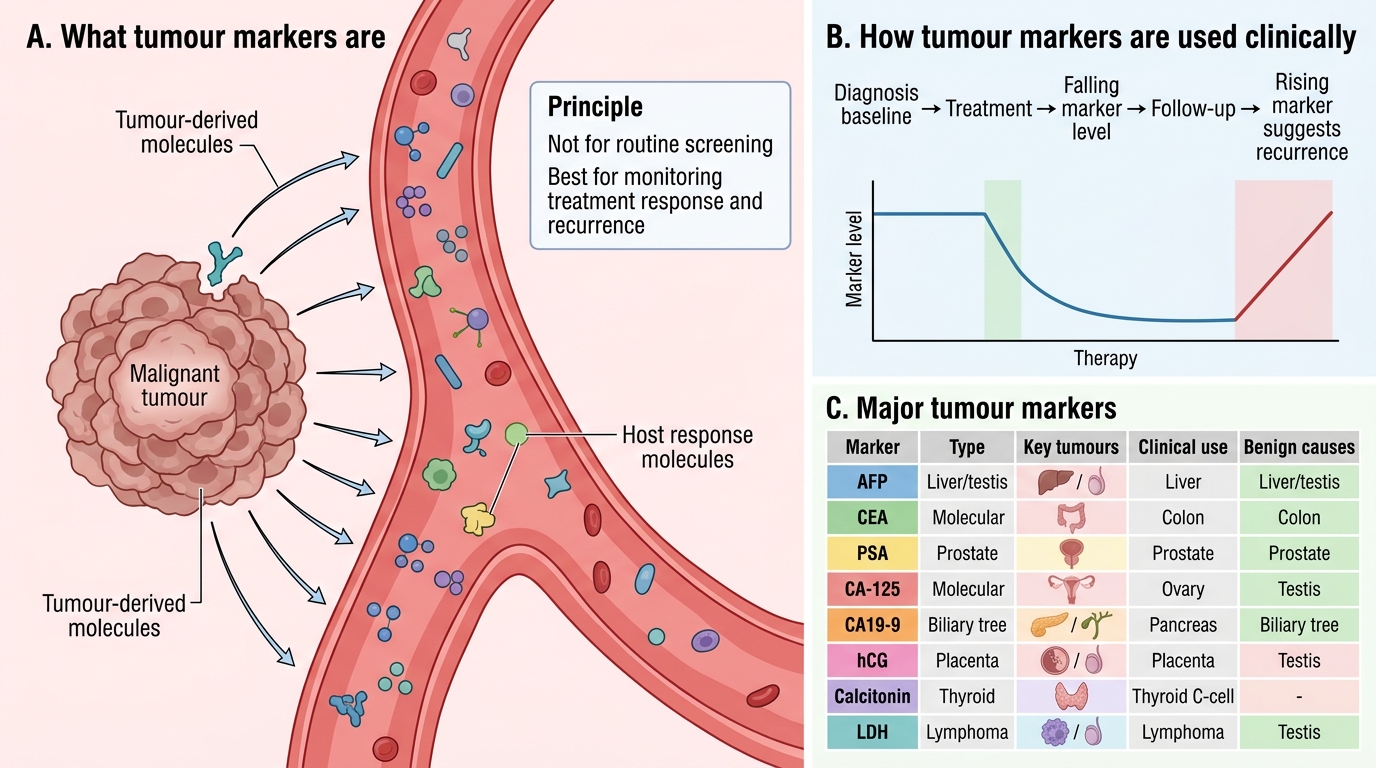
Tumour Markers: Principles and Major Examples
| Marker | Key tumour(s) | Clinical use | Benign causes |
|---|---|---|---|
| AFP (Alpha-fetoprotein) | Hepatocellular carcinoma (HCC); testicular germ cell (non-seminoma) | Diagnosis + monitoring | Hepatitis, cirrhosis; pregnancy |
| CEA (Carcinoembryonic antigen) | Colorectal carcinoma; gastric, pancreatic | Monitoring recurrence post-surgery | Smoking, IBD, cirrhosis |
| PSA (Prostate-specific antigen) | Prostate carcinoma | Screening (controversial) + monitoring | BPH, prostatitis |
| CA-125 | Ovarian carcinoma | Monitoring; second-line screening in high risk | Endometriosis, PID, liver disease |
| CA19-9 | Pancreatic carcinoma; biliary | Monitoring | Pancreatitis, cholangitis |
| β-hCG | Gestational trophoblastic disease; germ cell tumours | Diagnosis + monitoring | Pregnancy |
| Calcitonin | Medullary thyroid carcinoma (MTC) | Diagnosis + screening in MEN2 | — |
| LDH | Lymphoma, leukaemia, testicular | Disease burden / prognosis | Haemolysis, MI, myopathy |
PSA nuance: PSA is organ-specific (prostate), not cancer-specific. Raised in BPH and prostatitis. Its value lies in monitoring post-prostatectomy or post-radiotherapy (undetectable PSA = remission; rising PSA = recurrence).
Molecular and Cytogenetic Diagnosis
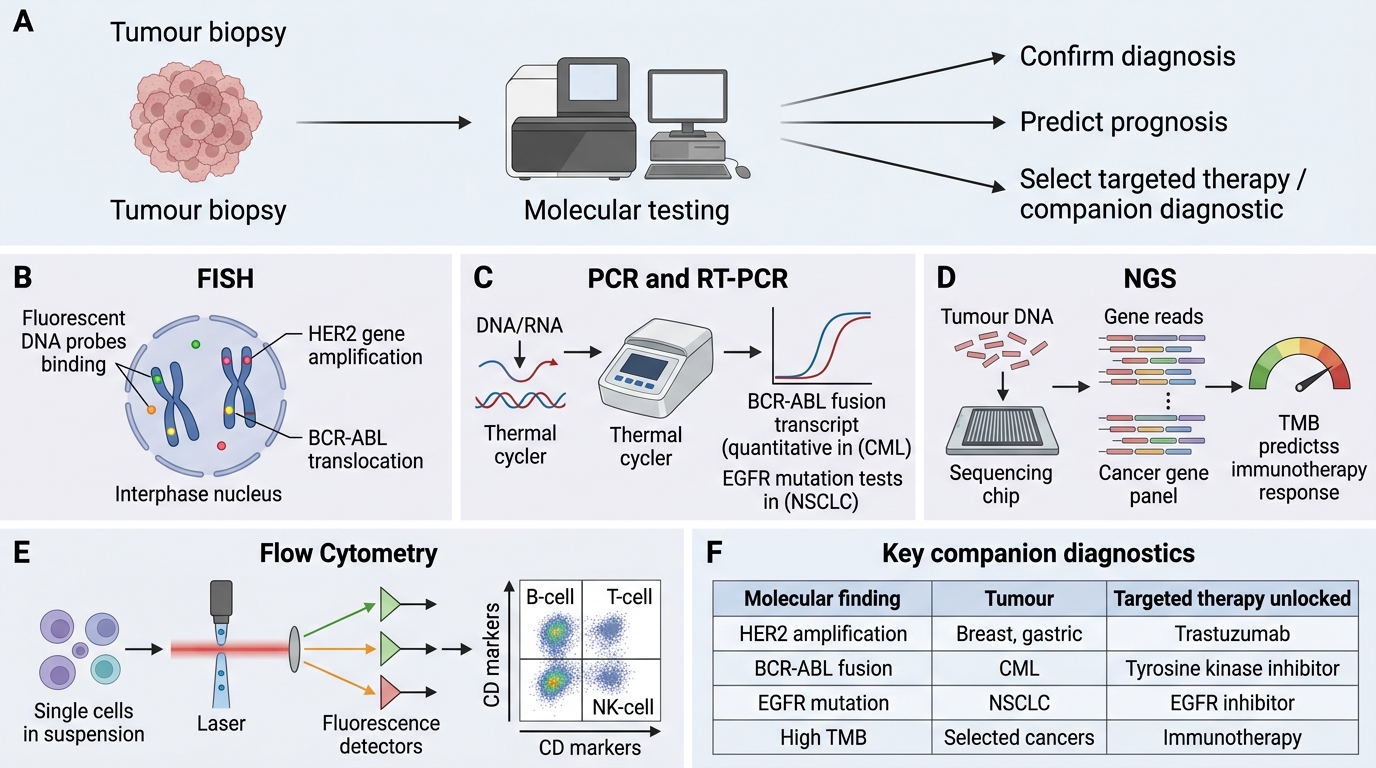
Molecular and Cytogenetic Diagnosis in Neoplasia
Molecular diagnostics identify specific genetic alterations that (a) confirm diagnosis, (b) predict prognosis, and (c) determine eligibility for targeted therapy (companion diagnostics).
Key techniques:
- FISH (Fluorescence In Situ Hybridisation): Fluorescent DNA probes hybridise to specific chromosomal loci on tissue sections or smears. Detects gene amplification (HER2 amplification in breast cancer), translocations (BCR-ABL in CML), and deletions.
- PCR (Polymerase Chain Reaction): Amplifies specific DNA/RNA sequences. RT-PCR detects BCR-ABL fusion transcript (quantitative monitoring in CML); EGFR mutation testing in NSCLC.
- NGS (Next-Generation Sequencing): Simultaneous sequencing of hundreds of cancer-relevant genes. Enables tumour mutation burden (TMB) assessment — predicts response to immunotherapy.
- Flow cytometry: Quantifies surface antigens on cells in suspension (blood, marrow, effusions). Critical for immunophenotyping leukaemias and lymphomas (B-cell vs T-cell vs NK, CD markers).
Key companion diagnostic examples:
| Molecular finding | Tumour | Targeted therapy unlocked |
|---|---|---|
| HER2 amplification | Breast, gastric | Trastuzumab (Herceptin) |
| EGFR mutation | Non-small cell lung (adenocarcinoma) | Erlotinib, gefitinib |
| BCR-ABL (t(9;22)) | CML | Imatinib (Gleevec) |
| BRAF V600E | Melanoma | Vemurafenib |
| PD-L1 expression | Multiple solid tumours | Pembrolizumab |
Molecular testing has shifted oncology from 'site of origin' to 'molecular phenotype' — the same EGFR mutation in lung and colon may respond to the same drug.